Introduction
Lacerations are a common cause for patient presentation to the emergency department in the United States, with over 2.5 million patient encounters (Peluso et al., 2024). The experienced emergency or urgent care provider is well-versed in controlling exsanguinating bleeding and acute wound repair. This typically involves pressure, elevation, possible tourniquet usage, and quick repair of the wound edges or bleeding vessel to help the wound self-tamponade. STOP THE BLEED® has taught civilian bystanders and providers to apply pressure, elevate, and apply a tourniquet (ACS, n.d.), which is the gold standard for any patient seen with an active external hemorrhage, prehospital or acute care setting.
Facial laceration repair in the urgent or emergent setting requires attention to both functional and cosmetic outcomes due to the face’s delicate structures and aesthetic importance. Unlike other body areas, the face and neck are paramount for the best cosmetic outcome. Facial scarring can significantly impact the patient’s social interactions and self-esteem, as the face and neck are highly visible parts of the body and play a central role in self-identity and interpersonal interactions. Poor cosmetic outcomes may lead to long-term psychological effects, including embarrassment, social withdrawal, or even anxiety and depression, especially in cases where the scars are large, raised, or otherwise disfiguring.
The skin on the face and neck is thinner and more vascular than other parts of the body (Marks et al., 2017), allowing it to heal quickly and making it more susceptible to prominent scarring if not handled delicately. The area is more exposed to UV rays, which can cause scar pigmentation or worsening if not properly managed during healing. Due to this significant impact, a discussion with the patient about the post-repair and healing process, specifically with sun coverage and sunscreen for up to one year after injury, is key to lessening the chances of hyperpigmentation and disfigurement.
Mastering a few essential suturing techniques for rural urgent and emergent providers can be invaluable, especially when access to advanced care or referral options is limited. This will limit the lasting impact of a poor cosmetic outcome on the face and neck. Several resources are available to hone suture techniques, suture choice, wound edge approximation, suture removal times, and follow-up instructions. These resources can be daunting to navigate for the novice provider and nearly impossible to manage as a busy practitioner. This breakdown of the essentials of face and neck laceration repair can help any level of provider with a quick reference while in the moment of repair.
Putting Ideas into Practice
Before wound repair can take place, it is imperative to clean the wound thoroughly. This will give the clinician the cleanest picture to visualize optimal wound closure. Assess for debris in the wound, devitalized tissue, or foreign bodies, and rinse with copious amounts of clean water (Otterness & J Singer, 2019). Consider radiological studies like X-rays or CT to evaluate for retained foreign bodies or underlying fractures that may complicate repair and follow-up plans, as facial lacerations are commonly caused by blunt or penetrating trauma (Allareddy et al., 2011).
Evaluate the Wound
There are several considerations when approaching the evaluation of the wound. The provider must consider the size, shape, and location of the wound on the face and neck. The concept of facial subunits is crucial in cosmetic repair and wound closures of the face and neck (Marks et al., 2017). These subunits are face areas with unique contours, skin textures, colors, and structures. Aligning wounds with natural borders or folds can camouflage scars effectively by blending scars into the natural facial architecture, resulting in less noticeable healing (Fattahi, 2003). (See Figure. 1)
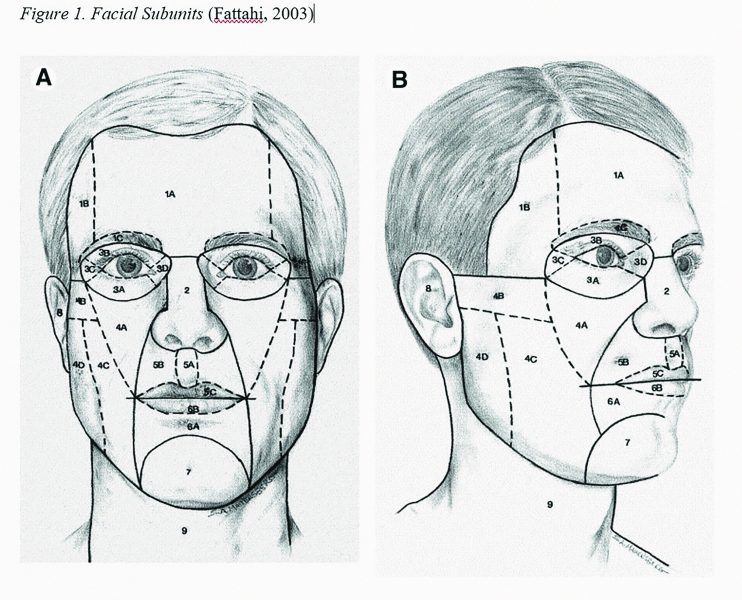
Special consideration should also be given to the skin of the neck. While it is fairly mobile and easy to appropriate the skin edges, one must consider the mobility and natural creases. Repairs to the skin on the neck need to consider the tension inherent in neck movement, as tension can lead to wider scars with a higher incidence of keloid production (Marks et al., 2017).
A secondary part of evaluating the wound is considering the addition of deep suture material versus superficial epidermis closure alone. Deep sutures are crucial for optimal cosmetic outcomes in wound management, particularly for deeper or gaping wounds. Utilization of deep suturing, with dissolvable sutures, provides structural support and reduces tension on the superficial skin layers, allowing the tissue edges to evert or turn outward, which minimizes scarring. Deep suturing also helps reduce the dead space within the wound to prevent hematomas or seromas. This eliminates pockets where fluid could accumulate, which may delay healing or increase the risk of infection.
