An individualized, multimodal, and interprofessional approach is key for success.
Takeaways:
- Many pediatric patients experience unnecessary pain because of undertreatment and inadequate pain management after surgery.
- Barriers to pediatric pain management include inadequate provider orders, insufficient time to provide pain medication before a procedure, insufficient premedication orders, and low priority given to pain management by medical staff.
- Nurses can be empowered to overcome these barriers and provide optimal pain management.
CNE
1.4 contact Hours
Learning Objectives
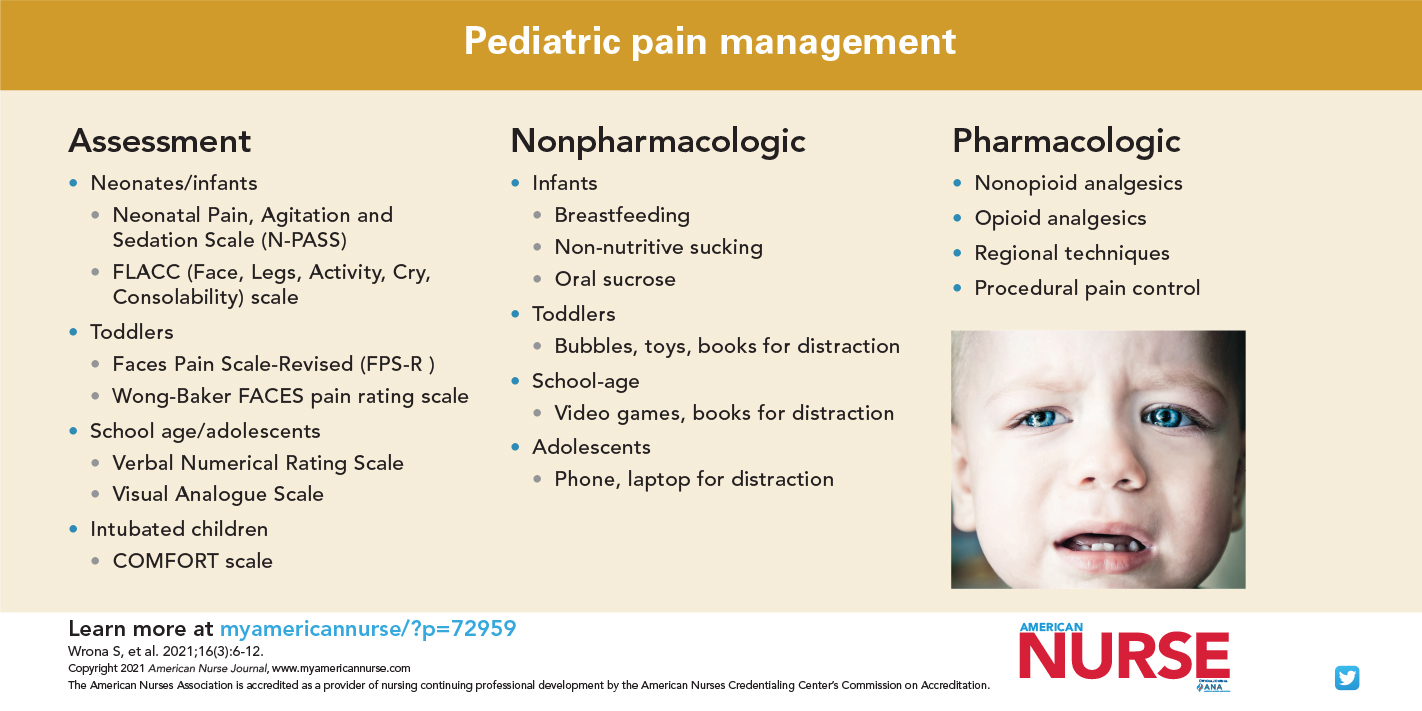
- Identify strategies for assessing pain in children.
- Discuss nonpharmacologic pain interventions for children.
- Describe pharmacologic pain interventions for children.
The authors and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 3/1/24
According to the Healthcare Cost and Utilization Project, more than 5,000,000 children in the United States had a hospital stay in 2017. Many of them experienced some type of pain. Pain has an immense impact on the mind and body. In addition to the physical sensation of pain, effects include emotional suffering, pulmonary complications, decreased mobility, poor sleep, immune impairment, reduced quality of life, economic costs, and a potential for developing persistent (chronic) pain syndromes. Despite advances in care, many children continue to experience significant pain because of undertreatment and inadequate pain management after surgery. Sparing children the short- and long-term effects of pain requires early recognition and treatment.
