
Optimize referral to home-based primary care.
- Frailty screening with the Clinical Frailty Scale before hospital discharge provides an accurate and user-friendly mechanism to increase inpatient clinician identification of hospitalized patients at high risk for poor discharge outcomes.
- The intervention addresses barriers to routine referral to home-based primary care for hospitalized patients.
- Integrating the scale into nursing care serves as a strategy to promote recognition of frail adults and optimize access to home-based primary care.
An expanding body of literature demonstrates the ability of HBPC to provide high-quality care that reduces rates of hospitalization and emergency department use, while also improving patient quality of life and reducing caregiver burden. According to Zimbroff and colleagues, HBPC has demonstrated improved care coordination via use of interprofessional teams and intensive medication management. Overall, HBPC results in reduced costs to healthcare systems and the frail homebound population.
The nurse’s role in advance care planning
HBPC’s rapid acceptance coincides with a readjustment in the U.S. healthcare landscape following the COVID-19 pandemic when healthcare systems were incentivized to offer more services outside of the hospital. In addition, according to Zimbroff and colleagues, the push toward value-based payment models offers HBPC programs an opportunity to demonstrate superior care coordination compared to traditional fee-for-service models.
Despite its demonstrated success (as noted by Zimbroff and colleagues), access to HBPC remains limited. Of the almost 7 million estimated homebound individuals in the United States, only a fraction have access to HBPC. When Ornstein and colleagues examined the epidemiological trends of the completely homebound population, they found that only 12% reported having access to an HBPC program. These programs remain especially limited for rural populations.
Some of the medical literature (including Zimbroff and colleagues) demonstrates improved integration of mental health services and HBPC at Veterans Health Administration (VA) sites. However, our review found little evidence of other specialty care involvement with HBPC. The VA system has an established HBPC program going back decades, and much of the HBPC literature analyzes VA data; less is known about HBPC trends in other care settings.
Identifying an appropriate tool
The initial phase of this evidence-based project (EBP) focused on determining an appropriate measure to identify currently hospitalized patients eligible for HBPC. The practice site had an existing HBPC program, so the project director used referral as a measure of access.