Suture Material Choice
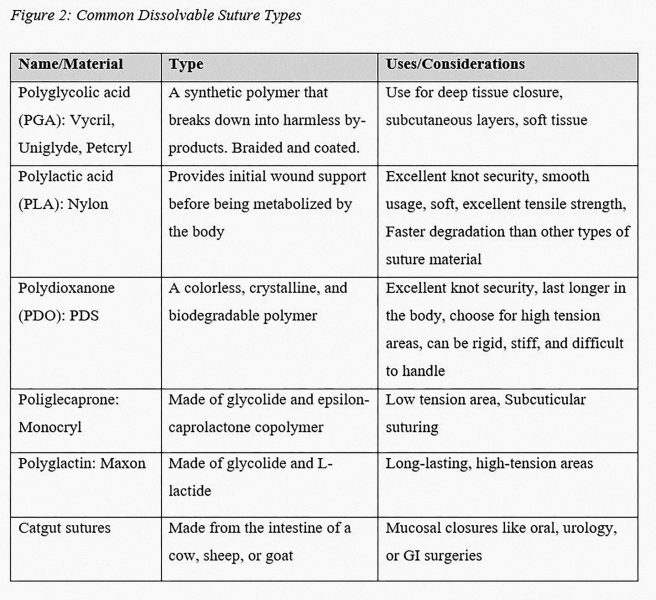
There are several types of suture material to choose from. The type of suture selected is based on the location of the wound along the facial subunits and the amount of tension on the wound edges. When choosing a deep suture material, the only option is a dissolvable or absorbable suture material. Dissolvable sutures are ideal for healing internal wounds and surgical sites because they do not need to be manually removed, reduce the risk of tissue trauma, and promote tissue regeneration. (See Figure. 2)
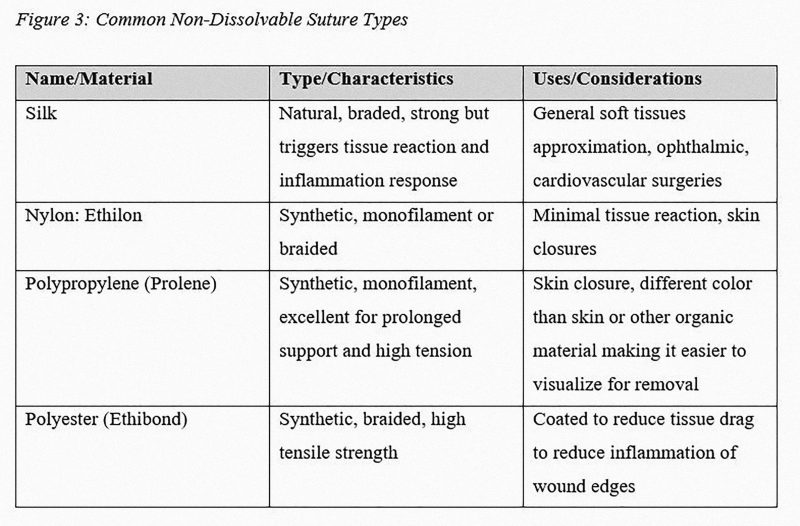
There are also several types of suture material to choose from for primary overlying skin tissue closure. Non-dissolvable sutures, such as nylon or polypropylene, offer better control and precision for fine, tension-free wound closure (Basyuni et al., 2024). This is crucial for aligning delicate facial tissues accurately, especially in high-visibility areas like the face and neck. Non-dissolvable sutures also allow for careful removal once healing has progressed sufficiently, reducing the likelihood of scarring (Basyuni et al., 2024). For patients who may be lost to follow-up, the choice may be made to avoid a non-dissolvable suture material. In this case, a dissolvable suture may be chosen due to the patient’s likelihood of not returning for suture removal. Suture size is also a consideration when dealing with facial and neck repair. The larger the number on the package, the smaller the suture and needle size. Generally, smaller suture material is chosen for facial and neck laceration repair due to the lessened effect of long-term scarring.
(See Figure. 3).
References
Allareddy, V., Allareddy, V., & Nalliah, R. P. (2011). Epidemiology of facial fracture injuries. Journal of Oral and Maxillofacial Surgery, 69(10), 2613–2618. https://doi.org/10.1016/j.joms.2011.02.057
American College of Surgeons (ACS). (n.d.) Stop the bleed [homepage]. Retrieved November 20, 2024, from https://www.stopthebleed.org/
Basyuni, S., Ferro, A., Jenkyn, I., Nugent, G., Bennani, M., Bennett, H., Chu, J., Davies, M., Hjalmarsson, C., Moorhouse, K., Bosley, R., Mehdizadeh, R., Pancharatnam, N., Cameron, M., Man, C.-B., Moar, K., Thompson, M., Fowell, C., & Santhanam, V. (2024). Randomised controlled trial of resorbable versus non-resorbable sutures for lacerations of the face (TORN Face). British Journal of Oral and Maxillofacial Surgery, 62(7), 642–650. https://doi.org/10.1016/j.bjoms.2024.05.012
Fattahi, T. T. (2003). An overview of facial aesthetic units. Journal of Oral and Maxillofacial Surgery, 61(10), 1207–1211. https://doi.org/10.1016/S0278-2391(03)00684-0
Marks, M., Polecritti, D., Bergman, R., & Koch, C. A. (2017). Emergent soft tissue repair in facial trauma. Facial Plastic Surgery Clinics of North America, 25(4), 593–604. https://doi.org/10.1016/j.fsc.2017.06.010