

The rural environment significantly contributes to maternal morbidity and mortality, especially in hospital systems delivering fewer than 460 newborns annually (Berstein et al., 2023). San Luis Valley Health (SLVH), the only hospital in the San Luis Valley, Colorado, that provides maternal delivery services, faces a unique challenge due to its annual delivery rate of approximately 400 newborns. This article discusses the increasing rates of severe maternal morbidity (SMM) in pregnant women, the preventable nature of maternal deaths due to obstetric hemorrhage (ACOG, 2019), and the integration of the novel JADA® System into treatment protocols to mitigate these risks (Shields et al., 2024).
Introduction
San Luis Valley Health (SLVH) serves about 46,000 residents, with nearly half of the patient population being Hispanic. (SLVIRC, 2024). This demographic experiences higher maternal mortality and postpartum hemorrhage (PPH) rates compared to white populations (AHRQ, 2022). The Hispanic population faces a 13% higher rate of PPH, than white populations (Feng et al., 2017).
Uterine atony accounts for 80% of PPH cases, representing a significant threat to maternal health, and is a leading cause of SMM (Corbetta-Rastelli et al., 2023). In the United States, pregnant women face increasing maternal and morbidity rates, which has the highest rates compared to other high-income countries (AHRQ, 2022). Deaths in the United States due to obstetric hemorrhage are preventable (ACOG, 2019). Current treatment protocols at SLVH include various interventions such as fundal massage, bimanual examinations, the use of uterotonics, and, in severe cases, surgical options. The Women’s Unit follows a nationally approved, evidence-based treatment bundle supported by the American College of Obstetricians and Gynecologists, the Association of Women’s Health, Obstetric and Neonatal Nurses, and the California Maternal Quality Care Collaborative (CMQCC).
Shared Governance
Shared governance models are decision-making processes that involve collaboration, shared accountability, and a shared vision, culminating in a partnership that not only supports organizational strategic plans but also enhances professional development (Brennan and Wendt, 2021). Additionally, they improve multidisciplinary collaboration, leading to greater workplace engagement, and allowing clinical nurses to drive change. Shared governance models are vital because they significantly enhance the quality of care and patient outcomes (Brennan and Wendt, 2021).
The Professional Nursing Practice Council at SLVH operates as a shared governance model, researching up-to-date evidence-based practice standards and providing recommendations to nursing leadership on implementing best practices to improve the quality of patient care. This council seeks to evaluate innovative methodologies, including the JADA® System, to optimize patient care and mitigate the adverse outcomes and comorbidities associated with PPH rates in the Women’s Unit.
Purpose
This quality improvement project aims to compare the effectiveness of the JADA® System against the Bakri Balloon in reducing blood loss and associated costs during PPH treatment. The purpose encompasses ongoing evaluation of PPH management strategies to enhance early identification and intervention. The council set out to answer the clinical question: In postpartum women, how does using the JADA® device, compared to the Bakri Ballon, reduce blood loss associated with PPH in the first 24 hours after birth?
Methodology
A retrospective study of 675 patients with PPH occurring within 24 hours of delivery at SLVH (January 2022 to August 10, 2023) was conducted. Utilizing the Johns Hopkins Nursing Evidence-Based Practice Model, the study aimed to critically evaluate and apply the latest research and practice standards regarding PPH treatment. Several high-quality research articles and literature on the FDA-approved JADA® System were utilized to support this initiative. This analysis is critical to understanding the real-world impact of integrating the JADA® System into clinical practice and to ensure that the adopted practices are based on the most current evidence.
Results
During the study period, SLVH recorded 675 deliveries, comprising 529 vaginal births and 146 cesarean sections. A total of 38 PPH cases were documented, with 18 patients requiring blood transfusions and one patient necessitating a hysterectomy. The observed PPH rate of 5.7% exceeds the national average of 4.3% (Corbetta-Rastelli et al., 2023), while the blood transfusion rate was exceptionally high at 47%, compared to the average of 12.6% (Corbetta-Rastelli et al., 2023) from 2011 to 2019. Furthermore, the hysterectomy rate of 2.6% starkly contrasts with the national average of 0.9% (Corbetta-Rastelli et al., 2023). Analysis of hemorrhagic shock criteria revealed that 24% of patients met class I criteria, 57.6% met class II criteria, 5.26% met class III criteria, and 9.09% met class IV criteria.
