

Introduction
Postoperative nausea and vomiting (PONV) are common consequences of anesthesia and occur in approximately 30-80% of patients, depending on the surgical procedure and type of anesthetic provided (Elvir-Lazo et al., 2020). Nausea and vomiting contribute significantly to patient dissatisfaction and surgical complications, such as aspiration, wound dehiscence, dehydration, and electrolyte disturbances (Nagelhout, 2018). These factors can prolong patients’ lengths of stay and increase costs associated with additional requirements for medication and management (Hiraki et al., 2022). Proper screening, adequate prophylaxis, use of regional anesthesia, and administering total intravenous anesthesia (TIVA) are strategies known to reduce PONV symptoms. There are, however, instances when these techniques are not sufficient and the patient experiences PONV in the recovery room. Aromatherapy has demonstrated effectiveness in reducing PONV when other remedies have failed.
During the COVID-19 pandemic, aromatherapy at a tertiary care hospital in Maryland was discontinued due to the virus’s unknown mode of transmission. After the end of the pandemic, aromatherapy was never reinstated because the supply of aromatic inhalers could not be maintained due to the inhalers’ high cost, thereby eliminating this nonpharmacologic method of managing PONV symptoms at this facility. Currently, after the administration of prophylactic medication during the preoperative and intraoperative periods, postoperative management in the hospital’s Post Anesthesia Care Unit (PACU) is limited to rescue pharmacologic therapy.
The purpose of this quality improvement (QI) project was to reinstate the hospital’s practice of aromatherapy utilizing bulk peppermint essential oil for colorectal surgical patients in the PACU and to monitor nurses’ adherence to the clinical practice. The process goal was to achieve 100% compliance of aromatherapy administration to PACU patients experiencing PONV. Peppermint oil was selected for this project due to its effectiveness in relieving symptoms of PONV and other gastrointestinal conditions, such as irritable bowel syndrome (Alammar et al., 2019).
Background
Essential oils have previously been demonstrated as an effective treatment for postoperative nausea and vomiting. Ginger, lavender, and peppermint oil inhalation significantly reduced the incidence and severity of PONV symptoms in the PACU (Amirhosseini et al., 2020; Karaman et al., 2019; Maghami et al., 2020). Females exposed to cardamom aromatherapy after Cesarean section experienced less nausea and reduced retching (Khatiban et al., 2022). Clary sage aroma reduced nausea in patients undergoing percutaneous nephrolithotomy (Amirhosseini et al., 2020). Additionally, the authors of a more recent systematic review have found that inhalational aromatherapy in the perioperative period reduces blood pressure, heart rate, and the patient’s perceived level of pain (Biachi et al., 2025).
Similarly, peppermint oil aromatherapy significantly reduced nausea in ambulatory surgical patients who underwent general anesthesia (Brown et al., 2018). A combination of ginger and peppermint oils decreased the number of rescue antiemetics administered to ambulatory surgical patients (Fearrington et al., 2019). Peppermint oil has also been shown to reduce PONV in patients undergoing open heart surgery (Pashaei & Akyuz, 2024). Literature supports the use of aromatherapy using various inhalation techniques (inhalers, gauze, clips, etc.) to relieve PONV symptoms in various patient populations. Some studies demonstrate a reduction in rescue antiemetics administration (Fearrington et al., 2019; Karaman et al., 2019). Overall, the strength and quality of available evidence supported the implementation of aromatherapy in the PACU.
Methods
The facility performs approximately 1,300 colorectal surgeries annually. Patients typically recover in the PACU unless intensive care is needed. Prior to the COVID-19 pandemic, aromatic inhalers were introduced for patients experiencing postoperative nausea and vomiting (PONV), but use was halted due to unknown viral transmission and later discontinued due to cost concerns. Seeking a cost-effective alternative, the Enhanced Recovery After Surgery (ERAS) committee and PACU leadership reintroduced aromatherapy using peppermint oil. The PACU’s 43 nurses, responsible for implementing the intervention, received education and followed a new administration protocol. Supplies such as gauze, disposable cups, and peppermint oil were provided by the unit and ERAS committee.
