
Challenges and technology recommendations
- Nursing care of patients with externalized ventricular and lumbar drains is complex and time-intensive.
- Inadequate management places patients are at risk of serious morbidity and mortality
- Advanced technology helps to reduce patient risk and improves the quality of nursing care in neuroscience settings.
MANY YEARS AGO, one of my friends and a fellow neuroscience nurse died as the result of an infection associated with an externalized ventricular device (EVD) to drain cerebral spinal fluid (CSF). Drainage of CSF, a common treatment in the management of patients with increased intracranial pressure with some forms of brain injury, carries a high risk of infection and other issues related to management. As a clinical nurse specialist, I led a team of three neurointensivists and two staff nurses who sought to better understand why these problems occur.
What the research says
In 2012, the American Association of Neuroscience Nurses (AANN) published a guideline for managing cerebral drainage that includes levels of evidence for nursing practice. However, no universal step-by-step protocol exists for clinical nurses actively caring for patients requiring EVDs or lumbar drains (LDs). Despite this gap, nurses working in step-down units and ICUs routinely manage patients with EVDs and LDs.
Although drainage of CSF with these devices can save lives by reducing intracranial pressure and protecting vulnerable brain tissue, Dolmans and colleagues and Kerry and colleagues reported a mortality rate as high as 32.9% at 90 days. Sam and colleagues echoed this statistic, noting that externalized ventricular catheter-related infection rates can range as high as 32.2%. Among these patients, mortality rates can reach 40.8%. Aten and colleagues demonstrated that treating these complications can cost hospitals from $25,000 to $62,000. Ideally, placement of an EVD catheter should occur in a sterile operating room suite, but Zakaria and colleagues reported that the procedure frequently takes place at the bedside in the ICU.
Inconsistent monitoring, leveling, and sampling techniques remain major contributors to preventable infections and drainage errors, which can dramatically increase mortality rates. Standardizing EVD nursing care can help reduce infection and mortality rates.
Although decades of research and multiple professional initiatives have sought to guide the care of patients with EVDs, their influence on day-to-day nursing practice has proved uneven. The 2012 AANN guideline and the 2016 Neurocritical Care Society consensus statement helped establish foundational principles for EVD insertion, infection prevention, and intracranial pressure monitoring, and they inform many organizational protocols and competency programs. Likewise, work by Talibi and colleagues, Zakaria and colleagues, and others contributed important infection prevention bundles and standardized insertion pathways that improved consistency at some centers. (See Insertion, care practices, and troubleshooting.)
Insertion, care practices, and troubleshooting
According to Vieira and colleagues, the insertion and care of externalized ventricular and lumbar drains include the following steps:
- Position head of bed at 30 degrees, with the patient’s head in a neutral position, aligned with the cervical spine to facilitate venous return and reduce intracranial pressure.
- Use a full-body drape and strict surgical aseptic technique during placement.
- Minimize personnel at the patient’s bedside.
- Cleanse the skin with 0.9% saline and chlorhexidine prior to placement.
- Secure the catheter using a chlorhexidine patch, Steri-Strips, and a bio-occlusive dressing.
- Perform cerebrospinal fluid (CSF) sampling only at insertion and then only every 48 hours if infection is suspected.
- Hand-deliver all CSF samples to the lab for immediate processing.
- Change the collection bag when it’s three-quarters full using aseptic technique to reduce infection risk.
- Clamp the drain when the patient is coughing, vomiting, or in pain and during suctioning or repositioning.
- Change the dressing only if its soiled or displaced.
- Re-zero and re-level the transducer every 4 hours, when the catheter is manipulated, and when the patient is repositioned.
- Republished, with permission, from The Royal Children’s Hospital, Melbourne, Australia. rch.org.au. Images and videos subject to copyright. More information at rch.org.au/kidsinfo/fact_sheets
Troubleshooting
The transducer, which creates the externalized ventricular drain waveform, must be connected to a bedside monitor to reveal the intracranial pressure. If it doesn’t produce a waveform, if the waveform varies from an expected pattern, or if no CSF drainage is evident, take the following steps:
- Ensure the tubing is secure and leak-free.
- Check for tubing kinks.
- Ensure that all stopcocks are open.
