
Recognizing and responding to Lyme neuroborreliosis
- Lyme neuroborreliosis presents with a variety of neurological symptoms that may be mistaken for other neurological conditions.
- Nurses’ understanding of appropriate assessment, diagnosis, treatment, and patient education can help ensure a successful outcome.
STEVEN LAIRD*, a 24-year-old electrician, arrives at the emergency department with left facial droop. He tells Stacy, the RN, that while at work he had trouble drinking from a water bottle and his coworker commented on the facial droop. Mr. Laird says that he feels generally fine, except for a headache that’s persisted all day. He also reports some neck stiffness, which he attributes to his work.
The combination of facial droop, persistent headache, and neck stiffness raises concern for neurologic involvement, making these symptoms particularly relevant in the clinical evaluation. Mr. Laird reports no fevers, shortness of breath, visual changes, confusion, slurred speech, head trauma, numbness, weakness, tingling, nausea, vomiting, or abdominal pain. He doesn’t use tobacco, alcohol, or illicit drugs. In his free time, Mr. Laird enjoys hunting and fishing near his Vermont home, which increases his potential exposure to tickborne illnesses. His only significant past medical history is recurrent otitis media as a child, which required bilateral myringotomy with tympanostomy tube placement.
Stacy takes Mr. Laird’s vital signs: temperature 38.4° C, heart rate 78 beats per minute, respiratory rate 16 breaths per minute, blood pressure 116/68 mmHg, and oxygen saturation 99% on room air. Stacy’s physical exam includes the following findings: normocephalic; bilaterally mobile tympanic membranes with normal light reflex; nares patent bilaterally; posterior pharynx without erythema; clear lungs; regular heart rate and rhythm; round, soft, and nontender abdomen; warm, dry, and pink skin; muscle strength +5/5 bilaterally; and limited neck range of motion due to pain (full range of motion bilaterally). Other than the left facial droop, Mr. Laird is alert and oriented x3 and his pupils are equal, round, and reactive to light and accommodation. (See Mr. Laird’s Glasgow Coma Scale and National Institutes of Health Stroke Scale results below)
GCS and NIHSS results
The Glasgow Coma Scale (GCS) objectively measures a patient’s level of consciousness by assessing eye, verbal, and motor responses. Mr. Laird’s score of 15 indicates that he’s fully awake.
The National Institutes of Health Stroke Scale (NIHSS) quantifies stroke severity and recovery. Scores range from 0 to 42; higher scores indicate greater severity. Mr. Laird’s exam shows a score of 3 in only one category (facial palsy), consistent with minor stroke-like symptoms.
Epidemiology and pathophysiology
According to the Centers for Disease Control and Prevention (CDC), Lyme neuroborreliosis is a tickborne illness caused by the spirochete Borrelia burgdorferi. Approximately 476,000 cases occur annually in the United States, with the highest incidence in the Northeast and upper Midwest, which is relevant given Mr. Laird’s outdoor recreational activities in Vermont.
In Mr. Laird’s case, the pathophysiology began with exposure to B. burgdorferi, which likely occurred during a hunting or fishing trip. The bacteria may have moved systemically from the dermal entry site to secondary organs, including the central nervous system (CNS).
Once in the CNS, B. burgdorferi can penetrate the blood–brain barrier and enter the cerebrospinal fluid (CSF), initiating an inflammatory response. This mechanism accounts for the patient’s neurological symptoms (left facial droop, headache, and neck stiffness).
According to Ford and colleagues, the complexity of Lyme disease frequently leads to underdiagnosis, increasing the risk of significant morbidity and mortality. Many early neurological manifestations are subtle or overlap with other conditions.
Symptom presentation
Akkurt and colleagues describe Lyme neuroborreliosis as an uncommon but serious complication of B. burgdorferi infection. Typical presentations include meningitis, cranial neuritis, and radiculoneuritis. However, cases of cerebral vasculitis, ischemic stroke, and encephalitic or cognitive symptoms also have been reported, but rarely. CDC surveillance data show that out of every 100 patients with Lyme neuroborreliosis, nine have facial palsy, four have radiculopathy, and three have meningitis or encephalitis. The Lyme Wellness Initiative states that about 70% of patients with Lyme will experience the classical erythema migrans (bullseye) rash. (See Signs and symptoms.)