Upon arrival in the PACU, patients are assessed for PONV using the post-anesthesia recovery score (PARS) documented in the electronic health record (EHR). Nurses record “controlled” if no symptoms are present or “further intervention required” if PONV occurs, typically followed by ondansetron administration. However, guidelines advise against repeating the same antiemetic class within six hours, risking prolonged symptoms.
The 15-week project followed an approved protocol: nurses prepared vpeppermint aromatherapy materials, instructed patients to inhale the aroma, and documented administration in the EHR. Project goals were reinforced through emails and staff engagement.
As no validated compliance tool exists, a REDCap-based EHR audit tool was developed to track aromatherapy use and ensure accurate data collection. The project received quality improvement approval from both the University of Maryland Baltimore and the sponsoring hospital’s Internal Review Board.
Results
Enrollment
Throughout the 15-week implementation period, 47 patients met inclusion criteria and were included in this QI project. Frequencies and percentages of the three nominal variables (administration of aromatherapy, development of PONV, and administration of rescue antiemetics) are displayed in Table 1. Eighteen colorectal surgical patients (38%) received aromatherapy. While 39 patients remained free of PONV symptoms, eight colorectal surgical patients (17%) experienced PONV. The project’s outcome goal was not attained because the rate of PONV among colorectal patients did not decrease by 25%. Instead, compared to the PONV data from September 2022 to December 2022, the rate of PONV in this patient population experienced a significant increase.
Table 1. Frequency Table for Eligible Colorectal Surgical Patients Admitted to the PACU During Each Week of Implementation (n=25)
Compliance
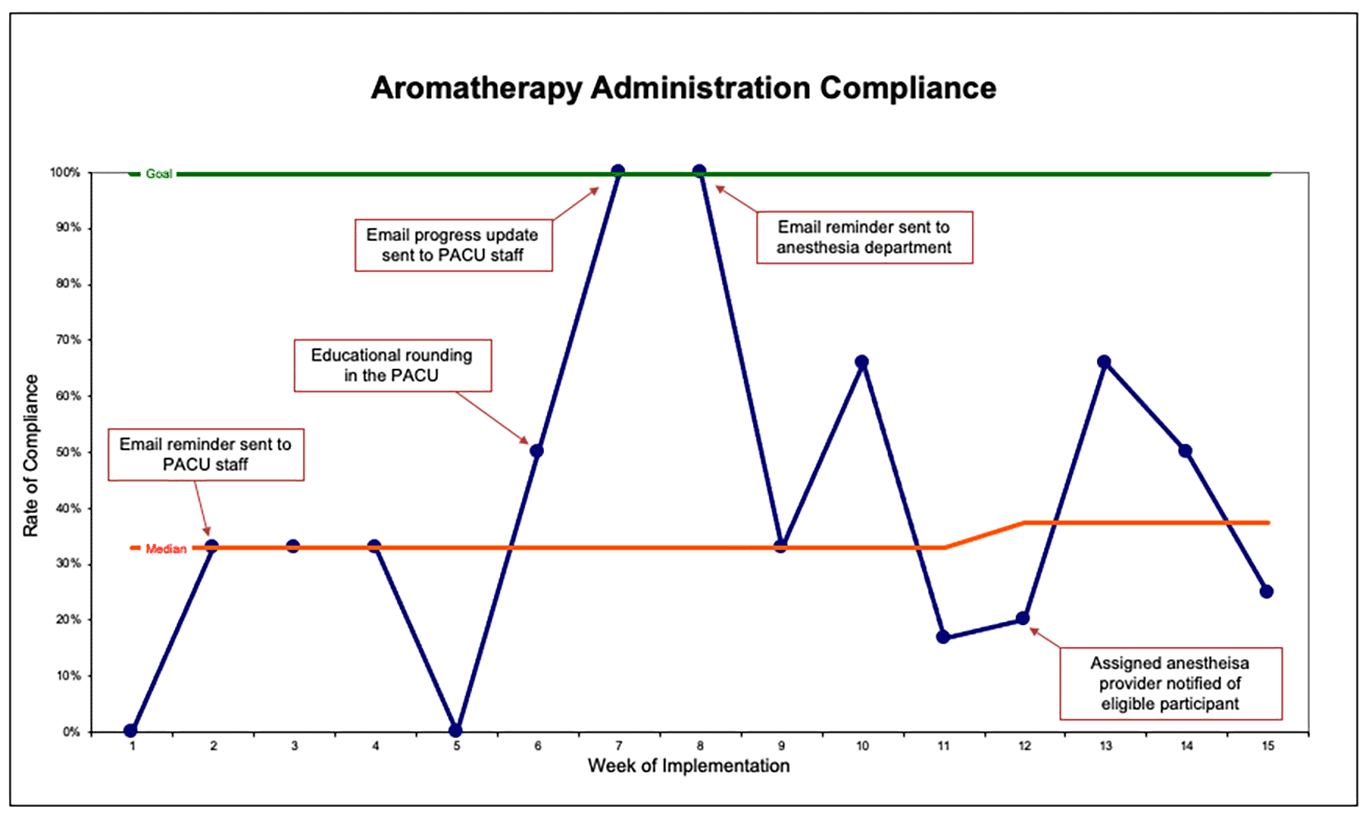
The PACU nurses’ compliance rate in administering aromatherapy ranged from 0% in weeks one and five to 100% in weeks seven and eight. From weeks one through eleven, the median aromatherapy administration compliance was 33%, but during week 12 through the completion of the project, the median compliance increased to 38%.