Noting the disparity in referrals to HBPC from specialty care services, the project director selected an acute care cardiology unit as the practice setting for implementation. Communication with practice site stakeholders (the unit nurse manager, staff nurses, a unit-based nursing case manager, internal medical residents, physical and occupational therapists, nurse practitioners, attending cardiologists, and clinicians from cardiology and those in the outpatient setting working with older adults) revealed routine use of frailty screening via the Clinical Frailty Scale (CFS) as a proxy measure of HBPC eligibility; however, the inpatient setting lacked a formalized process for frailty recognition. The team hypothesized that education about the CFS and its use by inpatient clinicians could increase identification of frail patients who might benefit from an HBPC referral. (See Clinical frailty scale.)
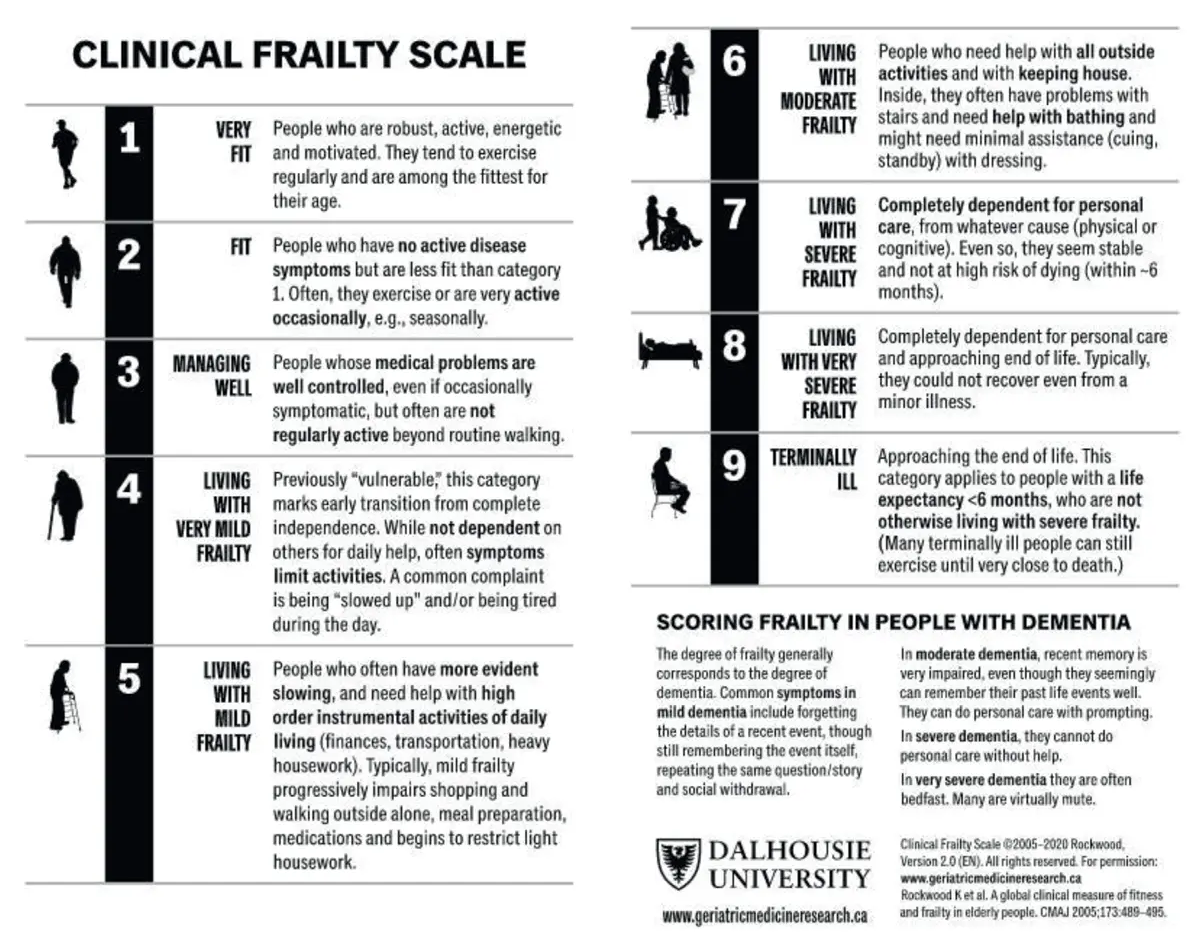
Clinical frailty scale
Rockwood and colleagues describe the clinical frailty scale (CFS) as a validated instrument widely used to identify older adults at risk for poor outcomes. The 9-point scale ranges from 1 (very fit) to 7 (severely frail) to 9 (terminally ill). CFS scores take into account patient factors, such as engagement in activities of daily living, number of chronic conditions, and ability to participate in activities outside of the home.
Source: Copyright permission obtained from Dalhousie University
Literature review
The project director conducted a systematic review of academic journal articles published in English between 2012 and 2022 to answer the clinical question: In an acute care population, what’s the utility and validity of the CFS in identifying patients at risk for poor discharge outcomes? The review (including of studies by Aucoin and colleagues, McLeod and colleagues, and others) concluded that frailty has high association with poor discharge outcomes, readmission after an acute care hospitalization, and increased mortality.
In addition, the review supports the CFS as an accurate and easy-to-use tool for identifying hospitalized patients at risk for poor discharge outcomes. The literature also supported use of the CFS as an early identification tool to customize interventions for effective discharge planning for frail adults.
Many of the poor discharge outcomes (such as increased healthcare use, length of stay, increased costs, decreased quality of life, and caregiver burden) strongly associated with moderately to severely frail CFS scores are the same outcomes positively impacted by access to an HBPC program. Thus, the prevailing academic literature supports use of the CFS in an acute care setting to improve care coordination and referral to trajectory-transforming discharge interventions like HBPC.
Methods
The project director followed The Johns Hopkins Nursing Evidence-Based Practice Model as a methodological framework to establish an environment of inquiry, recruit an interprofessional team (made up of the stakeholders), conduct a comprehensive review of the current evidence, and develop an action plan for implementation of the EBP project. (See What is EBP?)
