

This is sponsored content and is supplied by Nurses Service Organization. The content has been reviewed by our HCM internal editorial staff but is not peer-reviewed.
NURSE LEGAL CASE STUDY: ABSENCE OF DOCUMENTATION IN VIOLATION OF NURSING STANDARD OF CARE
The patient was admitted to a rehabilitation facility after undergoing a right hip arthroplasty. Due to the patient’s other co-morbidities, her rehabilitation and recovery was slow and difficult. The patient’s health continued to deteriorate during her admission, until her death four months following admission.
After the death of the patient, the family (plaintiffs) filed a complaint with the Department of Health (DOH) regarding the patient’s care at the facility. The DOH investigated the complaint and cited 13 violations in the nursing standard of care. In particular, the DOH was critical of the absence of documentation related to care plans for the Foley catheter, the patient’s weight loss (from 93 to 77 pounds over four months), and neither shower nor self-care was documented for a timespan of more than five weeks. The insured registered nurse (RN) was the facility’s wound care nurse, and the DOH’s investigation found several violations of the nursing standard of care specific to the RN’s lack of documentation. First, the DOH found a lack of documentation regarding a nursing incision wound for a period of approximately three weeks. The RN told the DOH surveyor that daily assessments were performed during that time, but, since the wound care orders were to leave the right hip incision wound open to air, no treatment was performed, so the RN did not document anything. The patient also had a left heel pressure injury that was not healing, and the RN agreed that this non-healing injury had not been appropriately assessed or documented. Moreover, the director of nursing informed the DOH surveyor that the RN was required to perform weekly assessments on all patients in the facility. However, none were noted in the patient’s healthcare information records during a three-month period.
After seeing the DOH report, the family sued the facility and sued the insured RN separately. Knowing the challenges of the missing documentation and the negative DOH report, mediation was proposed with the plaintiffs. The total incurred amount to defend and settle this case on behalf of the insured RN was greater than $270,000.
Nurses Service Organization (NSO), in collaboration with CNA, has published our 4th Edition of the NSO/CNA Nurse Liability Claim Report. It includes statistical data and case scenarios from CNA claim files, as well as risk management recommendations designed to help nurses reduce their malpractice exposures and improve patient safety.
You may access the complete report, and additional Risk Control Spotlights, at: www.nso.com/nurseclaimreport.
This Nurse Spotlight focuses the analysis and risk recommendations regarding one of the most significant topics in the report and for nursing professionals: Healthcare Documentation.
Nursing Allegations Related to Healthcare Documentation
While documenting care represents a critical component of nursing processes and standards, the electronic health record [EHR] has posed a level of complexity for nurses who are often challenged with why, how, what and where to document in a patient’s EHR.
Documentation deficiencies are contributing factors to many nurse professional liability claims, as well as license protection matters. However, in the 4th Edition of the NSO/CNA Nurse Liability Claim Report, failure to document or falsifying documentation closed claims,as an allegation of professional liability, increased in distribution and severity when compared to the 2011 closed claim report and the 2015 closed claim report. At left is an example of a professional liability claim asserted against a nurse due to the failure to document:
In the 2011 closed claim report, 0.2 percent ($31,250) of all closed claims were related to inadequate or inappropriate documentation as the primary allegation. This data increased slightly to 0.5 percent ($139,920) in the 2015 closed claim report. Respectively, in the 2020 closed claim report, documentation allegations represent 2.0 percent ($238,761) of all closed claims.
(Figure 1) demonstrates the increase in severity of professionalliability claims related to documentation allegations. While these professional liability claims occur infrequently in the 2011, 2015 and 2020 closed claim analyses, allegations related to documentation failures can be difficult to defend and often result in a license protection defense matter against the nurse.
2020 Claim Reports
Average Total Incurred of Closed Professional
Liability Claims by Documentation Allegations

License Protection Allegations Related to Documentation
Errors and Omissions
A license protection matter and a professional liability claim reflect a number of differences. First, a license protection matter only involves the cost of providing legal representation to defend the nurse before a regulatory agency or State Board of Nursing (SBON). On the other hand, professional liability claims include an indemnity or settlement payment. Second, license protection matters asserted against a nurse’s license to practice may or may not involve allegations related to patient treatment and care. The Nurse Spotlight: Defending Your License provides an overview of the roleof the State Board of Nursing in the legal/regulatory system, describes the disciplinary process, and imparts helpful recommendations on defending yourself if you were to receive a Nurse Spotlight: Defending Your License complaint summons.
