A nurse’s concern prompts action.
- Hypercalcemia may occur from benign or malignant origins.
- Severe cases of hypercalcemia are considered medical emergencies and must be treated in an inpatient setting.
- If left untreated, hypercalcemia can negatively affect multiple organ systems as well as the bones, leading t renal failure or cardiac arrest, as well as long-term effects such as osteoporosis and bone pain.
- Some patients present with psychiatric disturbances such as lethargy, confusion, obtundation, or coma.
Robert Tanner*, A 69-year-old man arrives in the ED with reports of persistent fatigue, nausea, vomiting, anorexia, excessive thirst, increased urination, and back pain for 3 days. His BP is 170/98 mmHg and HR is 60 bpm.
History and assessment
The ED nurse obtains orders for a CBC, CMP, parathyroid hormone level, vitamin D, urinalysis, and electrocardiogram. Mr. Tanner confirms his medical history includes vitamin D deficiency, hypertension, hyperlipidemia, and osteoporosis. His medications include oral hydrochlorothiazide (HCTZ), oral cholecalciferol, oral atorvastatin, and subcutaneous teriparatide.
Mr. Tanner’s calcium level (13.5 mg/dL) leads the provider to suspect medication-induced hypercalcemia. She discontinues the patient’s HCTZ and teriparatide, which can cause calcium retention and elevate serum levels.
The CBC reveals mild anemia; the ECG and other lab results are within normal limits. After a head, chest, abdomen, and pelvis CT scan, Mr. Tanner is transferred to the med-surg unit.
Taking action
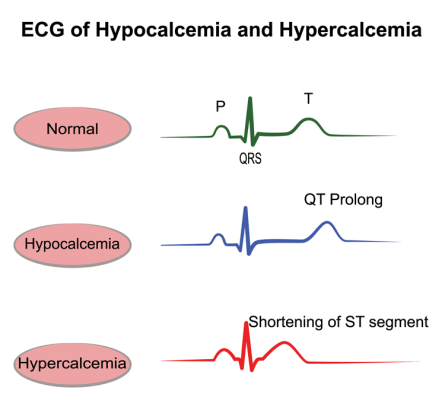
When Mr. Tanner arrives on the unit, his mental status has changed from alert and oriented x4 to alert and oriented to person (his GCS in the ED was 15; it’s now 14). Per admission orders, Wayne, the unit nurse, obtains a repeat serum calcium level, which shows an increase to 14.5 mg/dL. A repeat ECG shows bradycardia with a prolonged PR interval. Vital signs include BP 160/89 mmHg, HR 53 bpm, respiration rate 10 breaths per minute, and SPO2 92% on room air. Mr. Tanner reports mid to lower back pain (8/10). Wayne alerts the inpatient provider and expresses concern about the patient’s mental status changes.
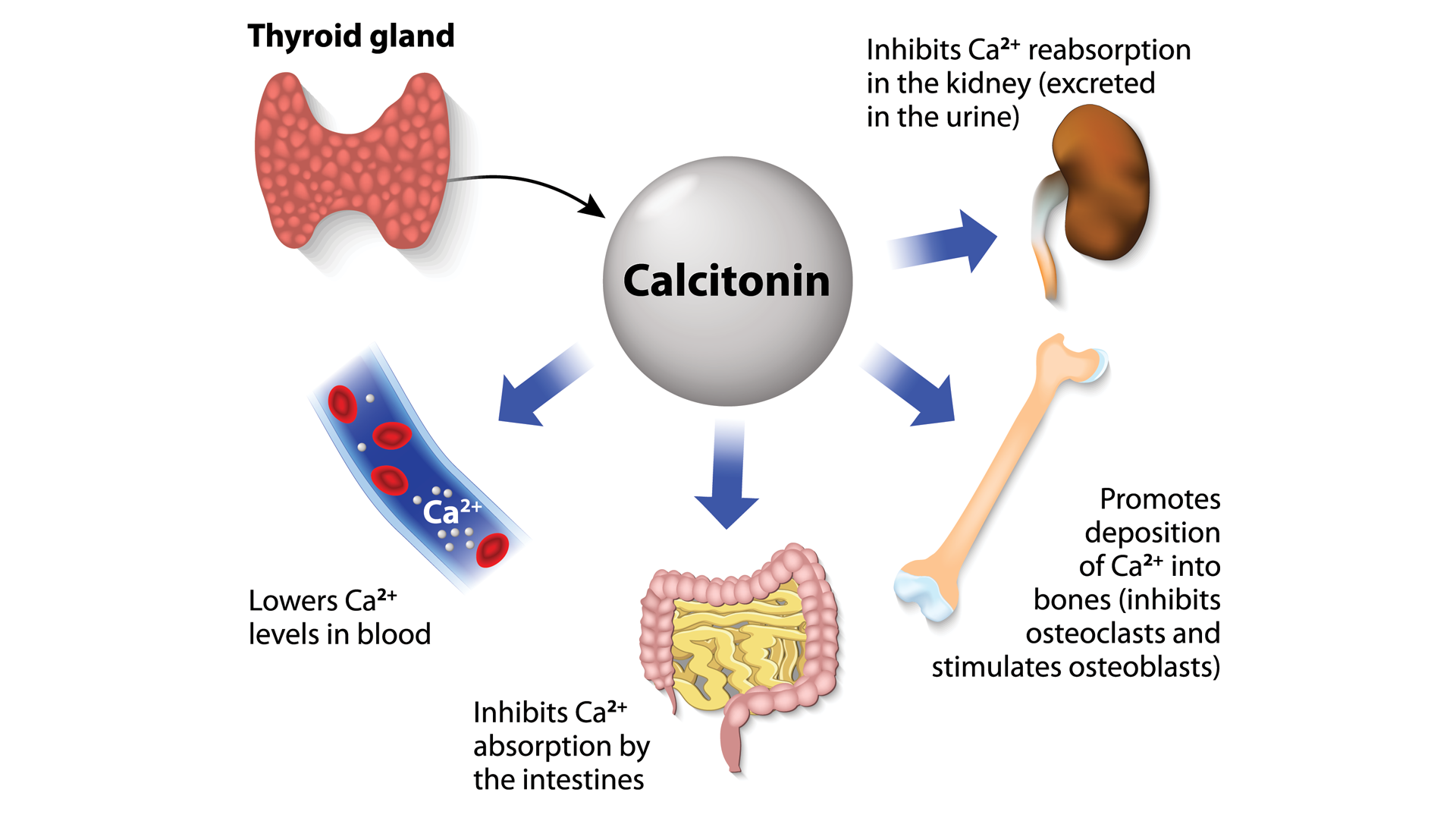
Per orders, Wayne administers 0.9% normal saline at 300 mL/hour, calcitonin 4 mg/kg I.V., and zoledronic acid 4mg I.V. Wayne administers ketorolac 15 mg I.V. push for pain control.
Outcome