What is EBP?
Melnyk and Fineout-Overholt define evidence-based practice (EBP) as a longitudinal problem-solving approach to clinical practice that integrates patient values, clinical expertise, critical appraisal, and synthesis of the best scientific evidence from a systematic search to guide care delivery. It aims to improve quality of care and patient outcomes by systematically applying current evidence to a complex clinical question. According to Dang and Dearholt, EBP encourages adoption of a practice, establishes a common language, creates standard processes, and helps to embed the practice within a unit or organization.
For this intervention, the project director selected the EBP approach to foster healthcare provider adoption of the CFS tool to ensure the interprofessional team (stakeholders) could speak a common language of frailty, standardize the process of discharge planning, and embed the practice of frailty identification into the fabric of acute care services at our academic medical center.
Intervention
The project director piloted the intervention on an acute medical cardiology unit of an academic teaching hospital in the mid-Atlantic region from October to November 2022. The director assessed existing organizational knowledge of frailty, identified clinical process gaps in discharge planning for high-risk patients, and elicited stakeholder buy-in for using the CFS.
The team then disseminated knowledge from the prevailing medical literature to unit nursing staff via brief in-person educational sessions, which occurred weekly over a 1-month period. During these sessions, the intervention nurse educator coached staff on the importance of using the CFS to identify frail hospitalized adults and provided handouts on how to score the CFS and make referrals to HBPC. (See Educational handouts.)
Educational Handouts
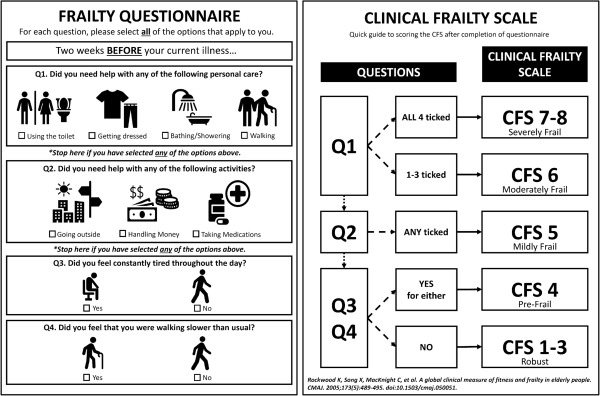
To aid adoption of the Clinical Frailty Scale (CFS), the project team offered educational handouts. One handout provides a step-by-step flow chart (previously validated by Chong and colleagues in a study of the CFS) for assigning a frailty score.
Source: Adapted from Chong et al
Another handout provides information about the existing home-based primary care (HBPC) program, answers frequently asked questions, and offers suggestions for making an HBPC referral.
After each educational session, staff nurses completed a CFS flowsheet in the electronic health record (EHR) for assigned patients during their current shift. The project director conducted a prospective chart audit to track completion of the CFS flowsheet and ensure inter-rater reliability in creating a CFS score. To confirm validity of the CFS screening, the intervention nurse educator (a geriatric nurse practitioner with clinical expertise in using the CFS score) reviewed each score for accuracy.
The chart audit enabled the nurse educator to track nursing adherence to screening completion and to review patients identified as moderately to severely frail with the unit-based nursing case manager and the medical care team during interprofessional discharge rounding. The audit allowed the intervention team to assess unit frailty knowledge in real-time and provide tailored coaching and feedback as the intervention evolved over the 4-week period.
To evaluate practice change and process outcomes, referrals from the intervention unit to HBPC were tracked prospectively during the intervention period and 1 month after the intervention (a total of 8 weeks). The project team compared referral volume during the intervention period to referral volume from the previous year (October to November 2021).
Outcomes
During the intervention, unit nurses screened 79 of 93 hospitalized patients using the CFS flowsheet in the EHR. This translated to a nurse screening adherence rate of 85%. Of the 79 screened patients, 32 (approximately 40%) had a CFS score of 6 or higher (moderately to severely frail). Because the CFS defines moderate frailty as requiring help with all outside activities, these 32 patients were categorized as homebound. However, not all met the inclusion criteria for HBPC referral—ten patients didn’t live within the HBPC catchment area, one was receiving dialysis, and two were scheduled for discharge to skilled nursing facilities.