Nurses are critical to pain prevention, recognition, and treatment in children. They’re with patients more than any other healthcare professionals and have the opportunity to assess pain throughout their shift. When pain is diagnosed, the nurse can start planning which interventions are most appropriate for individual patients. After interventions are implemented, the nurse should reassess the patient’s pain and response to treatment to evaluate intervention effectiveness.
Nurses have identified barriers (many outside of their control) to pediatric pain management. Czarnecki and colleagues’ 2019 multisite study of barriers to pediatric pain management found commonalities across the United States. The most frequently identified barriers included inadequate provider orders, insufficient time to provide pain medication before a procedure, insufficient premedication orders before procedures, and low priority given to pain management by medical staff. Regardless of role or setting, nurses can be empowered to overcome these barriers and provide optimal pain management. For example, they can use the electronic health record to develop order sets that include analgesic options, reducing barriers to adequate and timely orders. At a system level, nurses can collaborate with interprofessional teams on quality improvement projects to remove barriers that are out of the nurse’s control but within the area of other professionals’ work. In the Czarnecki study, concerns about addiction, limitations in nurses’ ability to assess pain, and a low priority given to pain by nursing staff were rated among the least frequently identified barriers.
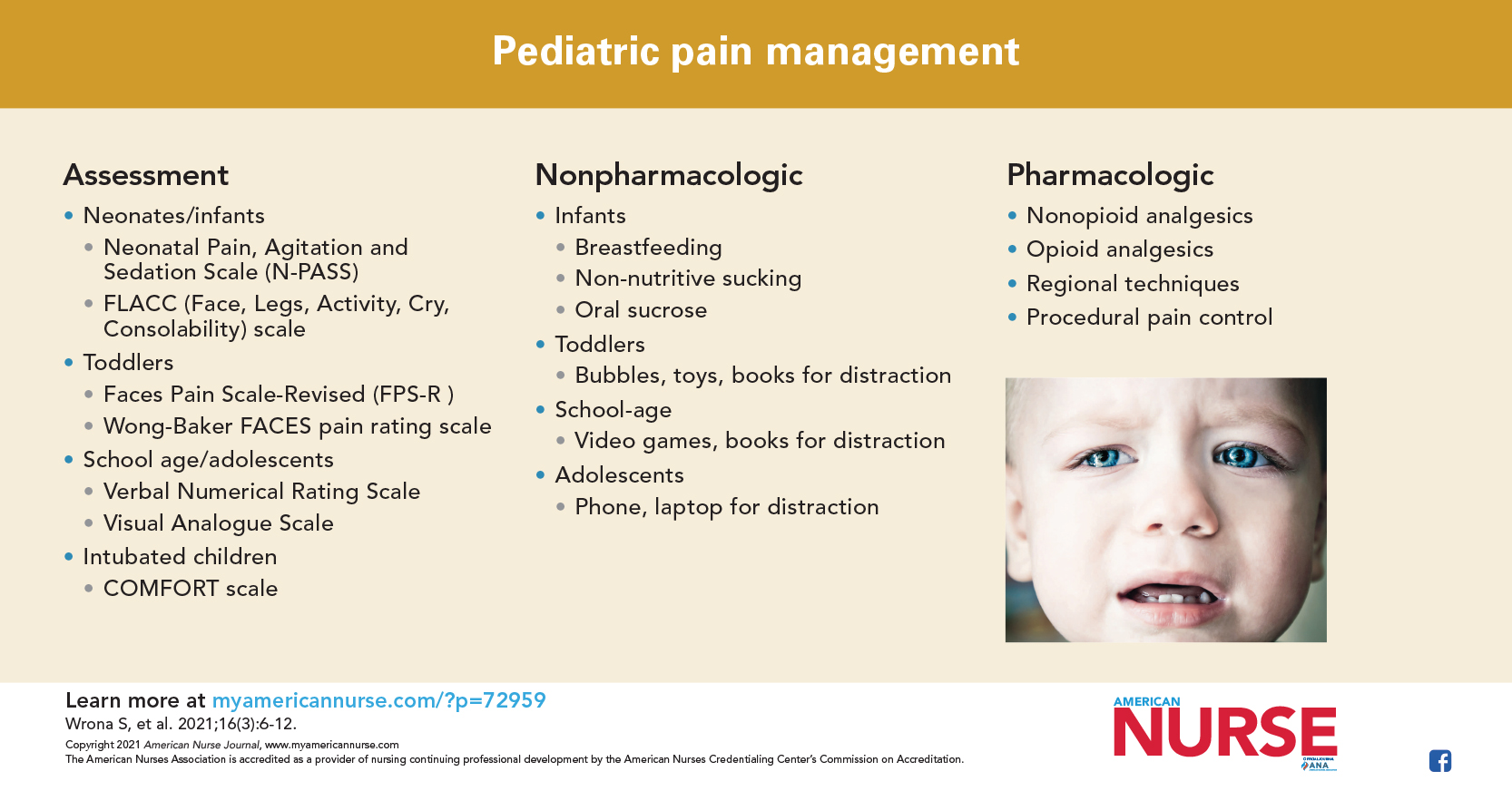
Assessment
Historically, pain intensity numbers were viewed as key to patient assessment, and pain was considered the 5th vital sign. Although this was interpreted as requiring a pain score along with other vital signs, a true pain assessment should capture more than just a number. It should describe the patient’s pain experience, including its nature, impact, and context. Parental input can help differentiate pain from anxiety or other sources of distress in pediatric patients.
Pain intensity ratings are one piece of a pain assessment, but function is more important. Among adult patients, pain intensity ratings are being replaced with multidimensional pain assessments. For example, the Clinically Aligned Pain Assessment Tool guides the conversation between nurse and patient, focusing on general comfort, treatment effectiveness, whether pain is getting better or worse, activity level, and sleep quality. The tool can be adapted for use with children. Not all categories may apply to all pediatric patients, so the tool should be individualized and include parental input.
When used, pain intensity ratings should be gathered with developmentally appropriate, reliable, and validated tools. (See Choosing the right pain scale.)
Choosing the right pain scale