- If still no drainage, re-level and re-zero the transducer. Improper leveling can cause intracranial hypertension, ventricular collapse, or subdural hematoma.
- Assess patency. Lower the drain and watch for fluctuation in tubing and drainage. In the event of no fluctuation, contact neurosurgery.
- If tubing becomes disconnected, turn the stopcock to off, secure the tubing, and notify neurosurgery.
- Call neurosurgery for color changes in the drained CSF. Blood may indicate cerebral hemorrhage. Cloudy or sedimented CSF may indicate an infection.
- When transporting the patient, clamping the EVD system may be safe if intracranial pressure is less than 20 mmHG and cerebral perfusion pressure (mean arterial pressure – intracranial pressure) is between 60 and 70 mmHg.
However, the current literature also reveals persistent gaps and disagreements that shape clinical practice. Studies by Lord and colleagues, Thamjamrassri and colleagues, as well as Zakaria and colleagues, report wide variations in nursing procedures, such as leveling and re-zeroing the transducer, CSF sampling technique, drain-height management, and troubleshooting catheter obstruction. No consensus exists on the optimal duration an EVD should remain in place, the frequency of sampling, the timing of mobilization, or the degree to which nursing practice requires standardization across different types of ICUs.
Moreover, available guidelines remain predominantly physician-focused and frequently lack the necessary step-by-step, nursing-specific operational detail required for consistent bedside practice. As a result, even well-intentioned policies are interpreted differently across organizations, contributing to practice variability, preventable complications, and ongoing controversy regarding best practices in EVD management. Hepburn-Smith and colleagues highlight the need for technological solutions and more detailed, nursing-specific competencies and protocols to improve safety and consistency in EVD and LD management.
Nursing care of EVDs and LDs
Alrashidi and colleagues and Rotter and colleagues reported the time-consuming nature of EVD and LD management, which requires a 1:1 nurse-to-patient ratio to prevent complications. Although many intensive care environments follow this practice, no national requirement exists. Fried and colleagues published a consensus statement regarding EVD insertion and patient care, but it focused primarily on physicians and didn’t guide nursing-sensitive measures. If not followed properly, these measures can result in devastating consequences, such as infection and improper CSF drainage.
Hepburn-Smith and colleagues outlined protocols for physician insertion of EVDs, as well as instructions for priming the drainage system and nursing recommendations for zeroing, troubleshooting, preventing over- and under-draining, assessment criteria for identifying patients who are deteriorating, and instructions for transporting patients and methods for safety monitoring.
Infection rates
Thamjamrassri and colleagues noted that EVD- and LD-related infections can occur as a result of inconsistencies in physician insertion practices and medication instillation, but nursing care measures—such as CSF sampling, catheter flushes, and catheter dressing care—dramatically impact infection rates. Bedside insertions in emergent situations increases infection risk.
Current guidelines recommend specific limits for I.V. and urinary catheter placement, but this isn’t the case for EVD and LD placement. Aten and colleagues reported that although the risk of EVD-related infections increases as drain placement reaches 5 days or more, potentially at a cost of more than $55,000, no universal recommendations exist regarding length of placement. This concern inspired Chung and colleagues to evaluate EVD discontinuation strategies.
However, in my follow-up survey, I discovered that nursing practices still vary widely in the care of EVDs, especially with regard to length of placement, sampling, and transducer leveling, re-leveling, and zeroing. Pratt and colleagues confirmed these findings.
Survey results
My survey included 300 neuroscience nurses, all members of the AANN. Of these, 42.8% reported roles as neuro ICU nurses and 26.3% described themselves as ICU or critical care nurses. Among all respondents, 48.4% noted that they cared for a patient with an EVD at least 75% of the time. Neuro ICU nurses were most likely to have a patient with an EVD, but confirmed that they didn’t manage EVDs on every shift (See Demographics.)
Demographics
Nurses from various hospital settings participated in a survey of externalized ventricular device management practices.
Over 75% of surveyed nurses reported seeking help in the complex task of preparing, calibrating, or troubleshooting an EVD or LD device. They also said that they spent an average of 2 hours in a 12-hour shift dedicated to care and troubleshooting existing EVD devices and at least 1.5 hours caring for patients with an LD.