Signs and symptoms
According to the Centers for Disease Control and Prevention, signs and symptoms of Lyme neuroborreliosis vary depending on the level of invasion.
- Facial palsy on one or both sides of the face
- “Shooting pain”
- Tingling
- Weakness in the arms or legs
- Fever
- Headache
- Sensitivity to light
- Stiff neck
According to Thaler and colleagues, another mimicking complex symptom to consider is hemiplegic migraine, a genetic and sporadic type of migraine affecting both individuals with and without a family history. It presents with one-sided hemiplegia and other stroke-like symptoms with no associated clinical evidence of stroke on radiographic imaging.
The American Stroke Association recommends evaluation for a cerebrovascular accident (CVA). Common CVA symptoms include numbness or weakness of the face, arm, or leg, especially on one side of the body; confusion; difficulty with speech, vision, or walking; and a severe headache with no known cause.
Nurse’s role in data collection
Nurses collect both subjective and objective data. Subjective information related to Mr. Laird’s hobbies serves as a crucial step in his diagnosis. The patient spends a significant amount of time outdoors participating in high-risk activities related to vector-borne insects. Stacy applies critical thinking and clinical judgement to assess how these activities may increase the risk of Lyme neuroborreliosis, prompting the collection of further information related to outdoor habits, risks of contracting diseases, and potential areas of needed education.
A nurse’s objective assessment is equally important. When considering differential diagnoses, the nurse should weigh the absence of classical symptoms, such as erythema migrans rash, against other presenting factors affecting the central nervous system.
A novice nurse might discount Lyme disease in Mr. Laird’s case because he doesn’t have a rash. Kolchinski and colleagues note that a rash doesn’t usually occur concurrently with Lyme neuroborreliosis symptoms, which don’t manifest until 4 to 7 months after infection; only a reported 35.9% of patients with Lyme neuroborreliosis ever develop a rash after the initial tick bite. Therefore, nurses shouldn’t rule out Lyme disease during assessment and diagnosis based on the absence of a bullseye rash.
Diagnostics
Volk and colleagues note that patients with suspected Lyme neuroborreliosis will receive evaluation via computed tomography (CT) of the head and magnetic resonance imaging (MRI) of the brain to rule out neurological conditions with similar symptoms, such as a stroke or mass lesion. The significance of imaging findings lies in their ability to exclude other acute neurological conditions; however, unremarkable imaging doesn’t rule out Lyme neuroborreliosis. No specific patterns on an MRI have been identified in patients with Lyme neuroborreliosis; rather, a constellation of findings may occur. Imaging might show findings consistent with encephalitis, meningitis, myelitis, and other conditions.
Further evaluation of neurologic findings with lumbar puncture and CSF studies may help to exclude other causes of meningitis, but these tests aren’t always necessary. According to the Infectious Diseases Society of America (IDSA), CSF testing serves several purposes. In suspected meningitis, it can provide data related to etiology of disease process. If CSF pleocytosis (typically lymphocytic or monocytic) is evident, testing can aid in providing a metric for treatment efficacy. CSF testing also can serve as a definitive diagnosis of CNS Lyme neuroborreliosis (although results will be negative if it’s limited to the peripheral nervous system). Lyme disease in children may be associated with a pseudotumor-like picture, in which clinical, radiological, or pathological findings indicate a tumor but none exists.
Volk and colleagues note that CSF analysis frequently will reveal lymphocytic pleocytosis, elevated protein concentrations, normal to mildly decreased glucose, and higher mean albumin CSF/serum quotient. Brain biopsy serves as the definitive diagnosis of Lyme neuroborreliosis. However, it’s usually avoided due to its invasiveness.