Outcome
The run chart in Figure 1 shows the weekly PONV rate over the implementation period. The PONV rate ranged from 0% to 50%. During weeks one through eleven, the median PONV rate was 0%, but from weeks 12 through 15, the median rate increased to 37%. No shifts, trends, or astronomical points are observed in this run chart. Based on these results, aromatherapy administration did not have a meaningful impact on the rate of PONV during this project. Instead, the increased PONV rate was likely the result of inadequate prophylaxis or other surgical- or anesthesia-related factors.
Although run chart analyses did not reveal significant changes during this project’s implementation; interventions, such as email reminders to PACU and anesthesia staff and educational rounding, increased compliance (Figures 1 & 2). Unexpected benefits of this project were high levels of patient and PACU nurse satisfaction with the aromatherapy intervention.
Figure 1. Run Chart Displaying Outcome Measure (PONV Rate in Colorectal Surgical
Patients)
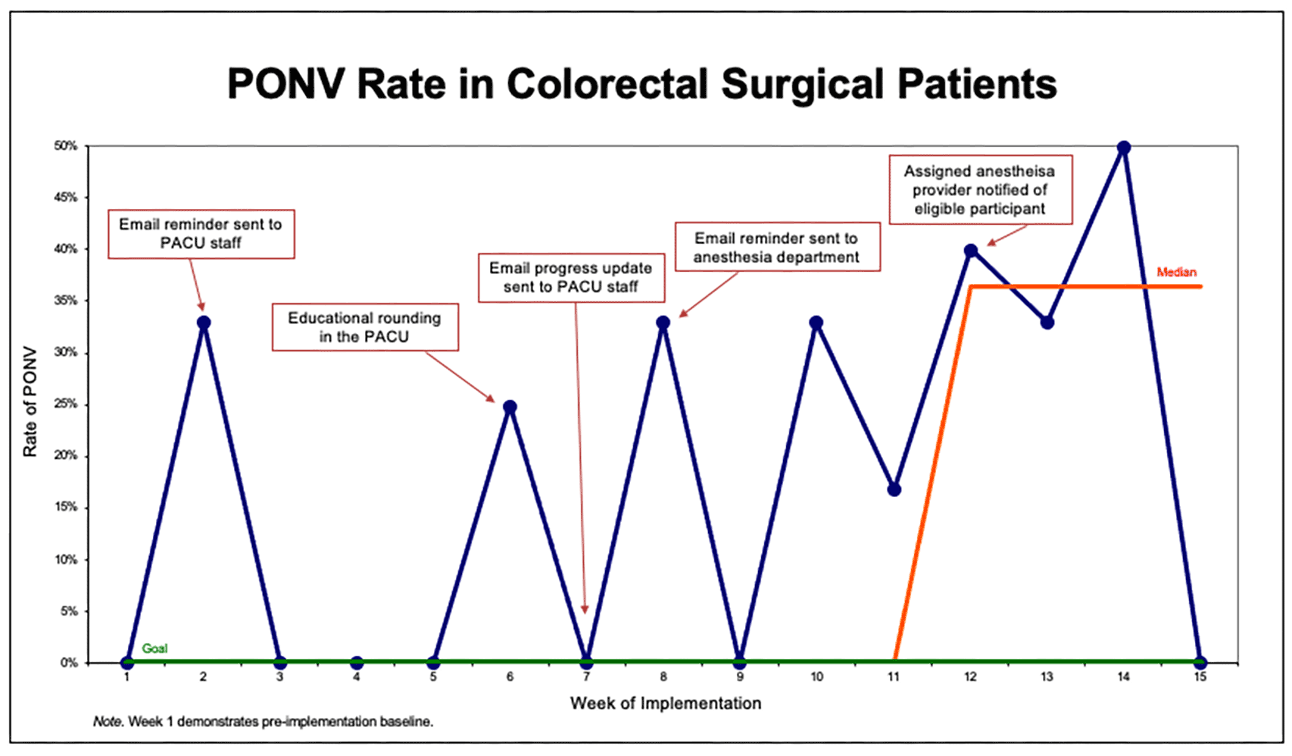
Figure 2. Run Chart Displaying Process Measure (Aromatherapy Administration Compliance)
Discussion
Although the project’s process and outcome measures were not met, an aromatherapy administration protocol and supplies were successfully implemented for colorectal surgical patients recovering in the PACU and the administration compliance rate increased throughout implementation. Frequent evaluation and interventions, as documented in Figures 1 and 2, proved beneficial in improving the compliance rate. Despite the increase in compliance, the rate of PONV among colorectal surgical patients increased during the implementation period. This is likely related to the short implementation period and the increase in eligible participants during the last five weeks of the implementation period.
Despite the project’s results, nurses reported satisfaction with aromatherapy, noting its ease of use and pleasant scent. They shared that patients frequently found the aroma calming. The intervention contributed to a more soothing recovery environment.
