ECMO Cannula Safety Bundle: A Nurse-Driven Quality Improvement Initiative to Prevent Migration and Dislodgement
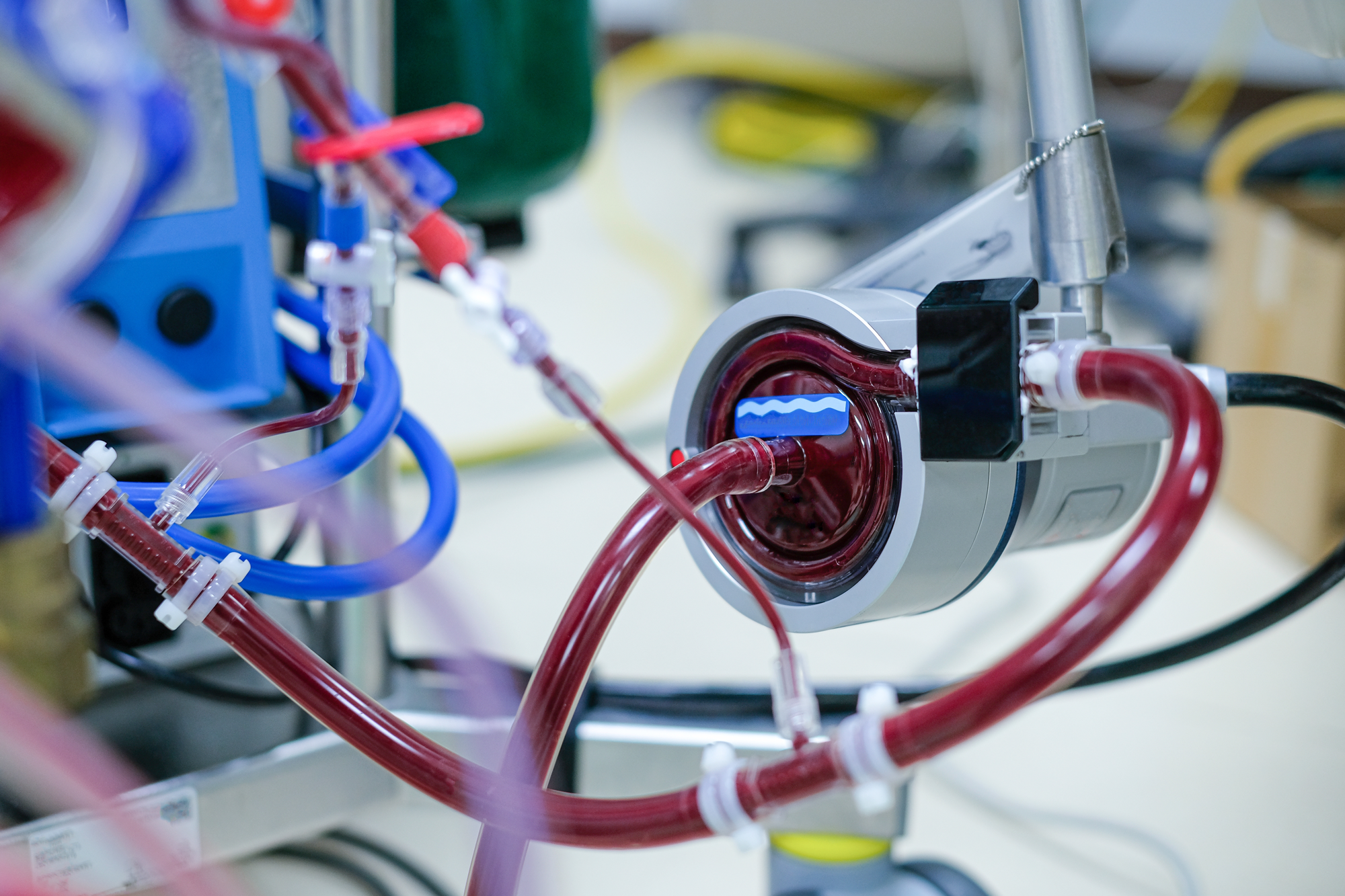
Extracorporeal Membrane Oxygenation, or ECMO, is a critical life-saving intervention for patients experiencing severe cardiac or respiratory failure (Makdisi & Wang, 2015; Brogan et al., 2017). Over the past decade, ECMO use has grown substantially, with many centers, including NewYork-Presbyterian (NYP), which saw an increase of 150% in ECMO cases from 2022 to 2024, which mirrors worldwide trends (Bull et al., 2019; ELSO, 2017). This growth reflects advances in technology and expanding indications for ECMO support. As a result of this increased usage, increasingly complex nursing responsibilities are required to maintain patient safety. (Parrett et al., 2024; Van Kiersbilck et al., 2016). Among these responsibilities, the surveillance of ECMO cannulas, large-bore catheters essential for extracorporeal support, is of paramount importance. Even subtle shifts, known as migration, cannula position can compromise blood flow, increase recirculation, or threaten vascular integrity. Dislodgement, defined as partial or complete exit from the vessel, can have catastrophic consequences, including bleeding, ECMO circuit failure, cardiovascular collapse, and death (Lucchini et al., 2023; Moayedifar et al., 2025; Asermily et al., 2023).