CSF testing, according to Halperin and colleagues, can help rule out other possible neurologic conditions in the differential diagnosis. Direct organism detection in the CSF has a low diagnostic sensitivity of <20% and isn’t recommended for routine use. This is likely secondary to low spirochete numbers in the CSF. IDSA and Halperin and colleagues recommend serum anti-BBss antibody testing for patients with suspected Lyme neuroborreliosis. An enzyme-linked immunosorbent assay (ELISA) screening test is performed first, with reflex to IgM and IgG immunoblots. The IgM is considered positive in the presence of >2 of the following bands: 24 kDa, 39 kDa, and 41 kDa. The IgG is considered positive if >5 of the following bands are present: 18 kDa, 21 kDa, 28 kDa, 30 kDa, 39 kDa, 41 kDa, 45 kDa, 58 kDa, 66 kDa, and 93 kDa.
Halperin and colleagues note limitations in using serologic testing to diagnose Lyme neuroborreliosis. Initially, infected patients may be seronegative as the body may have no measurable serum antibody for 4 to 6 weeks after being bitten by an infected tick. The time needed for the host to develop an immune response may occasionally overlap with the initial presentation of Lyme neuroborreliosis. In addition, positive antibody results can last for years, making determination of acute vs previous infection difficult.
Mr. Laird’s diagnosis
As Stacy prepares Mr. Laird for admission, he mentions that he shot a 10-point buck during hunting season a couple of months ago. His symptoms of cranial nerve palsy, neck stiffness, and headache in addition to his recent history of hunting leads Stacey to suspect Lyme neuroborreliosis, which she mentions to the provider preparing to admit Mr. Laird.
A chest x-ray is performed to rule out other causes of constitutional symptoms, although none were severely present and found to be within normal limits. A CT scan of Mr. Laird’s head, without contrast, to evaluate for CVAs shows no acute process. A complete blood count, comprehensive metabolic panel, and lactate level rule out infection and inflammatory processes.
The provider consults neurology, which orders additional laboratory studies, including Lyme serology and lumbar puncture. CSF reveals pleocytosis and positive B. burgdorferi antibodies. Lyme serology also results in positive B. burgdorferi antibodies and positive Lyme IgM bands 24 kDa, 39 kDa, and 41 kDa. IDSA supports obtaining CSF to evaluate for pleocytosis, elevated protein, hypoglycorrhachia to assist in distinguishing Lyme neuroborreliosis from meningitis, and other central nervous system infections. The diagnostic findings, positive Lyme serology, and clinical judgment lead the providers to diagnose Mr. Laird with Lyme neuroborreliosis.
Treatment
The CDC recommends I.V. ceftriaxone (2 g/day for 14 to 21 days depending on illness severity) for patients with suspected or confirmed Lyme neuroborreliosis with facial palsy. When the patient is stabilized for discharge, the provider can transition them to oral doxycycline 100 mg twice daily for 14 to 21 days.
Treatment for Lyme meningitis or radiculoneuritis involves doxycycline or ceftriaxone. IDSA recommended treatment for patients with symptoms of meningitis, cranial neuropathy, or radiculoneuropathy or with other peripheral nervous system manifestations includes I.V. ceftriaxone, cefotaxime, penicillin G, or oral doxycycline over other antimicrobials. Providers should base antibiotic treatment decisions on individual patient circumstances, such as side effects, ability to tolerate medications, and adherence.
Nursing management and implications
Nursing management of patients with Lyme neuroborreliosis directly affects outcomes by enabling early recognition of symptoms and facilitating prompt differentiation from other diagnoses such as migraines, mass lesion, viral/bacterial/fungal meningitis (not secondary to B. burgdorferi), or CVA. Nurses’ clinical judgment and use of IDSA recommendations play a critical role in educating patients about potential complications of Lyme neuroborreliosis, relapse monitoring, and when to seek medical attention during and after treatment.
Timely detection and intervention improve the likelihood of favorable neurologic recovery and minimize potential complications. To achieve these outcomes, nurses perform frequent and thorough neurological exams to monitor patient symptoms and detect changes.
According to the CDC, nurse vigilance includes ongoing assessment and interpretation of symptoms during and after treatment. Ongoing assessment involves applying clinical judgment to identify subtle and clear indicators of disease progression, such as persistent or worsening headache, cranial nerve deficits (for example, facial palsy), radicular pain, sensory disturbances, cognitive changes, fatigue, and gait instability.