Pain scales have been developed for various pediatric populations. Nurses should select scales that are valid, reliable, user friendly, and easy to incorporate into practice. No matter which scale is used, re-assessment after interventions is a necessary component of the pain management plan.
Neonates and infants
Premature infants, starting around 20 weeks gestation, can perceive and respond to pain. To conserve energy, they frequently show a less-robust physical response compared to full-term infants (for example, they are more likely to close their eyes instead of grimacing and often have lower oxygen saturation levels). This unique response requires a scale specific to premature infants.
- The Premature Infant Pain Profile (PIPP), although less commonly used now because it’s valid only in premature infants ≤ 37 weeks gestation, is well equipped to measure pain in this patient population. The Neonatal Pain, Agitation and Sedation Scale (N-PASS) includes a sedation assessment so that only one scale is needed for infants 23 weeks gestation through 100 days of life. The N-PASS scores pain/agitation from 0 to 10 and sedation from -10 to 0.
- Scales appropriate for full-term and older infants include the Neonatal Infant Pain Scale, the FLACC (Face, Legs, Activity, Cry, Consolability) scale, Child Facial Coding System, CRIES (Crying, Requires increased oxygen administration, Increased vital signs, Expression, Sleeplessness) score, Children’s Hospital of Eastern Ontario Pain Scale, Riley Infant Pain Scale, and Children and Infants Postoperative Pain Scale.
Toddlers
When possible, self-report scales are preferred over behavioral or observational scales in this patient population. When children communicate pain with words (usually by age 3 to 4 years), many can self-report using faces scales.
- Several self-report faces scales exist, each with varying levels of validity and reliability. These scales require the child to point to the face that best depicts their pain level. Examples include Faces Pain Scale-Revised (FPS-R) and Wong-Baker FACES pain rating scale. Nurses should use the same scale with a child rather than alternating between scales. The FPS-R has been used with smartphone technology with some success.
School age and adolescents
Many older children (8 years and older) can self-report pain by using a 0 to 10 scale.
- Numeric rating scales are easy to use and may be verbal (Verbal Numerical Rating Scale) or written (Visual Analogue Scale).
Children with cognitive developmental delays
These children are at increased risk for poor pain assessment and management. Although their pain response may be diminished, no studies have demonstrated a decrease in pain sensation. Voepel-Lewis found that when self-report isn’t possible, facial cues are highly sensitive indicators of postprocedure and postoperative pain. Several scales exist, each with varying levels of reliability and validity.