Despite the clinical significance of cannula migration and dislodgement, the literature reveals considerable variability and lack of standardization in preventing and addressing these potentially fatal complications (Bull et al., 2019; Lucchini et al., 2023). The Extracorporeal Life Support Organization (ELSO) provides general guidelines, yet no standardized framework exists for nursing surveillance of cannula position. In practice, monitoring techniques, documentation, and securement practices vary widely among institutions. (Bull et al., 2019; Lucchini et al., 2023).
In our 20-bed Cardiothoracic Intensive Care Unit (CTICU), a cannula dislodgement event in April 2024 underscored the need for improved surveillance and standardized practice. A root cause analysis revealed that inconsistencies in measurement, documentation, and securement processes contributed to the risk, signaling an opportunity for a nurse-driven quality improvement initiative.
In response to these findings, an interdisciplinary ECMO Committee at NYP was created to develop a structured solution. The committee consisted of Nurse ECMO Champions — bedside nurses selected for their clinical expertise and leadership — and was joined by clinical nurse specialists, perfusionists, CTICU intensivists, and cardiothoracic surgeons. Together, they developed the NYP ECMO Cannula Safety Bundle, a multidisciplinary project designed to enhance nursing surveillance, promote early recognition of cannula migration, and reduce dislodgement events. Central to the project’s design was leadership of Nurse ECMO Champions, who led education, audits, and mentorship. The bundle drew on ELSO guidelines, existing institutional protocols, and published evidence, but was carefully tailored to the realities of our CTICU workflow and patient population (ELSO, 2017; Asermily et al., 2023; Parrett et al., 2024).
The Safety Bundle emphasized four critical nursing actions: measuring, documenting, securing, and escalating. Nurses assessed and recorded the external length of each cannula at shift changes, after any patient mobilization, patient transportation, or bed turns. Documentation in EMR included cannula length in centimeters, along with the time, date, and witness signature to reinforce accountability and interprofessional collaboration. Securement devices were inspected and reinforced to anchor cannulas, while nurses routinely monitored cannula insertion sites for bleeding or hematoma as well as cannula tension. All measurement changes or concerning clinical findings triggered immediate escalation to providers. This framework provided a clear, actionable pathway for nurses to intervene early, enhancing patient safety and reducing the likelihood of catastrophic events (Asermily et al., 2023; Moayedifar et al., 2025).
Education and reinforcement were key to implementation. ECMO Champions conducted hands-on training in cannula measurement using anatomical landmarks, proper securement device application, and standardized documentation procedures. Visual guides and step-by-step materials support learning and help maintain consistency across staff. Champions also performed bedside audits using checklists aligned with ELSO and institutional protocols. These audits provided real-time feedback, reinforced best practices, and offered opportunities for mentorship. Limited staffing, however, constrained audit frequency, highlighting the practical challenge of sustaining continuous oversight in a busy CTICU (Parrett et al., 2024; Van Kiersbilck et al., 2016).
Integration with electronic medical records played a pivotal role in sustainability. The ECMO Committee partnered with the hospital’s informatics team to create dedicated Epic flowsheets for ECMO patients, capturing cannula measurements at key intervals, including shift changes, patient transportation, and mobilization with physical or occupational therapy. The flowsheets included prompts for witness verification by an RN, provider, or perfusionist. Embedding these processes within existing workflows helped standardize practice, reduce variation, and support long-term adherence (Asermily et al., 2023).
To evaluate the impact of the bundle, a retrospective audit of 31 ECMO runs from September 2024 to September 2025 was conducted. Four additional cases were excluded due to ongoing ECMO support, locked medical records, or changes in patient identifiers, representing a limitation in data completeness. Each measurement opportunity was assessed for documentation compliance and completeness relative to clinical events. Instances in which ECMO Champions corrected previous measurement inaccuracies were considered potential migration events, as true migration could not be definitively excluded.
Overall, compliance with cannula measurement documentation averaged 78.2%, with shift-change compliance reaching 93.5%. Compliance during patient mobilization with physical or occupational therapy (PT/OT) was 84%. Cannula migration was identified in 61.5% of ECMO runs, with a total of 44 migration events recorded among 19 patients. Most migrations occurred during routine nursing care or shift changes, while none occurred during PT/OT or patient transport. Escalation to providers occurred in 50% of identified migration events. Notably, only one dislodgement event occurred, requiring immediate surgical intervention, and the patient recovered hemodynamic stability after bedside correction.
These findings provide several important insights. First, cannula migration is more common than previously appreciated, even under the care of experienced nurses. Systematic measurement and documentation allow for early recognition of subtle changes before they progress to dislodgement. Second, nurse-led initiatives, particularly when supported by champions and interprofessional collaboration, are effective in standardizing practice and promoting safety. Third, embedding evidence-based practices into electronic workflows and providing structured audits and mentorship are critical to sustainability (Parrett et al., 2024; Van Kiersbilck et al., 2016).