Walker describes the nurse’s patient education role in preventing disease relapse or progression. Education about a patient’s antibiotic regimen includes assessing the patient’s ability to obtain the antibiotic, as well as the importance of adherence, possible side effects, and response to treatment.
Consistent with IDSA recommendations, nursing management also includes increasing awareness of tick bites and tickborne pathogens and teaching patients about preventive measures and strategies to reduce exposures. Using their clinical judgement, nurses anticipate complications, monitor for disease progression, and provide personalized patient education, which contribute to improved long-term health outcomes. (See Prevention education.)
Prevention education
Avoiding tick bites remains the most crucial step in Lyme disease prevention. The Lyme Wellness Initiative recommends using tick repellents and dressing for tick safety.
- Treat clothing with permethrin, an insecticide that kills ticks and mosquitoes. Do not apply it to skin.
- Wear light-colored clothing and a hat.
- Tuck long-sleeved shirts into pants.
- Tuck long pants into socks.
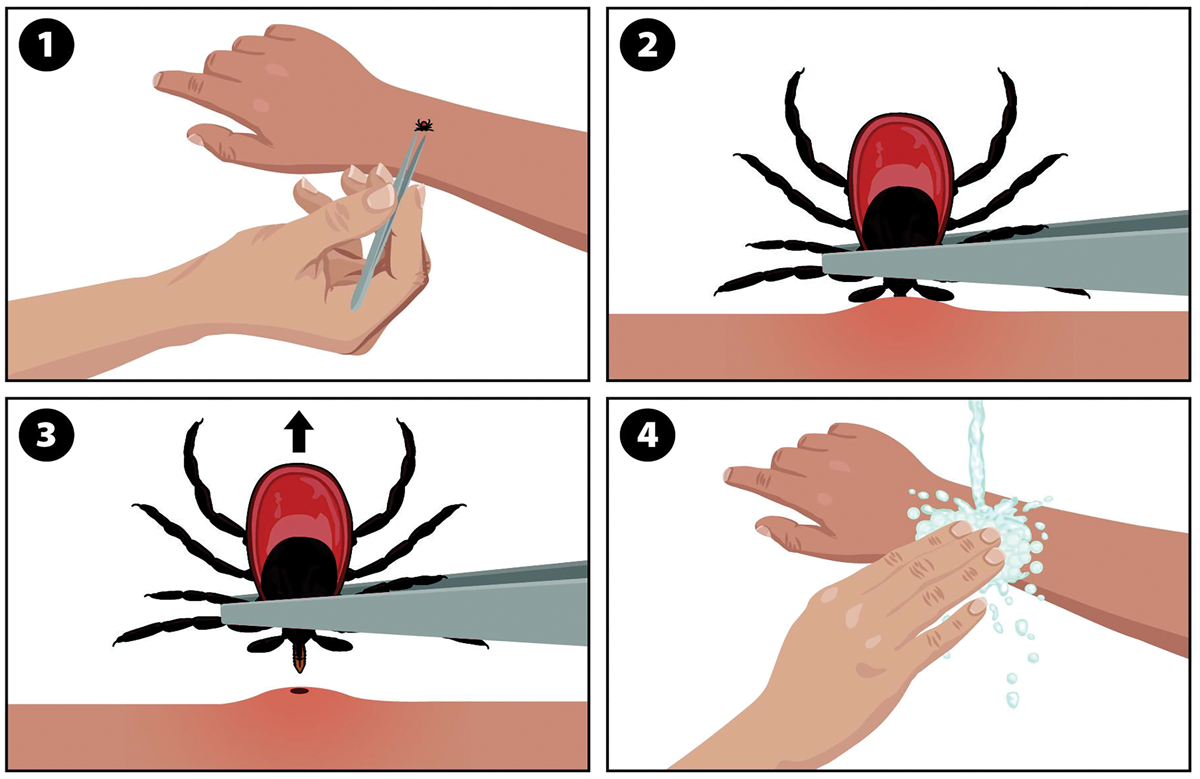
How to safely remove a tick
The Centers for Disease Control and Prevention recommends the following tick removal steps:
- Use clean fine-tipped tweezers.
- Grasp the tick close to the skin’s surface.
- Pull the tick away from the skin in an upright motion.