During the study period, the unit identified 19 patients (approximately 24%) as meeting inclusion criteria for referral to HBPC and discussed them as potential referrals with the nursing case manager. The previous year, the unit made no HBPC referrals (See Chart audits and referral outcomes).
Patient-related factors contributing to HBPC referral omission included acute psychiatric needs, unstable housing/caregiving, or patient declining referral to the program.
Chart audits and referral outcomes
Weekly chart audits identified the number of patients eligible for Clinical Frailty Scale screenings, the number who received screening, the number identified as homebound, and the number who met home-based primary care referral criteria. The fourth column shows the average frailty score per week.
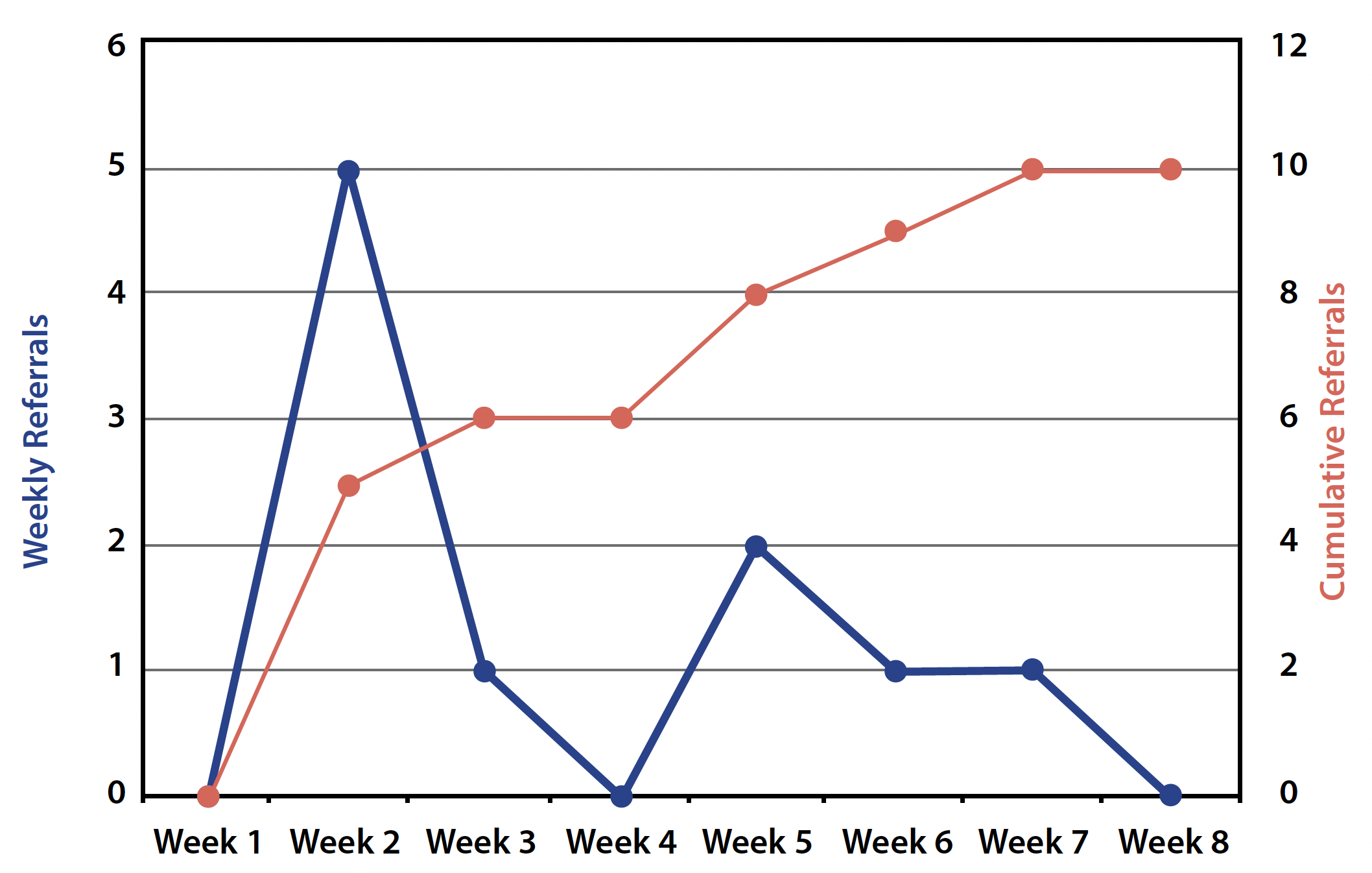
Referral outcomes
The following chart shows referrals by week (blue) vs referrals over time/cumulative (orange).