Challenges emerged during implementation, primarily related to staffing limitations. Continuous audits were not always feasible, leading to potential gaps in surveillance. Variability in early measurement techniques contributed to potential overestimation of migration events, though ongoing education and peer mentorship helped address these gaps without resorting to punitive oversight. These experiences reinforced the importance of fostering a culture where nurses feel ownership over quality improvement, rather than scrutiny, and highlighted that sustainability depends as much on organizational culture as on protocols and checklists (Parrett et al., 2024).
This project illustrates the unique insights nurses bring to quality improvement. Nurse ECMO Champions shaped the bundle to fit the practical realities of bedside care, anticipating barriers and designing creative solutions. Their engagement ensured that the initiative was not just a policy change, but a practical, replicable approach that integrates seamlessly into patient care. Other units and institutions can learn from this model, adapting the principles of standardized measurement, documentation, and securement to their own patient populations and workflows (Asermily et al., 2023; Bull et al., 2019).
From a broader perspective, the initiative underscores the value of nurse-led quality improvement in high-risk clinical environments. The high prevalence of cannula migration observed in our audit, coupled with strong compliance with documentation and measurement protocols, supports the notion that structured, evidence-informed nursing interventions can directly enhance patient safety. Leadership support, structured education, and interprofessional collaboration were all essential elements in achieving these results (Parrett et al., 2024; Van Kiersbilck et al., 2016).
Ultimately, the ECMO Cannula Safety Bundle demonstrates that targeted, nurse-led interventions can reduce variability in practice, enhance early detection of cannula migration, and prevent life-threatening dislodgement events. This project revealed that cannula migration in ECMO patients is more common than previously recognized, making systematic measurement, surveillance, and documentation essential for early detection and prevention. Nurse-led initiatives supported by interprofessional collaboration, embedded workflows, structured mentorship, and regular audits proved effective in standardizing practice and enhancing patient safety. Empowering nurses to lead quality improvement leverages their practical insights, ensuring initiatives are both feasible and impactful at the bedside. The bundle serves as a replicable model for improving patient safety in high-risk clinical settings, demonstrating that well-designed, evidence-informed nursing interventions can significantly improve outcomes and strengthen the role of nurses as leaders in clinical practice (Asermily et al., 2023; Parrett et al., 2024; Van Kiersbilck et al., 2016).
References
Asermily B, Smith K, Owen L, Gosev I, Magnuson R. 33: Better secure than sorry: developing evidence-based best practice guidelines for ECMO cannula securement. ASAIO J. 2023;69(Suppl 3):40. doi:10.1097/01.mat.0000990808.58799.54
Brogan TV, Lequier L, Lorusso R, MacLaren G, Peek G. Extracorporeal Life Support: The ELSO Red Book. 5th ed. Extracorporeal Life Support Organization; 2017.
Bull T, Corley A, Lye I, Spooner AJ, Fraser JF. Cannula and circuit management in peripheral extracorporeal membrane oxygenation: an international survey of 45 countries. PLoS One. 2019;14(12):e0227248. doi:10.1371/journal.pone.0227248
Butt W, Heard M, Peek GJ. Clinical management of the extracorporeal membrane oxygenation circuit. Pediatr Crit Care Med. 2013;14(Suppl 1):S13-S19. doi:10.1097/PCC.0b013e318292ddc8
Extracorporeal Life Support Organization. General Guidelines for All ECLS Cases. 2017. Accessed October 6, 2025. https://www.elso.org/ecmo-resources/elso-guidelines.aspx
Gay SE, Ankney N, Cochran JB, Highland KB. Critical care challenges in the adult ECMO patient. Dimens Crit Care Nurs. 2005;24(4):157-162.
Lucchini A, Elli S, Piovera D, et al. Management of vascular access for extracorporeal life support: a cohort study. J Vasc Access. 2023;24(5):1167–1173. doi:10.1177/11297298211056755
Makdisi G, Wang IW. Extracorporeal membrane oxygenation (ECMO) review of a lifesaving technology. J Thorac Dis. 2015;7(7):E166-E176.
Moayedifar R, Schachl J, Königshofer M, et al. Staying in place: in vitro comparison of extracorporeal membrane oxygenation cannula fixation for dislodgment prevention. J Clin Med. 2025;14(5):1712. doi:10.3390/jcm14051712
Ogrinc G, Davies L, Goodman D, Batalden P, Davidoff F, Stevens D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): revised publication guidelines from a detailed consensus process. BMJ Qual Saf. 2016;25(12):986-992. doi:10.1136/bmjqs-2015-004411
Parrett M, Yi C, Weaver B, et al. Nursing roles in extracorporeal membrane oxygenation. Am J Nurs. 2024;124(11):30-37. doi:10.1097/01.NAJ.0001081100.87718.df
Van Kiersbilck C, Gordon E, Morris D. Ten things that nurses should know about ECMO. Intensive Care Med. 2016;42(5):753-755.