Despite the time devoted to the care of these devices, many safety issues remained a concern, placing patients at risk of complications. For example, although nurses reported that they had re-leveled and re-zeroed the device more often than hospital protocol recommended, more than 37% had cared for a patient in which an accidental over-drain occurred more than once.
Reported nursing concerns
In my 2021 survey, nurses reported several concerns related to caring for patients with EVDs and LDs. Approximately 25% said that they felt challenged with regard to determining the type and location of catheter obstructions. Nearly 75% noted inconsistent education related to managing EVDs and LDs. Alrashidi and colleagues noted that many intensive care nurses who care for patients with EVDs do so without adequate education or resources.
Many surveyed nurses expressed concern that current technology doesn’t include alarms for over- or under-draining. They reported that they felt unsure about the devastating effects this may have on intracranial pressure. Nurses also questioned whether the rate of CSF drainage into the burette I.V. set influenced intracranial pressure.
Maintenance and monitoring
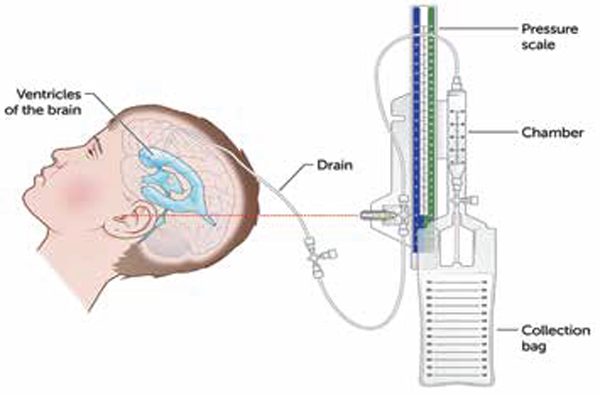
Vieira and colleagues recommend rigorous monitoring of neurologic status using the Glasgow Coma Scale for all patients with an EVD. After CSF drainage is measured, the CSF should be drained from the burette I.V. set into the collection bag. Nurses must document all findings in the electronic health record every hour. Using a quality-control checklist, they should monitor quality of care daily. (See Safety monitoring checklist)
Safety monitoring checklist
A quality control checklist, such as the one below, can help ensure adherence to safety monitoring.
EVD/LD daily safety adherence monitoring
Pt name:
Pt name:
Pt name:
Pt name:
Pt name:
CSF = cerebrospinal fluid, EVD = externalized ventricular device, LD = lumbar drain, MR = medical record
Leveling, zeroing, and sampling
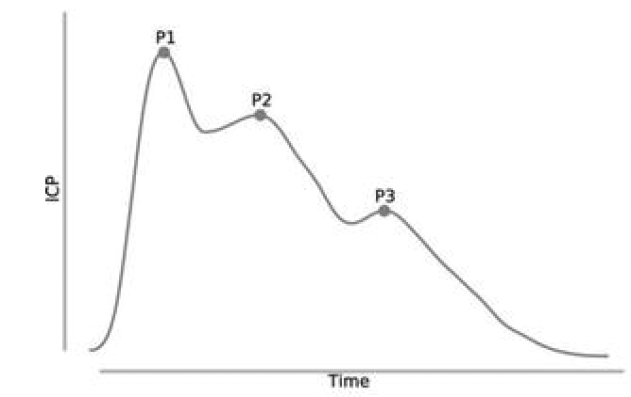
The EVD drainage system is connected to a pressure transducer, which continuously displays the patient’s intracranial pressure as a waveform. Because the transducer measures intracranial pressure relative to a fixed anatomical reference point, it requires accurate leveling to the tragus of the ear—the external landmark corresponding to the foramen of Monro (paired channels that connect the brain’s two lateral ventricles to the third ventricle). (See Figure 2. Normal pressure intracranial pressure tracing)
Figure 2: Normal pressure intracranial pressure tracing
Without precise leveling, even small deviations can introduce errors of ±2 mmHg, potentially obscuring true intracranial pressure trends and influencing clinical decision-making. To ensure ongoing accuracy, nurses must re-level and re-zero the transducer every 4 hours, after patient movement or repositioning, and after CSF sampling.