Financial Implications
Financial analysis reveals that aromatherapy is cost-effective. Evidence shows that aromatherapy, utilizing bulk oil, is effective in managing PONV symptoms (Amirhosseini et al., 2020; Karaman et al., 2019). Two 16-ounce bottles of peppermint oil were purchased for $45. The oil is highly concentrated, so only a few drops are needed to produce a sufficient aroma. This essential oil supply will suffice for hundreds of patients who wish to participate in aromatherapy.
Barriers
Factors that may have limited the validity of the result include inconsistency in documentation and instances of simultaneous administration of aromatherapy and rescue antiemetics. Data collection relied on PACU nurses to document the intervention. Bedside nurses are overburdened with documentation as requirements continue to increase (Gesner et al., 2022). Patients may have received aromatherapy, but because there was no documentation in the EHR, administration went unrecognized and was not accounted for in data analysis. Another limitation encountered during the project’s implementation was patients’ levels of sedation during their PACU stays. Intraoperative anesthetic management for colorectal surgery patients at the site includes long-acting intravenous infusions. Patients often arrive to the PACU sedated, which limited participation in aromatherapy.
Conclusion
Results from this project suggest that the effectiveness of aromatherapy on PONV symptoms remains inconclusive. However, the findings underscore its value as a simple, low-cost, and well-tolerated intervention that can complement pharmacologic management. Aromatherapy has the potential to enhance patient comfort and satisfaction and may contribute to improved PONV outcomes. While generally safe, appropriate patient assessment remains essential to ensure suitability. Although not a substitute for rescue antiemetics, offering aromatherapy alongside pharmacologic therapy appears to be a reasonable and patient-centered approach. Additional research is warranted to further evaluate its effectiveness across diverse clinical settings.
