
Although the incidence of central line–associated bloodstream infections (CLABSIs) has decreased, the Centers for Disease Control and Prevention reports that an estimated 30,100 of these infections still occur in the United States each year, resulting in thousands of deaths and adding up to billions in costs. To reduce CLABSIs, nurses need to address quality-control issues and make prevention a daily task.
At Penn State Hershey Medical Center, our 49-bed medical-surgical unit uses central lines for posttransplant medications, I.V. vesicants and antibiotics, and total parenteral nutrition. The unit averages 230 central line patient days per month. To address the issue of CLABSIs, we convened an interprofessional team of nurses, physicians, phlebotomists, and infection prevention experts to implement guidelines and recommendations to reduce central line access. The team collaborated to create the No Central Blood Line Draw program. We used the Plan-Do-Check-Act quality-improvement model to implement changes in physician ordering practices, phlebotomy and nursing workflow, patient education, and charge nurse competency in central line blood draws.
How it works
The unit’s education council members designed an education plan, which included teaching all staff about the risks for infection when a central line is accessed. Charge nurses, the only nurses permitted to perform blood draws from central lines, reviewed the relevant policy and received specialized training in this and capillary blood sampling. Laboratory and phlebotomy staff implemented laboratory specimen bundling and explained the process to staff. Collection times occur every 4 hours beginning at 4 A.M. Any specimens ordered between these collection times are drawn on the next collection cycle. Exceptions include admission laboratory specimens, coding or critically ill patients, stat blood cultures, blood cultures ordered before initiating antibiotics, drug monitoring that occurs at nonstandard lab times, and specimens needed after a blood product transfusion.