 Six hours after receiving calcitonin, Mr. Tanner’s serum calcium level has improved to 10 mg/dL. His CT scans reveal multiple lytic lesions, which may indicate malignancy. Diagnostic tests reveal kappa light chain multiple myeloma. The patient is discharged 4 days later with a 1-week follow-up to begin chemotherapy.
Six hours after receiving calcitonin, Mr. Tanner’s serum calcium level has improved to 10 mg/dL. His CT scans reveal multiple lytic lesions, which may indicate malignancy. Diagnostic tests reveal kappa light chain multiple myeloma. The patient is discharged 4 days later with a 1-week follow-up to begin chemotherapy.
Education
Hypercalcemia can result from benign or malignant origins. Severe cases (>14 mg/dL) are considered a medical emergency and require treatment in an inpatient setting. If left untreated, hypercalcemia can damage multiple organ systems, leading to renal failure or cardiac arrest as well as long-term effects such as osteoporosis and bone pain. With multiple myeloma, hypercalcemia can result from the destruction of bone due to osteolytic lesions. Patients also can experience psychiatric disturbances such as lethargy, confusion, obtundation, or coma.
Hypercalcemia is generally reversible. Treatment includes I.V. normal saline (to increase urinary excretion of calcium), calcitonin (to prevent bone resorption), and bisphosphonates, such as zoledronic acid (the effects can last several weeks and are preferred for patients with malignancy-related hypercalcemia).
*Name is fictitious.
The authors are stem cell transplant nurse practitioners at the Department of Veterans Affairs Tennessee Valley Health Care in Nashville.
American Nurse Journal. 2025; 20(7). Doi: 10.51256/ANJ072536
References
Anastasopoulou C, Mewawalla P. Malignancy-related hypercalcemia. StatPearls. March 4, 2024: ncbi.nlm.nih.gov/books/NBK482423/
Dickens LT, Derman B, Alexander JT. Endocrine Society hypercalcemia of malignancy guidelines. JAMA Oncol. 2023;9(3):430-1. doi:10.1001/jamaoncol.2022.7941
Horwitz MJ. Hypercalcemia of malignancy: Mechanisms. UpToDate. May 2, 2024. uptodate.com/contents/hypercalcemia-of-malignancy-mechanisms?search=hypercalcemia%20of%20malignancy&source=search_result&selectedTitle=1%7E150&usage_type=default&display_rank=1
Khan AA, Gurnani PK, Peksa GD, Whittier WL, DeMott JM. Bisphosphonate versus bisphosphonate and calcitonin for the treatment of moderate to severe hypercalcemia of malignancy. Ann Pharmacother. 2021;55(3):277-85. doi:10.1177/1060028020957048
Key words: hypercalcemia, malignancy, multiple myeloma

















2 Comments. Leave new
Wonderful article! Thank You.
Thank you very much! We are glad you enjoyed it.