


Continuing to Put Ideas into Practice
This is Part 2 of a two-part article on the art of face and neck laceration repair in an acute care setting, emphasizing careful wound closure for the best cosmetic outcome. Part 1 discussed the importance of this topic, a thorough evaluation of the wound with a focus on paying special consideration to facial subunits, and a discussion of various types of suture material characteristics, uses, and considerations.
Wound Anesthesia
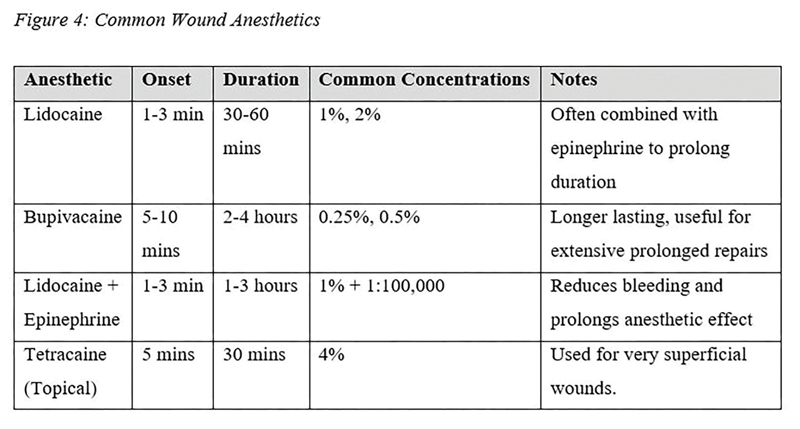
Wound-edge anesthesia is done for the comfort of the patient during the procedure. This can commonly be done with local anesthesia at the wound edges, but it may sometimes require a nerve block. Local wound anesthesia can be achieved by injecting anesthetic medication, such as Lidocaine, into the interior wound edges, directly into the dermis, rather than along intact skin on the exterior of the wound edge. This is most beneficial because it avoids interrupting non-injured tissue around the wound. Sometimes, a topical anesthetic, such as a Lidocaine/Tetracaine mixture, is appropriate for a very superficial wound that may only require minimal repair. (See Figure 4)
Suture Technique
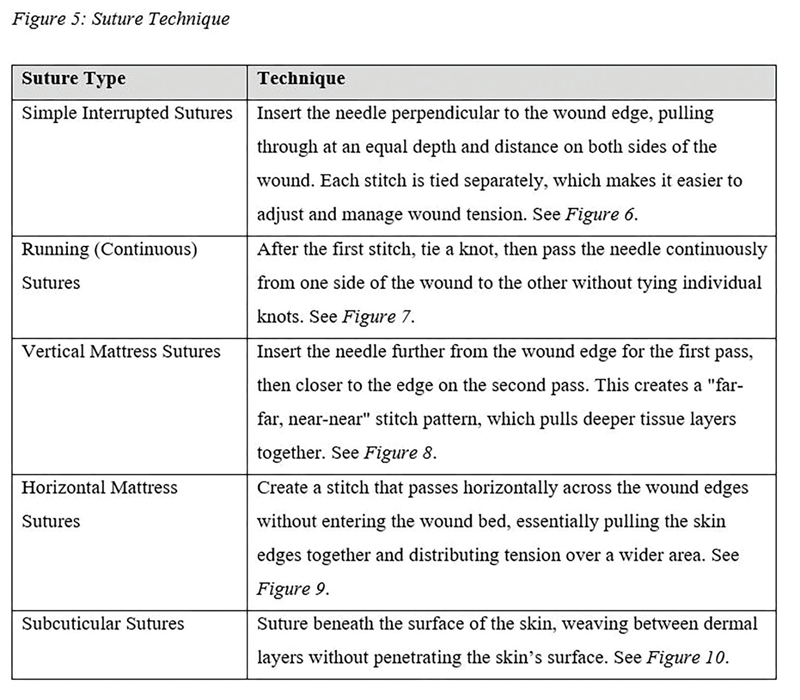
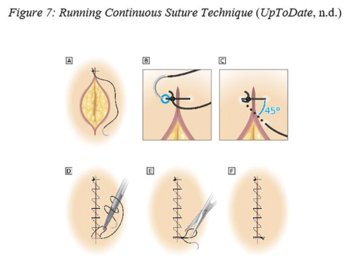
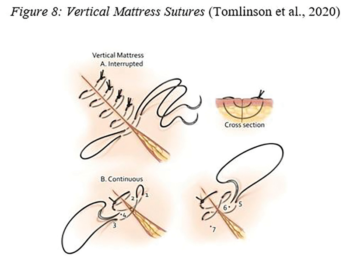
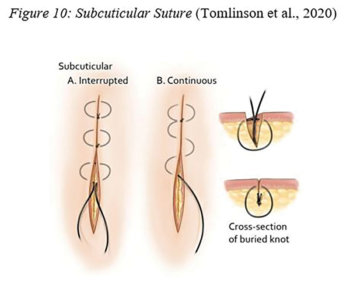
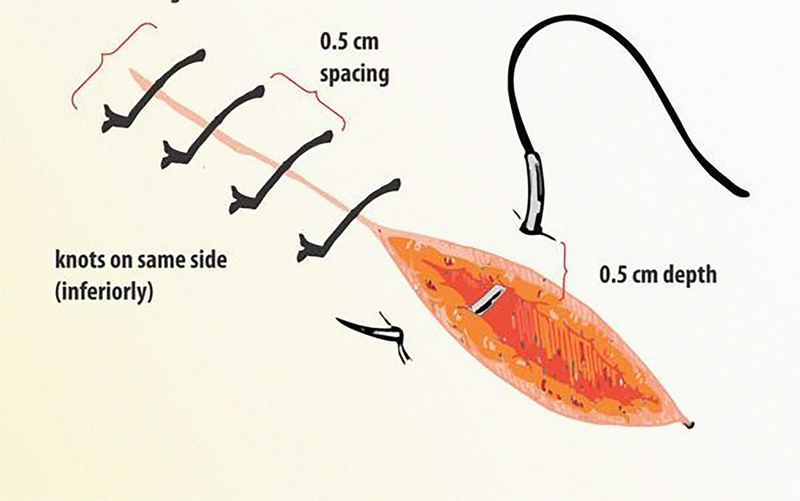
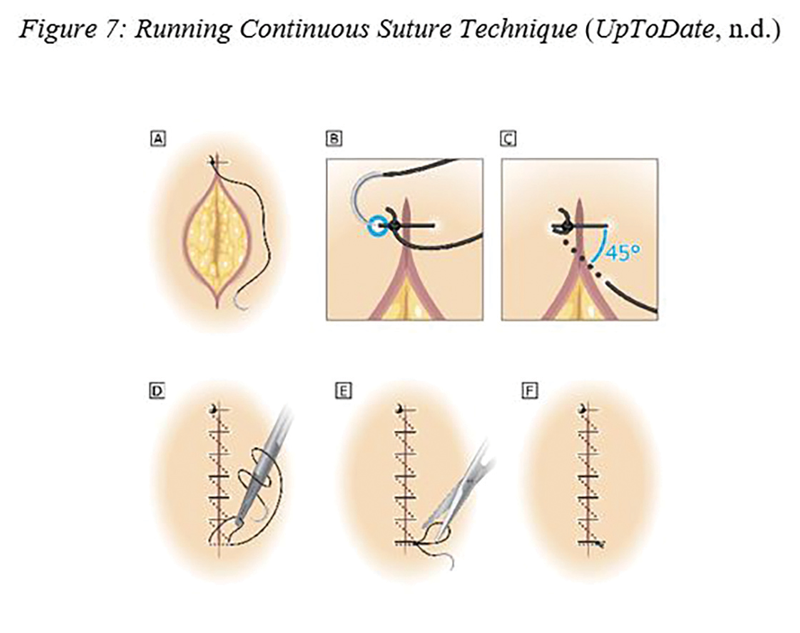
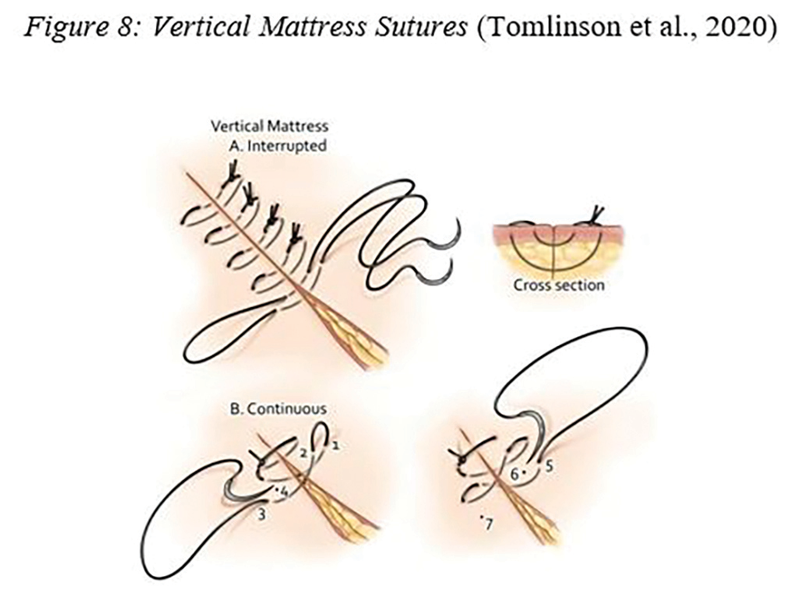