Discussion
This EBP intervention demonstrated success in building linkages and improving care coordination between inpatient clinicians and HBPC. Referrals increased significantly during the intervention period. Among patients hospitalized on the unit during the study period, nearly 85% received a frailty screening assessment, a remarkable accomplishment considering the existing time and staffing constraints. Despite multiple weeks of frequent staff absences due to illness and critically low staffing periods, nurses remained motivated and engaged with completing the screening and communicating with the project team about their evolving knowledge acquisition.
Staff frequently expressed that completing the screening provided them with an advocacy tool and a discharge resource (HBPC) that they previously didn’t know about. Before the intervention, inpatient clinicians expressed despair when caring for patients with significant discharge needs who frequently required readmission. Empowered with the knowledge that HBPC can help reduce avoidable hospital use among older adults with complex medical conditions, nursing staff anecdotally expressed increased job satisfaction with the knowledge that they could objectively identify frail patients and offer them an evidenced-based intervention.
Identification of 40% of patients as moderately to severely frail via screening suggests that the project accessed a population likely to benefit from frailty screening. In addition, 24% met initial screening criteria for referral to HBPC, demonstrating the intervention’s ability to reveal a previously unidentified population most likely to benefit from HBPC services. Of the 10 referrals placed to HBPC, eight were placed by the nursing case manager, one by a nurse practitioner, and one by a heart failure navigator nurse. This finding suggested the importance of recruiting specialized nursing roles in the intervention.
Unexpected benefits
Designing the educational handouts for this intervention led to improvements to the HBPC program website and referral process. These included the creation of a referral link on the website, easily accessible to all interested healthcare providers, family members, caregivers, and community members. In attempting to streamline the inpatient workflow for discharging frail hospitalized patients, the outpatient referral process became democratized, allowing greater access to HBPC from a wider pool of applicants, now all neatly organized into one referral link (as opposed to varying email addresses and word of mouth).
Limitations
Unit staffing appears to have played a significant role in limiting the nursing staff’s ability to place referrals. The nurse manager defined the last 2 weeks of the study period as critical staffing days, which correlated with a significant drop in referrals from the unit staff. However, this decline in referral volume also correlates to an overall drop in the average frailty score on the unit each week. The proportion of homebound/moderately to severely frail patients decreased from 46% in Week 1 to 29% in Week 4, which suggests a smaller pool of HBPC-eligible patients. This trend indicates that the intervention may not be applicable to acute care populations with a lower incidence of moderate-to-severe frailty.
An unexpected obstacle was the misconception that only physician providers had the authority to place an HBPC referral. The project team made several attempts to counter this misunderstanding, including coaching with each primary nurse to provide examples of referrals previously placed by family members, social workers, caregivers, and others. Unfortunately, no primary RNs made referrals during the intervention period. Further work is needed to explore this lack of agency felt among primary RNs to play a more active role in discharge planning for their assigned patients.
Sustaining frailty recognition
This EBP project fostered healthcare provider adoption of the CFS tool and enabled the nursing staff to speak a common language about frailty. Further work will help standardize the process of discharge planning and embed the practice of frailty identification into the fabric of acute care services at this medical center.
Expanding the intervention for replication across additional acute care units (at the practice site or elsewhere) offers a vital next step to continuing inpatient clinician recognition of frail patients in need of HBPC. Including the CFS as a required part of an admission database for every patient also would serve as a valuable next step in ensuring sustainability of frailty recognition among hospitalized patients.