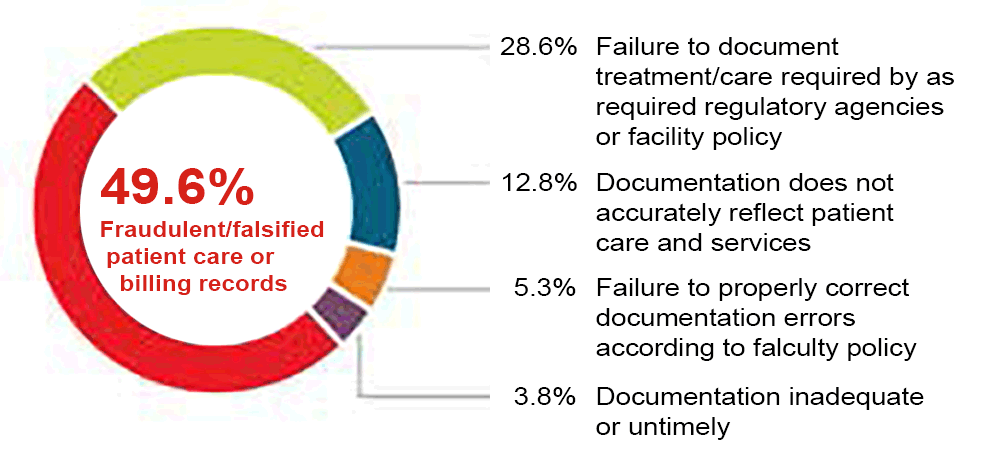
(Figure 2) displays license protection matters with defense expensepayments that involve allegations related to documentation. Documentation as a primary allegation comprises 9.7 percent of all license protection matters in the Nurse Liability Claim Report: 4th Edition. Approximately half of the license protection matters related to documentation involve an allegation of fraudulent or falsified patient care or billing records (4.8 percent).
Related to Documentation Errors and Omissions
A nurse’s license is one’s livelihood, and its protection is paramount. A nurse’s practice and behavior is expected to be safe, competent, ethical and in compliance with applicable laws and rules. However, when a complaint is filed, nurses must be equipped with the resources to adequately defend themselves. Being unprepared may represent the difference between a nurse retaining or losing the license to practice, a suspension or fine.
The False Claims Act
While documentation deficiencies may result in a professional liability claim and/or a license protections matter, nurses also may be subject to federal and state sanctions for knowingly falsifying healthcare documentation under the federal False Claims Act (FCA). The FCA imposes liability on any person who submits a claim to the federal government that they know (or should have known) is false. An example may be a healthcare provider who submits a bill to Medicare for medical services they know they have not provided. The False Claims Act also imposes liability on an individual who may knowingly submit a false record in order to obtain payment from the government. For additional information on fraud and abuse laws, please see the Office of Inspector General’s provider education materials on Fraud & Abuse Laws.
Healthcare Documentation: Minimizing Risks, Maximizing Benefits
NSO/CNA is often asked about documentation risks and recommendations to minimize those risks. Nurses are certainly aware that there are patient healthcare documenting fundamentals. The healthcare information record is a legal document that is an essential tool to:
- Document the services provided regarding the patient’s illnessor injury, response to treatment, and caregiver decisions;
- Communicate documented information about the patient’splan of care and outcomes to the health care team
- Communicate information to other nursing professionals and healthcare providers;
- Support the appropriate information for billing coding; and
- Serve as the organization’s business and legal record.
Because complete, accurate and legible healthcare records constitute an essential risk management measure, nurses should maintain proper documentation practices and follow facility policies and procedures governing appropriate and comprehensive records documentation. The facility’s healthcare record documentation policies and procedures should address, at a minimum:
- Correcting documentation errors;
- Delineating appropriate use of the copy and paste function inthe electronic healthcare record;
- Documenting practices during electronic system failures oroutages (“down-time”);
- Maintaining patient confidentiality;
- Releasing patient healthcare information records and auditing practices; and
- Procedures for late or delayed entries.
Risk Management Recommendations: Documentation
Maintaining a consistent, professional patient healthcare information record is integral to providing quality patient care, ensuring consistent communication among all professionals caring for the patient, documenting patient care outcomes and response and establishing the basis for an effective defense in the event of litigation. The following guidelines can help reduce risk:
Documentation – Clinical Content
- Document nursing actions in accordance with facility requirements and patient needs, capturing the following information as clinically indicated:
- results of each nursing assessment
- pertinent nursing observations
- patient complaints or concerns
- significant changes in the patient’s condition
- any change in the patient’s care plan
- relevant monitoring findings, treatment or episode of care, as well as the patient’s response to that care
- facts relating to any patient accident or incident, including evidence of any injury, all parties notified, nursing care provided and patient’s condition after care is rendered
- laboratory and diagnostic test results, especially those that are abnormal and require provider notification and/or intervention
- referral and consultation requests and results
- telephone, face-to-face and electronic contacts with other members of the healthcare team, including the content of discussions and agreed-upon follow-up.
- Document discussions with the patient about medical issues that require additional explanation by any healthcare practitioners and provider(s).
- Record medications administered, including injections, ointments and infusions, as well as a description of the patient’s response as necessary. Also record self-administered medications.