- The revised FLACC (r-FLACC) has been validated in children from age 4 to 19 years. Using the original FLACC scale as a base, additional indicators (such as head banging and breath holding) were added, along with space for parents to document any features unique to their child.
- Another helpful tool is the Individualized Numeric Rating Scale. Caregivers are asked to assign a number to typical pain behavior seen in their child. The scale must be periodically updated because pain signs may change as the child ages.
Intubated and mechanically ventilated children
Very few validated scales exist for this patient population.
- The COMFORT scale, which Van Dijk and colleagues demonstrated to be reliable and valid, is one of the more commonly used scales in this population. It uses six behavioral and two physiological metrics for a total score from 8 to 40.
- An American Society of Pain Management Nursing position statement recommends using self-report if possible, evaluating potential sources of pain, assessing patient behaviors, incorporating physiologic measures (keeping in mind that they may not be specific to pain), soliciting input from parents, and assuming pain is present if the child is undergoing a painful procedure or has known reasons for pain.
Treating pain in children and adolescents
Pain management should take an individualized, multimodal (nonpharmacologic and pharmacologic), and interprofessional approach. The Pain Management Best Practices Inter-Agency Task Force identified gaps where multimodal, nonopioid treatment options were underused, especially in acute care settings. This report suggests the need for more guidelines, including a multimodal approach.
Nonpharmacologic approaches
Nonpharmacologic approaches to pain treatment should be tailored to the developmental level of the child and their individual needs. Treatment plans should be developed to effectively manage the child’s pain with an overarching goal of improving function. Involving the patient and family in treatment planning is essential for developing realistic expectations and goals.
The Joint Commission standards encourage hospitals to provide nonpharmacologic pain treatment and monitor intervention outcomes. Frequently, acute pain, especially in the hospital, is treated with a combination of nonpharmacologic and pharmacologic options. In contrast, when working with children and adolescents with persistent pain, nonpharmacologic treatment options frequently are the mainstay of pain treatment.
Nonpharmacologic pain interventions can be categorized as behavioral, cognitive, restorative, and complementary. A child life therapist can work with a child before a procedure or surgery to help facilitate therapeutic play and teach behavioral and cognitive techniques they can use throughout their lives to manage pain or uncomfortable situations. These techniques include deep breathing, self-coping skills, guided imagery, and virtual reality. In addition, music and reduced stimulation can create a soothing environment. (See Age-appropriate options.)
Age-appropriate options

Nonpharmacologic pain management interventions should be age-appropriate.
Infants
- Breastfeeding
- Oral sucrose
- Non-nutritive sucking
- Swaying (rocking the infant back and forth)
- Swaddling
Toddlers
- Bubbles, toys, books, or other objects for distraction
- Comfort holds (secure hugging by a parent or caregiver that helps the child feel safe and secure, decreases movement, and allows the parent to appropriately participate in the procedure)
School-age children
- Comfort holds during procedures
- Video games, toys, books, bubbles, and other objects for distraction
Adolescents
- Whenever possible, allow adolescents to use their independence, make choices, and apply coping skills they’ve previously acquired.
- Adolescents may want more privacy or social support from peers and others, compared to other age groups.
- They may prefer technology (phone or laptop) for distraction.
Restorative therapies, such as physical therapy, occupational therapy, and therapeutic recreation, can help restore a child to optimal function when they’re experiencing acute pain. These therapies are essential for children with persistent pain.
According to Brittner and colleagues, complementary and integrative health modalities, such as massage and acupuncture, are showing some promising effects when used as part of a multimodal approach to treat various types of pain in children. Their evidence supports the safe use of acupuncture in children, and findings suggest this type of integrative approach can be beneficial for improving infant colic, headaches, dysmenorrhea, and other types of pain.
For children of all ages, parental involvement to provide comfort and reassurance is beneficial to both the parent and the child. However, nurses must recognize when parent or caregiver stress and anxiety may be upsetting the child. When that’s the case, nurses can help by providing open channels of communication, sharing information, and involving the parent in their child’s care (bathing, comfort holds, distraction) when possible.