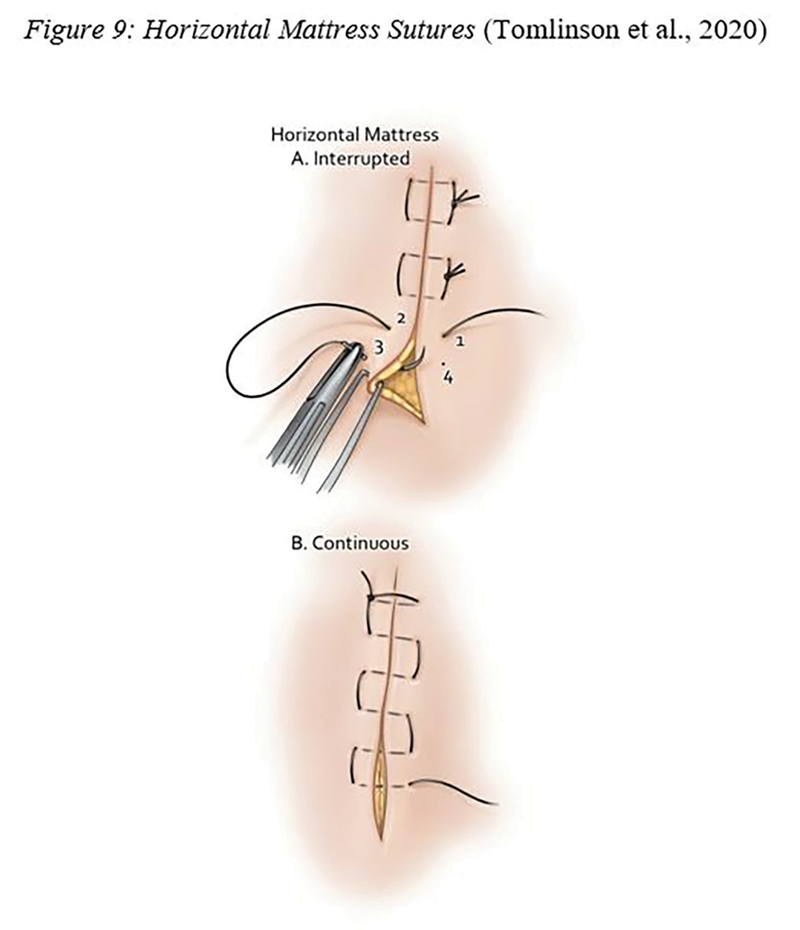
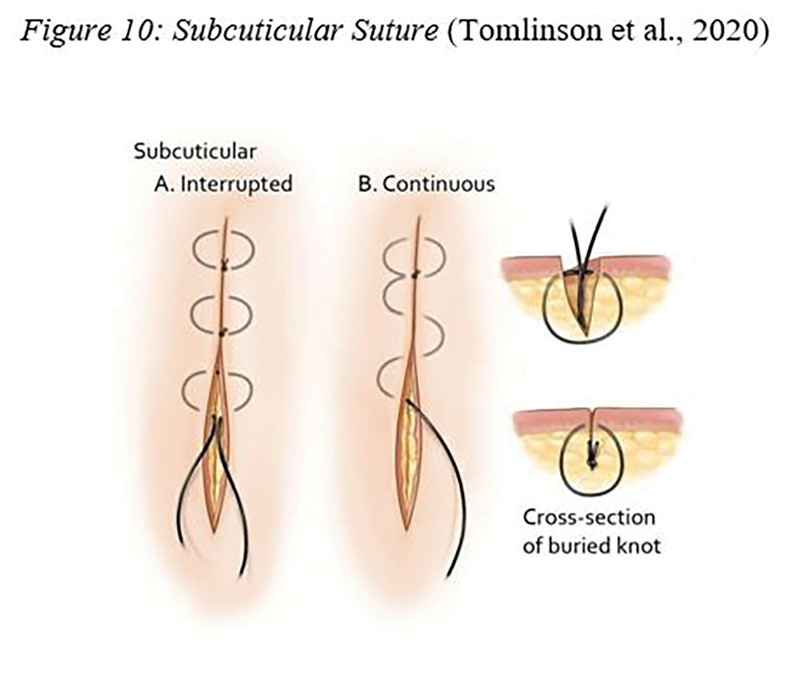
The technique of wound edge eversion, or turning the wound edges outward, is ideal for scar cosmesis. Wound edge eversion refers to the slight upward lifting or tilting of wound edges during closure to optimize healing. When a wound heals, natural tissue contraction can cause the edges to sink inward, creating a depressed scar. Eversion of the wound edges counters this tendency. Special attention should be put to not over-evert the edges as this may cause ridges or dog-ear deformities. Simple interrupted sutures are appropriate for most types of lacerations, including wounds with jagged edges or flaps. Running sutures are ideal for long linear wounds that require a lot of suture material. This allows for less time spent on knot tying and ease of removal. There are two suturing techniques that are used for deeper wounds under tension: vertical and horizontal mattress. A vertical mattress helps evert the wound edges for better healing and is particularly useful in high-tension areas. A horizontal mattress provides excellent tension relief and minimizes the risk of wound-edge ischemia, which can be crucial in cases where tissue is delicate, such as the face and neck. Lastly, there is the subcuticular suture technique. This is ideal for cosmetic closure, especially on the face or areas with low tension. This technique results in a low-profile scar and reduces the risk of stitch marks, and especially useful if cosmetic appearance is a priority. These techniques provide versatility for various types of wound closures, which can significantly improve patient outcomes in a rural emergency setting.