- Detail nursing observations during patient contacts.
- Specify patient’s questions and answers given regarding the nursing care/service plan, as well as the goals and methods of treatment.
- Describe the patient’s response to nursing care.
- Note the review of current problems and plan of care.
- Assess skin and wound condition, including clinical findings and observations, and interventions, the nursing care/service plan and the patient’s response to treatment.
- Document practitioner notification of a change in condition, symptoms, or patient concerns and document the practitioner’s response and/or orders, as well as any changes in the treatment plan
- Summarize communications with practitioners, including those via telephone, facsimile and e-mail, text messages and patient portal communication and note any subsequent orders and nursing interventions.
- Note use of an interpreter, including the interpreter’s contact information, as well as the patient or family member’s willingness to communicate with an interpreter.
Documentation – Medications and Prescriptions
- Review and update the current medication list and patient’s reported adherence to prescribing orders. The list should include both prescribed and over-the-counter medications, including supplements and holistic/alternative remedies.
- Collect and document the appropriate medication history as an essential component of the medication reconciliation process following patient admission, changes in care or treatment, transfer from one service to another (e.g., after surgery or delivery), or post-discharge return to care.
- Clearly describe patient responses to medications, expected and unexpected.
- Document signs or symptoms of adverse drug reactions, contact with physicians/licensed independent practitioners and subsequent follow-up. Based on facility policies and procedures, contact with the patient’s pharmacy as well as the facility’s pharmacy may be warranted.
- In the case of any rare verbal orders, document that the order was read back and verified.
For additional information regarding medications and prescriptions, refer to the Nurse Spotlight: Medication Administration.
Nursing Scope and Standards of Practice
According to the American Nurses Association (ANA), documentation represents a critical competency of all nursing processes and standards of practice (ANA Nursing Scope and Standards of Practice 3rd Edition, 2015).
The ANA Standards of Practice Competencies include the following criteria for appropriate documentation:
- Documents relevant patient data accurately and in a manner accessible to the inter-professional team (ANA Standards of Practice, Standard 1. Assessment).
- Documents the patient’s nursing and medical diagnosis, problems and issues in a manner that facilitates the determination of the expected outcomes and plan (ANA Standards of Practice, Standard 2. Diagnosis).
- Documents expected patient outcomes as measurable goals (ANA Standards of Practice, Standard 3. Outcomes Identification).
- Documents the patient’s plan of care with the prescribed strategies used to attain expected measurable outcomes using standardized language or recognized terminology (ANA Standards of Practice, Standard 4. Planning).
- Documents implementation and any modifications, including changes or omissions, of the identified plan (ANA Standards of Practice, Standard 5. Implementation).
- Documents the coordination of care (ANA Standards of Practice, Standard 5A. Coordination of Care).
- Documents the results of the evaluation (ANA Standards of Practice, Standard 6. Evaluation).
- Documents nursing practice in a manner that supports quality and performance improvement initiatives (ANA Standards of Practice, Standard 14. Quality of Practice).
Documentation – Diagnostic Tests, Referrals, Consultations
- Contact the patient’s healthcare provider to report abnormal test results and any provider orders for additional testing or follow-up and document the interaction.
- In cases of a non-response/delay or urgent/emergent consultation, contact the consulting physician(s) or practitioner(s) to confirm that the consulting provider was notified of the consultation request and to facilitate the timely provision of the consultation and receipt of the results, as needed. Document these actions in the patient’s healthcare information record.
- Utilize the chain of command to report abnormal laboratory results and the results of consultations if the ordering/primary care provider (physician, APRN, PA) is not available or does not respond to messages.
- Initiate additional steps, if necessary, to ensure timely patient care. These may include escalating to the supervisor/nurse manager, administrators, attending or covering physician, licensed independent practitioner and/or medical staff leadership until the abnormal result is addressed.
Documentation – Patient Education
- Describe patient and family healthcare education encounters, listing the presence of specific family members and their relationship to the patient.
- Document an assessment of the patient’s ability to comprehend and repeat information provided using a “teach-back” approach, both immediately and after a few minutes have elapsed to test accurate recall.
- Provide a written assessment of the patient’s appropriate demonstration of procedures/taught tasks, such as blood glucose testing or application of dressings.
- Maintain a copy of written materials provided and document references to standard educational tools.
- Retain patient-signed receipts for any educational materials provided. If a family member or friend receives the education materials due to the patient’s cognitive abilities, reflect a note in the healthcare information record to that effect. The family member’s or friend’s name should be documented as the person that received the materials.
- Document the use of interpreters, if needed, and include the interpreter’s contact information.
Nurse Spotlight
For risk control strategies related to:
- Defending Your License
- Medication Administration
- Liability for Nurse Managers
- Depositions
- Communication
- Home Care
Visit nso.com/nurseclaimreport





