Pharmacologic approaches
A variety of medication classes can be used to treat pain in children. The medication selection should consider the nature (for example, physical or emotional, acute or persistent) and intensity of the pain, its characteristics (for example, sharp, dull), and duration.
Nonopioid analgesics. Nonopioid medications, such as acetaminophen (I.V., oral, or rectal) and nonsteroidal anti-inflammatory drugs (NSAIDs) can be used to treat most types of pain. NSAIDs are recommended for mild to moderate pain and as part of a multimodal treatment plan for severe pain when using stronger analgesics such as opioids. Even in the postoperative setting, scheduled acetaminophen and NSAIDs may provide enough analgesia for children to tolerate pain. When any medication (including over-the-counter [OTC] drugs) is administered to a child, doses must be determined based on weight and age. Some OTCs may be contraindicated for children with certain clinical issues, such as liver or kidney disease and bleeding disorders. Nurses should screen for contraindications and teach parents and caregivers how to use nonopioid analgesics appropriately to help manage their child’s pain.
Adjuvant medications (such as tricyclic antidepressants) or anticonvulsants (such as gabapentin) can be used for persistent neuropathic pain. A study by Baxter and colleagues indicates that these medications can help reduce opioid use to treat postoperative pain in pediatric patients. Some pediatric organizations use low-dose ketamine or lidocaine infusions to help manage acute and neuropathic pain. Benzodiazepines can be used in the acute setting to treat muscle spasms; however, these medications can cause sedation and should be used with extreme caution when given in conjunction with opioids or other sedating medications. Medications such as baclofen or tizanidine, which cause less sedation, may be more appropriate for pediatric patients.
Opioid analgesics. Opioids are reserved for managing severe pain. When prescribed for children, opioids are given orally or intravenously. The oral route is easy and inexpensive, and most short-acting opioids are available in a liquid or tablet form. Some oral opioids, such as hydrocodone, are available only as a combination medication (for example, hydrocodone with acetaminophen). When using combination medications that have acetaminophen, nurses must educate parents and caregivers about the maximum daily dose of acetaminophen for their child to prevent unintentional overdose. Nurses should explain to parents that some cold and flu OTC products contain acetaminophen.
I.V. opioids are used for children who can’t tolerate oral formulations and may be administered as an infusion or an intermittent I.V. push as needed. I.V. opioids also can be given via a patient-controlled analgesia (PCA) pump, which allows patients to safely and effectively administer small amounts of opioid within a specified time period. Some pediatric organizations also use PCA pumps for authorized agent-controlled analgesia. This modality allows authorized and educated nurses and/or caregivers to activate the PCA button for children who can’t do so themselves. A 2015 study by Czarnecki and colleagues showed this modality to be safe and effective, although it may not increase parent satisfaction.
Regardless of administration route, nurses should closely monitor children receiving opioids for side effects and adverse reactions, including increased sedation, which may be the first sign of impending opioid-induced respiratory depression. Nurses should take immediate action to decrease or stop the opioid per provider orders. Common opioid side effects include nausea, pruritus, drowsiness, and constipation. Managing side effects is key to patient comfort. If medications are needed to control side effects, the least sedating option should be used. (See Safe opioid use, storage, and disposal.)
Safe opioid use, storage, and disposal
Reducing opioid misuse requires appropriate use for pain control as well as safety precautions in the home.
Appropriate opioid use
In a study by Miech and colleagues, a legitimate opioid prescription predicted future opioid misuse in 12th grade students who had little experience with illegal drug use and strongly disapproved of marijuana use. This increased risk of future opioid misuse must be considered when weighing the risks and benefits of prescribing these medications to children. Opioids are appropriately indicated and necessary in some cases, but if pain can be adequately treated without them, they shouldn’t be prescribed. Nurses have a duty to discuss the risks and benefits of any treatment modality with patients and their families, and to inform providers of any identified risks.
Safe opioid storage and disposal
About 70% of the opioids misused by children are prescribed or obtained for free from a relative or friend. A study of U.S. Poison Control Centers by Allen and colleagues found that an average of 32 calls a day are received for unintentional opioid ingestion by children (more than 50% are age 5 years or younger).
When educating patients and families about opioid safety, nurses should include the following points:
- Secure medications in a locked location. Many retail pharmacies sell medication lockboxes.
- To ensure no medications are missing, keep a log of the number of opioids on hand and given to the child.
- Be on the lookout for opioid seekers, including family members, friends, neighbors, and even strangers, who might want to steal unused medications from the home.
