Creating safe environments for children with mental health crises is an absolute for safe care, for both patients and staff within the healthcare industry. Additionally, the emergency room is the introductory point where mental health crises patients are often sent, yet staff in these departments have limited, or no training to navigate this complexity. Recent research indicates that mental health-related ER visits for pediatric patients have increased over 60% in the last decade, further highlighting the urgent need for crisis management strategies (Georgadarellis & Baum, 2023). Verbal de-escalation techniques are essential to manage populations, prevent added trauma and injury, and improve staff competency and comfortability by implementing these in an emergency. Despite existing barriers such as inconsistent protocols and resource shortages, integrating de-escalation education into hospital policy and crisis management frameworks is essential for sustained improvement, and to inform best practices for handling acutely agitated pediatric patients and contribute to the development of standardized, evidence-based protocols within emergency care settings.
Background
Behavioral health crises in pediatric emergency departments (ED’s) are increasingly challenging and with 500,000 pediatric patients presenting to ED’s each year for vpsychiatric care (Hudgins & Lee, 2025), the need for confident and competent staff to provide care has never been greater. Frontline observations, incident reports, and a review of current literature indicate that inconsistent approaches to verbal de-escalation in pediatric ED settings contribute to increased aggression, staff injuries, and reduced therapeutic rapport. This led to the development of the PICOt question: Among emergency room staff who encounter behavioral health patients exhibiting violent behaviors, how effective is verbal de-escalation training in improving competency and confidence, compared to pre-training, over a three-month period?
The project’s aim was to implement a standardized verbal de‑escalation education for emergency room staff, using the “Ten Domains of Verbal De-escalation” (heretofore referred to as “The Ten Domains”) from Techniques for the Agitated Pediatric Patient (Georgadarellis & Baum, 2023). Evaluation was then made regarding impact on staff competency, confidence, and comfort in managing pediatric behavioral health crises.
Methods
Due to applicability in emergency settings, scalability, and rapid-cycle evaluation, the PDSA quality improvement model was selected. In a local Oklahoma pediatric ED, a gap analysis revealed that although staff were routinely exposed to behavioral health crises, standardized, evidence-based verbal de-escalation training did not exist. Practices varied widely between providers, and staff reported limited confidence or comfort in managing escalating behaviors. Staff responses were reactive and did not reflect trauma informed, evidence-based communication techniques, therefore this quality improvement project centered on delivering accessible, multimodal education to all emergency room staff.
The project was introduced to the agency through leadership communication, emphasizing the need for consistent, trauma‑informed de‑escalation practices. Staff were invited to attend an in‑person training session covering The Ten Domains. Training was provided via in-person education, emailed PowerPoint for those unable to attend, and unit-based flyers to reinforce key strategies and maintain visibility of the initiative. Outcomes were measured using pre‑training, post‑training, and one‑ and three‑month follow‑up assessments delivered through Microsoft Forms. The data was collected, managed in Excel, and statistically analyzed using SPSS software.
Finally, findings were used to reinforce training, and guide future iterations of the program. Training materials were designed to be practical, scenario‑based, and directly applicable to pediatric behavioral health emergency encounters. The project rollout included clear expectations for participation and timelines for completing assessments.
Results and Analysis
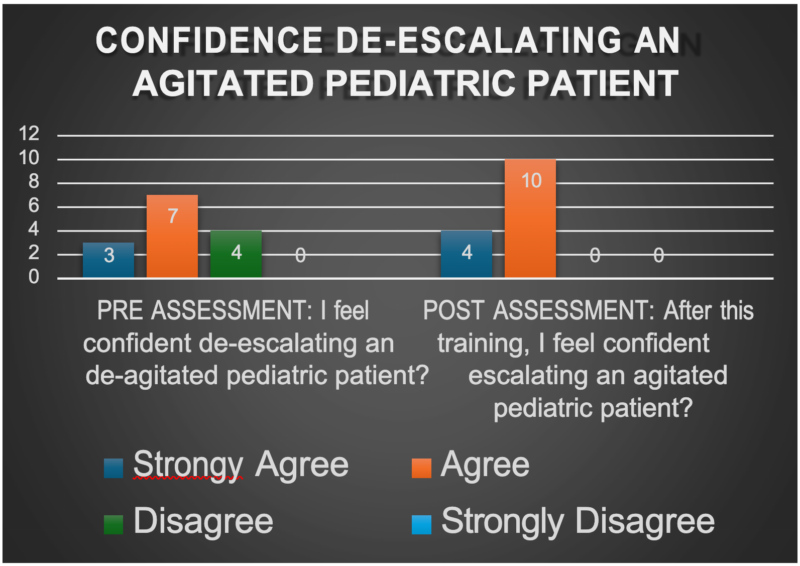
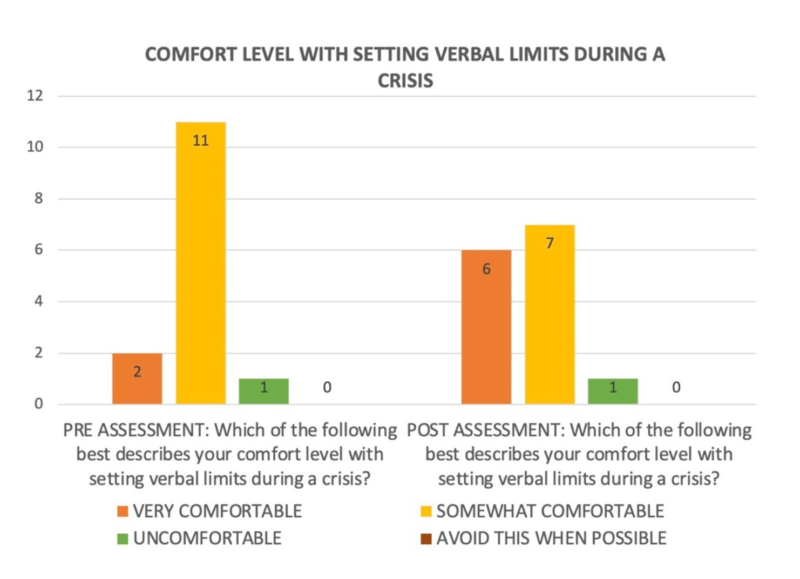
A Wilcoxon signed‑rank test was used to compare pre‑ and post‑training scores given the non‑parametric data and small sample size. Results from the immediate post assessment showed a statistically significant increase in staff (a combination of nurses, behavioral health technician, physician, and pharmacy staff) confidence when de‑escalating an agitated pediatric patient (n=14, Z = –2.33, p = .020), as outlined on Table 1, and a statistically significant improvement in comfort with setting verbal limits during a crisis (n=14, Z = –2.00, p = .046) per Table 2, demonstrating meaningful gains in staff self‑reported skills and comfort levels following the training. While assessing early signs of agitation, 93% reported being able to before the instruction was received, 100% reported being able recognize early agitation after receiving the education.