Upon initial setup, the ICP system is zeroed to calibrate the transducer to atmospheric pressure. Re-zeroing should be completed per institutional protocol.
Because of intracranial pressure sensitivity to patient positioning, changes in the head-of-bed angle can significantly alter readings by affecting cerebral blood flow and venous return. Any change in positioning must include immediate re-leveling and re-zeroing to prevent inadvertent over- or under-drainage and ensure accurate intracranial pressure monitoring.
Improper leveling or failure to re-zero the system can lead to dangerously misleading readings. A transducer positioned too high may falsely lower the displayed intracranial pressure, delaying recognition of intracranial hypertension, whereas a transducer positioned too low may inaccurately elevate the pressure reading and prompt unwarranted interventions.
CSF sampling should occur only when clinically indicated, such as in response to acute changes in neurological status, new vital sign instability, or noticeable alterations in CSF color or clarity. Each sampling event carries an inherent risk of contamination and temporarily disrupts the drainage system and should be obtained only when indicated via strict sterile technique.
Clinical consequences of measuring variability
Inconsistent nursing practices—particularly in leveling the transducer, monitoring the rate of CSF drainage, and measuring output—drive clinical decisions that can ultimately lead to devastating patient outcomes.
Yataco and colleagues noted that most patients with LDs and EVDs aren’t mobilized due to concerns about over-draining or the risk of clinical deterioration. However, Yataco and colleagues also identified that the risk of not mobilizing patients can lead to poor outcomes. Prolonged bedrest raises the risk of other complications, such as atelectasis, skin breakdown, and deep vein thrombosis.
Transport
Transporting patients poses unique risks and challenges, especially with those who are sedated and intubated. Prior to transport, nurses should empty all drainage from the burette into the drainage collection bag, turn off the flow of CSF at the stopcock and white plate and at the more proximal stopcock, and secure the drainage system to the front of the patient’s gown with tape.
Continuing concerns
EVDs and LDs, essential interventions for managing increased intracranial pressure, require consistent, highly skilled nursing care. Inconsistent transducer leveling, variable CSF sampling practices, and nonstandardized troubleshooting contribute to infection, drainage errors, and preventable complications.
My survey findings reinforced these concerns. Despite increased availability of care bundles and organizational protocols, nurses reported practice variation, uncertainty about troubleshooting, and episodes of accidental over-drainage. The literature and survey data underscore that education, competency-based training, and standardized procedures can help reduce patient risk.
However, even with improved training, the limitations of current drainage technology—particularly the lack of built-in safeguards to prevent over- or under-drainage and the need for frequent re-leveling—constrain safe practice and impede patient mobility. These findings highlight the need for ongoing standardization of nursing care and technological innovations capable of providing more reliable, automated, and mobility-friendly CSF drainage systems.
Strategies for improvement
Because of the time-intensive nature of caring for patients with CSF drainage devices, nursing competency alone can’t overcome system-level vulnerabilities. Advances in device engineering are a logical next step, including two specific, literature-informed strategies.
First, the development of closed CSF sampling systems would reduce circuit disconnections, minimize contamination risk, and address persistent infection-prevention challenges. Second, implementing automated or wearable self-leveling transducers calibrated to the foramen of Monro would eliminate the need for frequent manual re-leveling and allow safe patient mobilization, thereby reducing complications associated with immobility.
Integrating these innovations with standardized nursing competencies has the potential to substantially enhance the safety, efficiency, and reliability of EVD and LD care.
Millie Hepburn is a neuroscience nurse scientist and associate professor of nursing at Sacred Heart University in Fairfield, Connecticut.