- Transition from opioids to over-the-counter (OTC) pain medications when opioids are no longer needed. For many minor surgeries or injuries, OTC medications may be sufficient to manage pain.
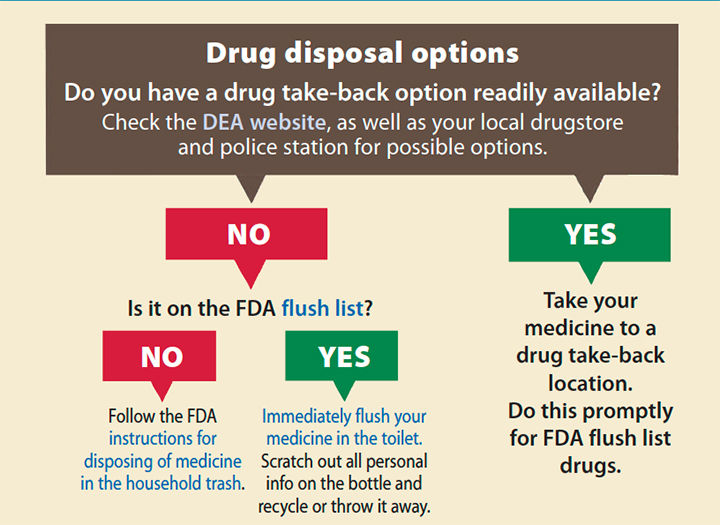
- Unused medications can be disposed of in a medication drop box using a medication disposal bag, taken to a drug take-back program, or disposed of in household trash after mixing them with undesirable substances such as coffee grounds or cat litter. Nurses can direct families to visit the U.S. Food and Drug Administration website for more information fda.gov/Drugs/ResourcesForYou/Consumers/BuyingUsingMedicineSafely/EnsuringSafeUseofMedicine/SafeDisposalofMedicines/ucm186187.htm.
Regional techniques. Regional anesthesia techniques—such as epidural catheters, spinal anesthesia, peripheral nerve catheters, paravertebral catheters, and blocks—can improve postoperative pain control in children and reduce opioid use. Many of these techniques, which are being more widely used in the pediatric population, use local anesthetics and other medications that work directly on the nerves to help block the pain. Local anesthetics are nonsedating and have fewer side effects than opioid medications.
Procedural pain control. Critically ill infants experience between seven and 17 painful procedures per day during neonatal intensive care unit stay. A variety of local and topical anesthetics can be used in conjunction with nonpharmacologic pain management techniques to help comfort children during a procedure. Local anesthetic creams, patches, injections, or sprays should be offered to children before a painful procedure unless contraindicated. Involving parents or caregivers to help with comfort holds can help reduce stress and anxiety during a procedure.
Make a difference
Pain management in children continues to be suboptimal, but nurses can make a difference. Their individualized pain assessment using age-appropriate tools, administration of pharmacologic and nonpharmacologic pain treatments, optimal pain management advocacy, and patient and family education are key to relieving pediatric patients’ pain and improving their quality of life. AN
Click here and here to download visual abstracts for this continuing education article.
Sharon Wrona is director of comprehensive pain and palliative care services at Nationwide Children’s Hospital in Columbus, Ohio. Michelle Czarnecki is a pain management advanced practice nurse at Children’s Hospital of Wisconsin Jane B. Pettit Pain and Headache Center in Milwaukee.
References
Allen JD, Casavant MJ, Spiller HA, Chounthirath T, Hodges NL, Smith GA. Prescription opioid exposures among children and adolescents in the United States: 2000-2015. Pediatrics. 2017;139(4):e20163382. doi:10.1542/peds.2016-3382
American Pain Society. Principles of Analgesic Use in the Treatment of Acute Pain and Cancer Pain. 5th ed. Glenview, IL: American Pain Society; 2003.
Baxter KJ, Hafling J, Sterner J, et al. Effectiveness of gabapentin as a postoperative analgesic in children undergoing appendectomy. Pediatr Surg Int. 2018;34(7):769-74. doi:10.1007/s00383-018-4274-9.