To evaluate competency, we included four identical content-based- questions on the pre-and post- assessments to measure knowledge retention. A McNemar test in SPSS showed no significant change in responses, because most participants answered these questions correctly on the pre-assessment. This finding suggests there was minimal room for improvement and indicates that staff entered the training with a baseline understanding of key verbal de‑escalation concepts.
During the in-service, staff also had the opportunity to share personal experiences.
Several recounted challenging encounters with agitated patients, and one even expressed wishing they had received this training before being injured in a prior incident.
For those who had the PowerPoint emailed to them due to the lack of attendance, no responses were received via this avenue. Additionally, only one response for the one month follow up, and two responses from the three month follow up were received. Statistical analysis could not be run or measured for long term retention, due to the lack of responses.
Discussion
All seventy-seven counties in Oklahoma are designated as mental health professional shortage areas. This shortage funnels a disproportionate number of pediatric patients experiencing a mental health crisis to available ED’s throughout the state (Healthy Minds Policy Initiative, 2023). This critical healthcare gap has placed Oklahoma ED staff at the frontlines of managing mental health patients. For these nurses, our results are relevant and pertinent to their daily workflow. Improved confidence, comfortability, and competency managing agitated patients while applying The Ten domains, embodies a therapeutic, evidence-based approach that promotes safety for both patients and the staff caring for them.
The project led to several meaningful practice shifts. Staff expressed interest in incorporating The Ten Domains into the facility’s upcoming onboarding curriculum. Of note, educational flyers and digital reference materials continue to be used on the unit to reinforce key strategies. These outcomes suggest that structured, trauma‑informed training offers sustained value for staff skill development.
This quality improvement project is highly generalizable across various healthcare settings and populations. Moreover, this education does not require additional cost to the facility, allowing integration into employee onboarding, yearly education requirements, and bolstering daily staff workflows.
A few noteworthy limitations were encountered. Biases may exist. These include self-reporting and observational limitations, and heterogeneity in design and outcomes, which may undermine comparability. Resource limitations, such as insufficient staff or infrastructure in smaller hospitals, and the resource-intensive nature of studies further constrain implementation across diverse settings. Finally, external factors, including regional variations and the absence of standardized reporting or institutional oversight, may exacerbate gaps.
Conclusions
This evidence-based multimodal training approach accommodates diverse staff schedules, provided reinforcement through visual reminders, structured follow‑up assessments, and goal clarity. Project enhancements may involve incorporating simulation‑based practice to deepen skill retention, expanding participation to include security staff or ancillary personnel, increasing the sample size to improve statistical power, and embedding the training into mandatory competencies from the outset to ensure consistent, universal engagement. n
Keywords: “de-escalation,” “The Ten Domains,” “trauma-informed care,” “mental health,” “emergent,” “pediatric,” “violent,” and “verbal de-escalation,” “confidence”, “competency”, “comfortability”.
Antonia Benton, BSN, RN, is a Doctor of Nursing Practice–Psychiatric Mental Health Nurse Practitioner (DNP‑PMHNP) student at the University of Oklahoma Fran and Earl Ziegler College of Nursing, with expected graduation in May 2026. Her clinical background spans medical and neurological rehabilitation, with specialized experience in spinal cord injury care. She is committed to advancing mental health access for underserved communities, with a developing clinical focus on the treatment of alcohol and substance misuse in adult populations.
Samantha Hemenway, BSN, RN, is a DNP‑PMHNP student at the University of Oklahoma Fran and Earl Ziegler College of Nursing, graduating in May 2026. She brings clinical experience across adult and pediatric psychiatry, grounded in a neuro‑behavioral foundation shaped by early work in neurosurgery and neuro‑trauma, including care for brain tumors, cerebrovascular accidents (CVAs), and traumatic brain and spinal cord injuries. Ongoing clinical focus includes supporting neurodivergent individuals and providing developmentally sensitive, equity‑driven mental health care in rural and underserved communities.
References
Healthy Minds Policy Initiative. (2023, November 6). The state of Oklahoma’s behavioral health workforce. https://www.healthymindspolicy.org/research/state-of-workforce-2023
Hudgins, J. D., & Lee, L. K. (2025). The waiting game: Boarding for pediatric mental health emergencies. Pediatrics, 155(3). https://doi.org/10.1542/peds.2024-069841
Georgadarellis, A. G., & Baum, C. R. (2023). De-escalation techniques for the agitated pediatric patient. Pediatric Emergency Care, 39(7), 535–539. https://doi.org/10.1097/PEC.0000000000002989