American Nurse Journal. 2026; 21(5). Doi: 10.51256/ANJ052615
References
Alrashidi Q, Al-Saadi T, Alhaj AK, Diaz RJ. The role of nursing care in the management of external ventricular drains on the neurosurgical ward: A quality improvement project. World Neurosurg. 2023;176:265-71.e2. doi:10.1016/j.wneu.2023.05.016
Aten Q, Killeffer J, Seaver C, Reier L. Causes, complications, and costs associated with external ventricular drainage catheter obstruction. World Neurosurg. 2020;134:501-6. doi:10.1016/j.wneu.2019.10.105
Censullo JL. External Ventricular Drain (EVD) Monitoring. American Association of Neuroscience Nurses. aann.org/uploads/Neuroscience_Resources/EVD.pdf
Chung DY, Thompson BB, Kumar MA, et al. Association of external ventricular drain wean strategy with shunt placement and length of stay in subarachnoid hemorrhage: A prospective multicenter study. Neurocrit Care. 2022;36(2):536-5. doi:10.1007/s12028-021-01343-9
Dolmans RGF, Harary M, Nawabi N, et al. External ventricular drains versus intraparenchymal pressure monitors in the management of moderate to severe traumatic brain injury: Experience at two academic centers over a decade. World Neurosurg. 2023;178:e221-9. doi:10.1016/j.wneu.2023.07.037
Fried HI, Nathan BR, Rowe AS, et al. The insertion and management of external ventricular drains: An evidence-based consensus statement: A statement for healthcare professionals from the neurocritical care society. Neurocrit Care. 2016;24(1):61-81. doi:10.1007/s12028-015-0224-8
Hepburn M. Nursing Perspectives on the Management of Externalized Ventricular Drains (EVDs). Paper presented at: International Neuroscience Research Symposium. January 19, 2024.
Hepburn-Smith M, Dynkevich I, Spektor M, Lord A, Czeisler B, Lewis A. Establishment of an external ventricular drain best practice guideline: The quest for a comprehensive, universal standard for external ventricular drain care. J Neurosci Nurs. 2016;48(1):54-65. doi:10.1097/JNN.0000000000000174
Kerry G, Holtmannspoetter M, Kubitz JC, Steiner HH. Factors which influence the complications of external ventricular cerebrospinal fluid drainage. Acta Neurochir. 2022;164(2):483-93. doi:10.1007/s00701-021-05007-7
Lord AS, Nicholson J, Lewis A. Infection prevention in the neurointensive care unit: A systematic review. Neurocrit Care. 2019;31(1):196-210. doi:10.1007/s12028-018-0568-y
Pratt KA, Peacock SH, Yost KD, Freeman WD, Collins CI, McLaughlin DC. Zero-calibrating external ventricular drains: Exploring practice. J Neurosci Nurs. 2022;54(1):2-5. doi:10.1097/JNN.0000000000000622
Rotter J, Carlstrom LP, Graffeo CS, et al. Streamlining the external ventricular drain and intracranial pressure monitor procedural setup: A quality Improvement Initiative. World Neurosurg. 2022;166:e475-e483. doi:10.1016/j.wneu.2022.07.034
Sam JE, Lim CL, Sharda P, Wahab NA. The organisms and factors affecting outcomes of external ventricular drainage catheter-related ventriculitis: A Penang experience. Asian J Neurosurg. 2018;13(02):250-7. doi:10.4103/ajns.AJNS_150_16
Talibi SS, Silva AH, Afshari FT, et al. The implementation of an external ventricular drain care bundle to reduce infection rates. Br J Neurosurg. 2020;34(2):181-6. doi:10.1080/02688697.2020.1725436
Thamjamrassri T, Yuwapattanawong K, Chanthima P, et al. A narrative review of the published literature, hospital practices, and policies related to external ventricular drains in the United States: The external ventricular drain publications, practices, and policies (EVDPoP) study. J Neurosurg Anesthesiol. 2020;34(1):21-8. doi:10.1097/ANA.0000000000000694
Vieira TW, Sakamoto VTM, Araujo BR, Pai DD, Blatt CR, Caregnato RCA. External ventricular drains: Development and evaluation of a nursing clinical practice guideline. Nurs Rep. 2022;12(4):933-44. doi:10.3390/nursrep12040090
Yataco RA, Arnold SM, Brown SM, et al. Early progressive mobilization of patients with external ventricular drains: Safety and feasibility. Neurocrit Care. 2019;30(2):414-20. doi:10.1007/s12028-018-0632-7
Zakaria J, Jusue-Torres I, Frazzetta J, et al. Effectiveness of a standardized external ventricular drain placement protocol for infection control. World Neurosurg. 2021;151:e771-e777. doi:10.1016/j.wneu.2021.04.113
Keywords: neuroscience nursing care, externalized ventricular drains, lumbar drains


