Brittner M, Le Pertel N, Gold MA. Acupuncture in pediatrics. Curr Probl Pediatr Adolesc Health Care. 2016;46(6):179-83. doi:10.1016/j.cppeds.2015.12.005
Czarnecki ML, Hainsworth KR, Jacobson AA, Simpson PM, Weisman SJ. Opioid administration for postoperative pain in children with developmental delay. Parent and nurse satisfaction. J Pediatr Surg Nurs. 2015;4(1):15-27.
Czarnecki ML, Guastello A, Turner HN, Wrona SK, Hainsworth KR. Barriers to pediatric pain management: A brief report of results from a multisite study. Pain Manag Nurs. 2019;20(4):305-8. doi:10.1016/j.pmn.2019.01.008
Crellin DJ, Harrison D, Santamaria N, Babl FE. Systematic review of the Face, Legs, Activity, Cry and Consolability scale for assessing pain in infants and children: Is it reliable, valid, and feasible for use? Pain. 2015;156(11):2132–51. doi:10.1097/j.pain.0000000000000305
Cruz MD, Fernandes AM, Oliveira CR. Epidemiology of painful procedures performed in neonates: A systematic review of observational studies. Eur J Pain. 2016;20(4):489-98. doi:10.1002/ejp.757
Davies RB. Pain in children with Down syndrome: Assessment and intervention by parents. Pain Manag Nurs. 2010;11(4):259-67. doi:10.1016/j.pmn.2009.09.003
Di Maggio T, Clark LM, Czarnecki ML, Wrona S. Pediatric pain management. In: American Society for Pain Management Nursing. Core Curriculum for Pain Management Nursing. 3rd ed. St. Louis, MO: Elsevier, Inc; 2017; 349-423.
Donaldson G, Chapman CR. Pain management is more than just a number [research statement]. Salt Lake City: University of Utah Health/Department of Anesthesiology; 2013. faculty.utah.edu/u0274011-GARY_W_DONALDSON/research/index.hml
Healthcare Cost and Utilization Project. HCUP Fast Facts—Trends in inpatient stays. May 2020. http://bit.ly/38fkkaT
Herr K, Coyne PJ, Ely E, Gélinas C, Manworren RCB. Pain Assessment in the patient unable to self-report: Clinical practice recommendations in support of the ASPMN 2019 position statement. Pain Manag Nurs. 2019;20(5):404-17. doi:10.1016/j.pmn.2019.07.005
Hummel P, Puchalski M, Creech SD, Weiss MG. Clinical reliability and validity of the N-PASS: Neonatal pain, agitation and sedation scale with prolonged pain. J Perinatol. 2008;28(1):55-60. doi:10.1038/sj.jp.7211861
Lalloo C, Stinson JN. Assessment and treatment of pain in children and adolescents. Best Pract Res Clin Rheumatol. 2014;28(2):315-30. doi:10.1016/j.berh.2014.05.003
Lundeberg S. Pain in children—Are we accomplishing the optimal pain treatment? Paediatr Anaesth. 2015;25(1):83-92. doi:10.1111/pan.12539
Miech R, Johnston L, O’Malley PM, Keyes KM, Heard K. Prescription opioids in adolescence and future opioid misuse. Pediatrics. 2015;136(5):e1169-77. doi:10.1542/peds.2015-1364
Stevens B, Johnston C, Petryshen P, Taddio A. Premature infant pain profile: Development and initial validation. Clin J Pain. 1996;12(1):13-22. doi:10.1097/00002508-199603000-00004
Sun T, West N, Ansermino JM, et al. A smartphone version of the Faces Pain Scale-revised and the Color Analog Scale for postoperative pain assessment in children. Paediatr Anaesth. 2015;25(12):1264-73. doi:10.1111/pan.12790
van Dijk M, Peters JWB, van Deventer P, Tibboel D. The COMFORT behavior scale: A tool for assessing pain and sedation in infants. Am J Nurs. 2005;105(1):33-6.
Voepel-Lewis T. The ongoing quandaries of behavioral pain assessment in children with neurocognitive impairment. Dev Med Child Neurol. 2011;53(2):106-7. doi:10.1111/j.1469-8749.2010.03845.x
Wilson CA, Sommerfield D, Drake-Brockman TFE, Lagrange C, Ramgolam A, von Ungern-Sternberg BS. A prospective audit of pain profiles following general and urological surgery in children. Paediatr Anaesth. 2017;27(11):1155-64. doi:10.1111/pan.13256

















{kind=link}
{kind=link}