References
Alammar, N., Wang, L., Saberi, B., Nanavati, J., Holtmann, G., Shinohara, R. T., & Mullin, G. E. (2019). The impact of peppermint oil on the irritable bowel syndrome: A meta-analysis of the pooled clinical data. BMC Complementary and Alternative Medicine, 19(1), 21. https://doi.org/10.1186/s12906-018-2409-0
Amirhosseini, M., Dehghan, M., Mangolian, S. P., & Pakmanesh, H. (2020). Effectiveness of aromatherapy for relief of pain, nausea, and vomiting after percutaneous nephrolithotomy: A randomized controlled trial. Complementary Medicine Research, 27(6), 440–448. https://doi.org/10.1159/000508333
Brown, L., Danda, L., & Fahey, I. T. J. (2018). A quality improvement project to determine the effect of aromatherapy on postoperative nausea and vomiting in a short‐stay surgical population. AORN Journal, 108(4), 361–369. https://doi.org/10.1002/aorn.12366
Biachi, F. B., de Oliveira Faria, M. F., Oliveira, R. A., de Brito Poveda, V., & Rizzo Gnatta, J. (2025). Effect of Aromatherapy for Postoperative Pain Management in the Postanesthesia Recovery Room: A Systematic Review. Journal of Perianesthesia Nursing. https://doi.org/10.1016/j.jopan.2024.09.011
Elvir-Lazo, O. L., White, P. F., Yumul, R., & Cruz Eng, H. (2020). Management strategies for the treatment and prevention of postoperative/postdischarge nausea and vomiting: An updated review. F1000Research, 9(983), 1-25. https://doi.org/10.12688/f1000research.21832.1
Fearrington, M. A., Qualls, B. W., & Carey, M. G. (2019). Essential oils to reduce postoperative nausea and vomiting. Journal of Perianesthesia Nursing, 34(5), 1047–1053. https://www.jopan.org/article/S1089-9472(19)30064-4/abstract
Gan, T. J., Belani, K. G., Bergese, S., Chung, F., Diemunsch, P., Habib, A. S., Jin, Z., Kovac, A. L., Meyer, T. A., Urman, R. D., Apfel, C. C., Ayad, S., Beagley, L., Candiotti, K., Englesakis, M., Hedrick, T. L., Kranke, P., Lee, S., Lipman, D., … Philip, B. K. (2020). Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesthesia and Analgesia, 131(2), 411–448. https://doi.org/10.1213/ANE.0000000000004833
Gesner, E., Dykes, P. C., Zhang, L., & Gazarian, P. (2022). Documentation burden in nursing and its role in clinician burnout syndrome. Applied Clinical Informatics, 13(5), 983–990. https://doi.org/10.1055/s-0042-1757157
Hiraki, M., Tanaka, T., Koga, M., Miura, D., Sadashima, E., Sato, H., Mitsumizo, S., & Kitahara, K. (2022). A clinical risk analysis of postoperative nausea and vomiting after colorectal cancer surgery. Journal of Coloproctology, 42(3), 203-209. https://www.scielo.br/j/jcol/a/4cQkTvJBq3GrSW8vczLQ3Lz/
Karaman, S., Karaman, T., Tapar, H., Dogru, S., & Suren, M. (2019). A randomized placebo-controlled study of aromatherapy for the treatment of postoperative nausea and vomiting. Complementary Therapies in Medicine, 42, 417–421. CINAHL. https://doi.org/10.1016/j.ctim.2018.12.019
Khatiban, M., Mirzaie, M., Fazeli, A., Tapak, L., & Khalili, Z. (2022). Effect of cardamom inhalation therapy on intra-and postoperative nausea and vomiting of mothers undergoing spinal anesthesia for elective Cesarean section. Journal of Perianesthesia Nursing, 37(4), 452–457. https://doi.org/10.1016/j.jopan.2021.09.008
Maghami, M., Afazel, M. R., Azizi-Fini, I., & Maghami, M. (2020). The effect of aromatherapy with peppermint essential oil on nausea and vomiting after cardiac surgery: A randomized clinical trial. Complementary Therapies in Clinical Practice, 40, 1-7. https://doi.org/10.1016/j.ctcp.2020.101199
Nagelhout, J. J. (2018). Chapter 14: Additional drugs of interest. In J. J. Nagelhout & S. Elisha (Eds.), Nurse anesthesia (6th ed., pp. 190-200). Elsevier, Inc.
Pashaei, S., & Akyüz, N. (2024). Effective role of aromatherapy in reducing big little problem-postoperative nausea and vomiting: A systematic review. Journal of Education and Health Promotion, 13(1), 298–298. https://doi.org/10.4103/jehp.jehp_1666_23





