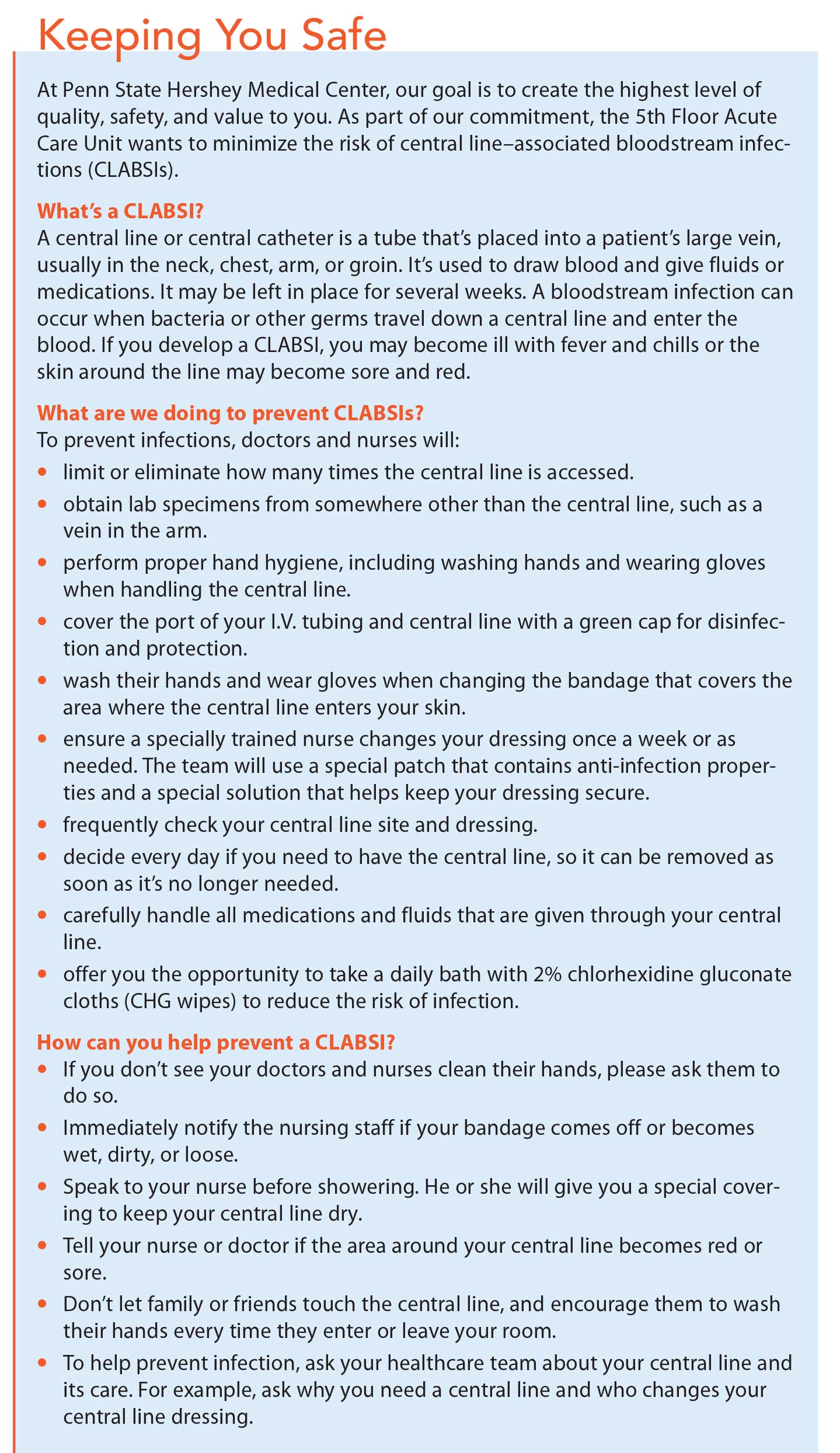
Nurses evaluate all patients with a central line for their willingness to participate in the No Central Blood Line Draw program. Patients naturally prefer having blood drawn from a central line to being “stuck” with a needle, so we teach them about the relationship between accessing central lines for blood specimens and the risk of infection with each occurrence. We also developed a patient education handout describing CLABSIs, strategies used to prevent them, and how patients can participate in their own care. (See Keeping you safe.)
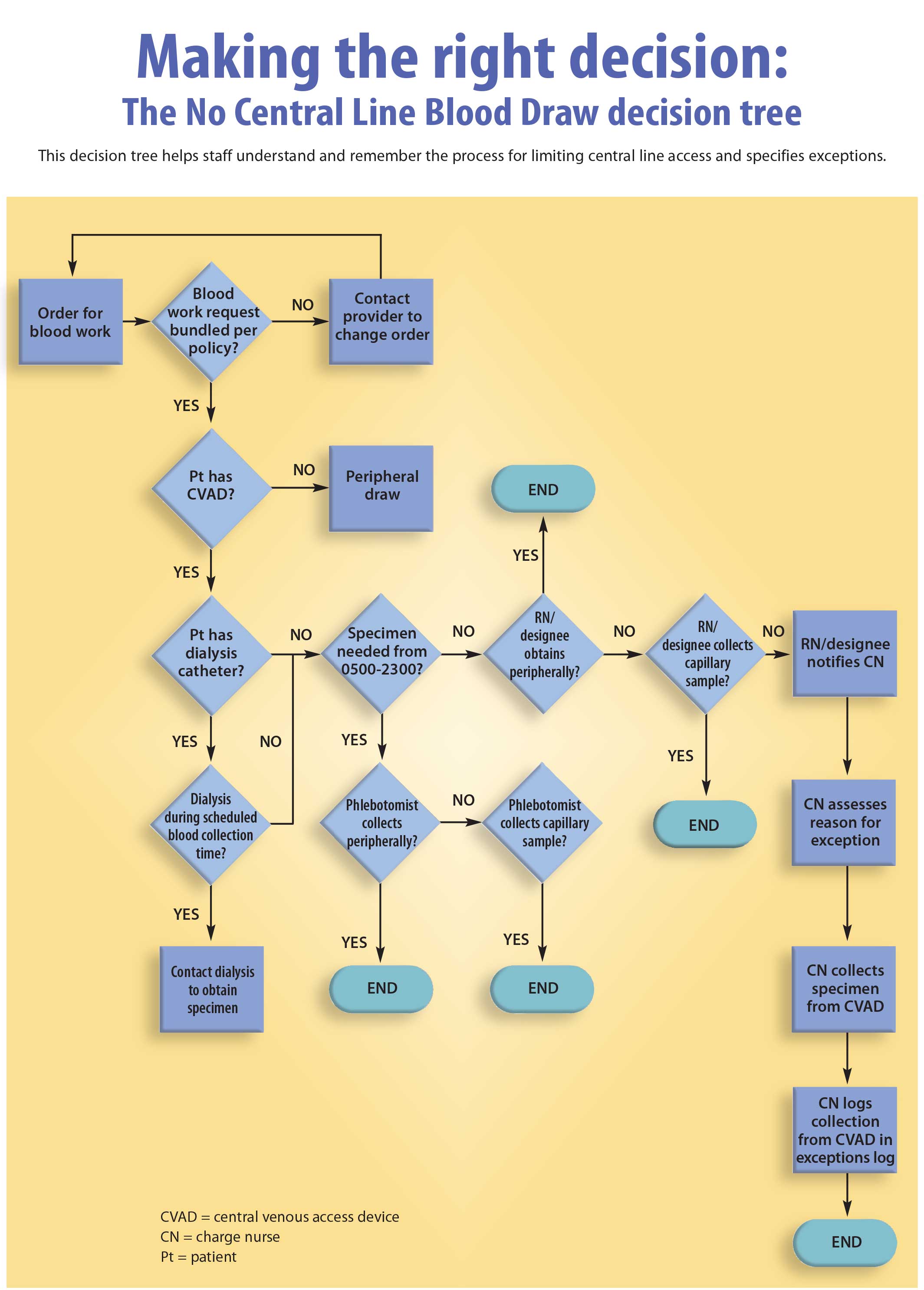
Once patients agree to participate, staff and charge nurses evaluate them for venous accessibility for peripheral blood specimens, and laboratory specimens are bundled and drawn by phlebotomy or nursing staff. We created a process flow chart to provide a visual guide for all staff. (See Making the right decision: The No Central Line Blood Draw decision tree.)
In addition to the steps and exceptions identified in the flow chart, if a specimen can’t be obtained after four attempts or if the patient is identified as having difficult venous access, we evaluate him or her for a foot or capillary blood specimen. If a patient refuses peripheral blood draws despite CLABSI prevention awareness education, or if the patient meets one of the exceptions, the physician orders central line collection. The charge nurse documents this information in the unit charge nurse’s resource book, which contains patients who have had a specimen drawn from their central line and why the line was accessed.