Cost Analysis
The average costs associated with vaginal and cesarean deliveries at SLVH are approximately $9,000 and $14,000, respectively (CIVHC, n.d.). The total charges for labor, delivery, and postpartum care, including PPH treatment, ranged from $12,000 to $34,808. Specifically, costs for PPH treatment ranged from $3,000 to $25,808. In a cost analysis comparing a theoretical cohort of 75,000 women with the Bakri or the JADA® system, the JADA® system reduced the amount of charges extensively for a total of $144,773,439 (Bridges et al., 2023).
Ongoing Patient Analysis
Ongoing analysis of this project evaluates the management of PPH with and without the JADA® System to determine its effectiveness, thereby aiming to increase implementation through early identification. From August to December, the remainder of 2023, there were an additional 148 deliveries, and the PPH rate decreased to 5.4%. There was a significant improvement in the transfusion rate, which decreased to 13%. The peripartum hysterectomy rate also decreased to 1%. It is important to note that the patients who met PPH criteria did not exceed 1,500 mL of blood loss, and no patients in this time frame met class III or IV hemorrhagic shock criteria. In 2024, there were 389 deliveries with a 4.6% PPH rate, 22% blood transfusion rate, and a 0% peripartum hysterectomy rate. Ten patients met class II hemorrhagic shock criteria, five met class III, and one met class IV. From January to June this year, there were 207 deliveries. For those deliveries, the PPH rate was 5.3%, the blood transfusion rate was 9%, and the peripartum hysterectomy rate was 0%. Seven patients met class II hemorrhagic shock criteria, and one patient met class III criteria.
Discussion
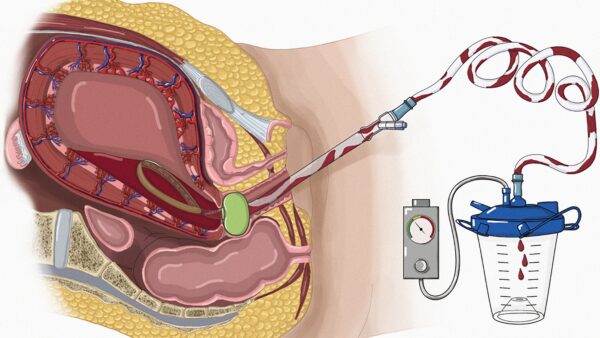
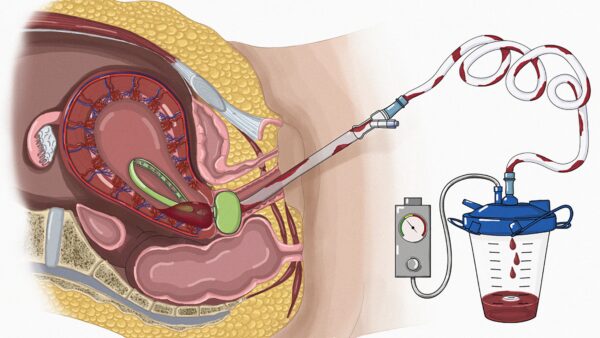
The JADA ® System is a vacuum-induced hemorrhage-control device that is placed in the uterus, providing low-level suction, inducing uterine contractions to control and treat abnormal uterine bleeding caused by atony (D’Alton et al., 2020). The alarming rates of PPH and associated complications stress the necessity for implementing effective treatment protocols. By integrating the JADA® System into existing practices at SLVH, there is potential to improve maternal outcomes significantly.
With dedicated patient surveillance, providers and nursing staff improved patient care delivery. As previously highlighted, the rates of PPH, blood transfusions, and peripartum hysterectomies have decreased significantly, thereby enhancing the overall quality of care provided to patients.
Based on the evidence provided to the Perinatal Committee and Nursing Leadership, the Women’s Unit has successfully implemented the JADA® System. Since its inception, it has been used four times, each time improving the outcomes for those patients. In these cases, bleeding was controlled within minutes with only an additional blood loss of less than approximate average of 250 mL.