Caitlin Burchfield is an assistant professor and nurse practitioner at the University of Virginia School of Nursing in Charlottesville. Halima Walker is a nurse manager at UVA Health in Charlottesville, Virginia. Regina DeGennaro is a professor at the University of Virginia School of Nursing. Justin Mutter is an associate professor and section head in geriatrics at the University of Virginia School of Medicine in Charlottesville. Sarah Craig is an associate professor at the University of Virginia School of Nursing.
American Nurse Journal. 2026; 21(1). Doi: 10.51256/ANJ012650
References
Aucoin SD, Hao M, Sohi R, et al. Accuracy and feasibility of clinically applied frailty instruments before surgery: A systematic review and meta-analysis. Anesthesiology. 2020;133(1):78-95. doi:10.1097/ALN.0000000000003257
Chong E, Tham A, Chew J, et al. Brief aids to guide clinical frailty scale scoring at the front door of acute hospitals. J Am Med Dir Assoc. 2021;22(5):1116-7.e2. doi:10.1016/j.jamda.2021.02.005
Curtis E, Romanowski K, Sen S, Hill A, Cocanour C. Frailty score on admission predicts mortality and discharge disposition in elderly trauma patients over the age of 65 y. J Surg Res. 2018;230:13-9. doi:10.1016/j.jss.2018.04.017
Dang D, Dearholt SL. Johns Hopkins Nursing Evidence-Based Practice: Model and Guidelines. 3rd ed. Indianapolis, IN: Sigma Theta Tau International; 2017.
Hominick K, McLeod V, Rockwood K. Characteristics of older adults admitted to hospital versus those discharged home, in emergency department patients referred to internal medicine. Can Geriatr J. 2016;19(1):9-14. doi:10.5770/cgj.19.195
Juma S, Taabazuing MM, Montero-Odasso M. Clinical frailty scale in an acute medicine unit: A simple tool that predicts length of stay. Can Geriatr J. 2016;19(2):34-9. doi:10.5770/cgj.19.196
Kanenawa K, Isotani A, Yamaji K, et al. The impact of frailty according to Clinical Frailty Scale on clinical outcome in patients with heart failure. ESC Heart Fail. 2021;8(2):1552-61. doi:10.1002/ehf2.13254
Lewis ET, Dent E, Alkhouri H, et al. Which frailty scale for patients admitted via emergency department? A cohort study. Arch Gerontol Geriatr. 2019;80:104-14. doi:10.1016/j.archger.2018.11.002
Mazzola P, Buttò V, Elli S, et al. Frailty predicts failure to discharge patients home from a subacute-care unit: A 3-year Italian experience. Aging Clin Exp Res. 2022;34(1):95-103. doi:10.1007/s40520-021-01908-w
Melnyk BM, Fineout-Overholt E, eds. Evidence-Based Practice in Nursing & Healthcare: A Guide to Best Practice. Fourth edition. Wolters Kluwer; 2019.
Ornstein KA, Leff B, Covinsky KE, et al. Epidemiology of the homebound population in the United States. JAMA Intern Med. 2015;175(7):1180-6. doi:10.1001/jamainternmed.2015.1849
Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489-95. doi:10.1503/cmaj.050051
Rockwood K, Theou O. Using the Clinical Frailty Scale in allocating scarce health care resources. Can Geriatr J. 2020;23(3):210-5. doi:10.5770/cgj.23.463
Tew YY, Chan JH, Keeling P, et al. Predicting readmission and death after hospital discharge: A comparison of conventional frailty measurement with an electronic health record-based score. Age Ageing. 2021;50(5):1641-8. doi:10.1093/ageing/afab043
Wharton C, King E, MacDuff A. Frailty is associated with adverse outcome from in-hospital cardiopulmonary resuscitation. Resuscitation. 2019;143:208-11. doi:10.1016/j.resuscitation.2019.07.021
Zimbroff RM, Ornstein KA, Sheehan OC. Home-based primary care: A systematic review of the literature, 2010-2020. J Am Geriatr Soc. 2021;69(10):2963-72. doi:10.1111/jgs.17365
Key words: frailty, home-based primary care, nurse-driven evidence-based practice


