Suture Removal and Long-Term Scar Management
Facial and neck laceration repairs should be seen 5-7 days post-repair for suture removal. This time increment is chosen to reduce track marks from the suture material at the optimal stage of wound healing for the best cosmetic outcome for the patient (Marks et al., 2017).
It is important to discuss long-term scar management with patients. Sun exposure can significantly impact the healing and appearance of laceration scars. This is even more important on regularly sun-exposed skin and in highly visible areas of the face and neck. Proper management is crucial to minimize adverse effects and promote optimal healing. Immature scars, when exposed to UV light, may darken or hyperpigment the laceration line. It is important to counsel patients on sun protection with a hat or clothing and SPF 30 for at least 1 year after laceration repair. There are also commercial products, like patches and creams, specifically designed to improve scarring.
Considerations
It is essential to recognize that face and neck lacerations can be complex and intimidating to a novice rural provider. One must also recognize that not all facial and neck areas will have a good cosmetic outcome. As a provider, one must do the best job possible with wound management given the wound location, size, and amount of tissue lost. Sometimes no matter how well the provider plans the reconstruction, the wash out of the wound, the consideration of suture material and technique, repair, and a good follow-up plan, the patient can still have a poor outcome. Whether that is in regards to unexpected infection, suture material incompatibility, or post-discharge wound care, there are some things that are out of the control of the provider and the patient. Keeping the pearls learned here may help mitigate this in the future.
Conclusion
Cosmetic wound repair of the face and neck requires a meticulous approach to optimize both functional and aesthetic outcomes. Access to specialized consultation, like Plastic Surgery or Ear, Nose, and Throat Surgery, may be limited or unavailable. Postoperative care, including proper wound hygiene, choice of suture type and technique, and sun protection, are essential for optimal healing. By combining evidence-based surgical techniques with prompt follow-up, and diligent aftercare, rural providers can achieve favorable results that restore both form and confidence for the patient. With these pointers, after the initial bleeding is controlled, the rural urgent and emergent provider can take a breath and effectively assess the wound for closure through a more cosmetic lens.






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
1 Comment. Leave new
Short and very Informative.