Success
Since implementing No Central Line Blood Draw in October 2014, no participating patient has acquired a CLABSI, down from 2.99 infections per 1,000 central line days. In addition, the number of times central lines were accessed for specimen collection decreased from an average of 6 to 1.4 times per day, and mislabeled or contaminated specimens sent to the laboratory were significantly reduced.
Implementation of this innovative process allowed for interprofessional collaboration and decreased the risk of patients acquiring CLABSIs. The process is now standard practice on the unit, and it’s being evaluated for implementation in other medical-surgical units.
All authors work at Penn State Hershey Medical Center in Hershey, Pennsylvania. Krista Williamson is a nurse manager, Lorie Gonzalez is a nurse educator, Ashley Neusbaum is a clinical head nurse, and Jaime Messing is a staff nurse.
Selected references
Centers for Disease Control and Prevention. Bloodstream infection event (central line-associated bloodstream infection and non-central line–associated bloodstream infection). January 2016.
Centers for Disease Control and Prevention. FAQs about catheter-associated bloodstream infections. (n.d.).
Centers for Disease Control and Prevention. Vital signs: Central line–associated blood stream infections—United States, 2001, 2008, and 2009. MMWR Morb Mortal Wkly Rep. 2011;60(8):243-8.
Marschall J, Mermel LA, Fakih M, et al. Strategies to prevent central line–associated bloodstream infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(7):753-71.
Wilson MZ, Rafferty C, Deeter D, Comito MA, Hollenbeak CS. Attributable costs of central line–associated bloodstream infections in a pediatric hematology/oncology population. Am J Infect Control. 2014; 42(11):1157-60.


















{kind=link}
{kind=link}