Dr. Carmelo Hernandez, MD, MHA, FACOG, an Obstetrician and the Chief Medical Officer at SLVH, states, “The implementation of the JADA® System at SLV Health has the real potential to reduce comorbidities and eliminate the need for hysterectomy as a solution to PPH”. By continuously monitoring patient outcomes, the Women’s Unit at SLVH can adapt practices as needed and better address the specific healthcare challenges faced by the local population.
Conclusion
This quality improvement initiative highlights the urgent need for enhanced postpartum hemorrhage management in rural settings. Employing the JADA® System could mitigate severe maternal morbidity and potentially reduce healthcare costs associated with PPH treatment.
References
1. ACOG. (2019). Committee report: Quantitative blood loss in obstetric hemorrhage. Number 794. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2019/12/quantitative-blood-loss-in-obstetric-hemorrhage
2. AHRQ. (2022). National healthcare quality and disparities report [Internet]. Maternal Health. Rockville, MD. https://www.ncbi.nlm.nih.gov/books/NBK587184/
3. Berstein, S., Picciolo, M., Grills, E., and Catchpole, K. (2024). A qualitative study of systems-level factors that affect rural obstetrics nurses’ work during clinical emergencies. The Joint Commission Journal on Quality and Safety. 50(7): 507-515. https://doi.org/10.1016/j.jcjq.2023.12.002
4. Bridges, A., Doshi, U., and Caughey, A. (2023). Bakri balloon vs. JADA device for treatment of postpartum hemorrhage: A cost-effective analysis. American Journal of Obstetrics and Gynecology. 228(1). S600. https://www.clinicalkey.com/#!/content/journal/1-s2.0-S0002937822019020
5. Center for Improving Value in Healthcare (CIVHC). (n.d.). Data drive: Cost of labor and delivery in Colorado. https://civhc.org/2022/09/05/data-dive-cost-of-labor-and-delivery-in-colorado/#:~:text=Published%20by%20CIVHC%20on%20September%205%2C%202022%20September%205%2C%202022&text=Colorado’s%20statewide%20vaginal%20delivery%20costs,the%20national%20average%20of%20%2414%2C768
6. Corbetta-Rastelli, C., Friedman, A., Sobhani, N., Arditi, B., Goffman, D., and Wen, T. (2023). Postpartum hemorrhage trends and outcomes in the United States, 2000–2019. Obstetrics & Gynecology, 141(1), 152-161. DOI: https://doi.org/10.1097/AOG.0000000000004972
7. D’Alton, M., Rood, K., Smid, M., Simhan, H., MS; Skupski, D., Subramaniam, A., Gibson, K., Rosen, T., Clark, S., Dudley, D., Iqbal, S., Paglia, Michael, J., Duzyj, C., Chien, E., Gibbins, K., Wine, K., Bentum, N., Kominiarek, M., Tuuli, M., Goffman, D. (2020). Intrauterine vacuum-induced hemorrhage-control device for rapid treatment of postpartum hemorrhage. Obstetrics & Gynecology, 136(5), 882-891. DOI: https://doi.org/10.1097/AOG.0000000000004138
8. Feng, C., Paasche-Orlow, M. K., Kressin, N. R., Rosen, J. E., López, L., Kim, E. J., Lin, M. Y., & Hanchate, A. D. (2018). Disparities in potentially preventable hospitalizations: Near-national estimates for Hispanics. Health Services Research, 53(3), 1349–1372. https://doi.org/10.1111/1475-6773.12694
9. Organon Group of Companies. (2025). The JADA® system media kit. https://organonpro.com/en-us/product/the-jada-system/media-kit-content/
10. Shields, L., Klein, C., Torti, J., Foster, M., and Cook, C. (2024). Effectiveness of the intrauterine balloon tamponade compared with an intrauterine, vacuum-induced, hemorrhage-control device for postpartum hemorrhage. Obstetrics & Gynecology. DOI: https://doi.org/10.1097/AOG.0000000000005770
11. SLVDRG. (2023). San Luis Valley statistical profile. https://www.slvdrg.org/wp-content/uploads/2023/04/2023-San-Luis-Valley-Statistical-Profile-.pdf
12. SLVIRC. (2024). About us: Working together to build a strong community. https://slvirc.org/about/#:~:text=SLVIRC%20serves%20a%20geographically%20remote,Legal%20Access%20Programs%20(OLAP).
