- After removal, place the tick in a sealed container, on a piece of tape, in a dish of alcohol, or flush it down the toilet.
- Clean the bite area and wash hands.
- Check other areas for tick bites.
Disclaimer: Use of this image and associated links do not imply endorsement by the Centers for Disease Control and Prevention, Health and Human Services, the United States government, the authors, or this journal. The material is available on the CDC website at no charge.
Clinical reasoning and thorough assessment
Nurses’ critical role in the differential diagnosis of Lyme neuroborreliosis involves systematically synthesizing subjective and objective data, recognizing atypical and evolving neurologic presentations, and differentiating the condition from other neurologic disorders. Through advanced clinical reasoning and thorough assessment, early recognition by nurses facilitates timely intervention, effective symptom management, and targeted patient education, which leads to improving patient outcomes and reinforcing nursing’s essential role in complex decision-making.
*Names are fictitious.
Jessica Gregg is an assistant professor of nursing at Saint Francis University in Loretto, Pennsylvania. Kristin Eckenrode is a physician assistant at UPMC in Altoona, Pennsylvania.
American Nurse Journal. 2026; 21(6). Doi: 10.51256/ANJ062641
References
Akkurt BH, Kraehling H, Nacul NG, et al. Vasculitis and ischemic stroke in Lyme neuroborreliosis—Interventional management approach and literature review. Brain Sci. 2023;13(10):1388. doi:10.3390/brainsci13101388
American Stroke Association. Stroke symptoms. stroke.org/en/about-stroke/stroke-symptomsBeBop Labs. Tips for preventing tick bites. 2023. beboplabs.org/prevention/
Centers for Disease Control and Prevention. Clinical care and treatment of neurologic Lyme disease. March 5, 2025. cdc.gov/lyme/hcp/clinical-care/neurologic-lyme-disease.html
Centers for Disease Control and Prevention. Lyme disease surveillance and data. March 13, 2025. cdc.gov/lyme/data-research/facts-stats/index.html
Centers for Disease Control and Prevention. What to do after a tick bite. July 15, 2025. cdc.gov/ticks/after-a-tick-bite/index.html
Ford L, Tufts DM. Lyme neuroborreliosis: Mechanisms of B. burgdorferi infection of the nervous system. Brain Sci. 2021;11(6):789. doi:10.3390/brainsci11060789
Halperin JJ, Eikeland R, Branda JA, Dersch R. Lyme neuroborreliosis: Known knowns, known unknowns Brain. 2022;145(8):2635-47. doi:10/1093/brain/awac206
Infectious Diseases Society of America. AAN/ACR/IDSA 2020 guidelines for the prevention, diagnosis, and treatment of Lyme disease. November 30, 2020. idsociety.org/practice-guideline/lyme-disease
Kolchinski A, Habis R, Rebman A, Venkatesan A, Aucott J. Neuroborreliosis: A retrospective study of clinical manifestations and quality of life impacts Neurology. 2024;102(7 suppl 1):5595. doi:10.1212/WNL.0000000000205927
Lyme Wellness Initiative. Preventing tick bites. lyme.health.harvard.edu/preventing-tick-bites
Mayo Clinic Staff. Pseudotumor cerebri (idiopathic intracranial hypertension): Symptoms and causes. Mayo Clinic. December 17, 2025. https://www.mayoclinic.org/diseases-conditions/pseudotumor-cerebri/symptoms-causes/syc-20354031
Thaler A, Green L, Lai J, Baskin S, eds. Hemiplegic migraine: symptoms and treatments. American Migraine Foundation. March 25, 2025. bit.ly/4eecLUo
Volk T, Urbach H, Fingerle V, Bardutzky J, Rauer S, Dersch R. Spectrum of MRI findings in central nervous system affection in Lyme neuroborreliosis. Sci Rep. 2024;14:12486. doi:10.1038/s41598-024-63006-x
Walker BW. Malaria still cause for concern. Nurs. 2017;47(11):64-66. doi:10.1097/01.NURSE.0000524773.72085.1c
Key words: Lyme neuroborreliosis, Lyme disease, nursing assessment





1 Comment. Leave new
Thanks you for this content