
This NICU established a process that improved patient outcomes and triggered a positive culture change.
- This nursing morbidity and mortality conference empowers nurses to expand their knowledge base, improve collaboration, and heightened the quality of care.
- The conferences allow nurses to address concerns even if tangible processes aren’t created as a result.
- They promote shared decision-making, empowering nurses to address patient care concerns, enhance nursing practice, foster teamwork, and grow professionally.
PDSA cycle
THE IMPLEMENTATION of nursing-led morbidity and mortality conferences (NMMCs) in our neonatal intensive care unit (NICU) emerged after experiencing several adverse patient outcomes and identifying nursing knowledge gaps related to certain diagnoses. With the goal of improving the quality of nursing care and providing educational opportunities for nurses, we established a committee (including nursing representatives from the unit-based council) to begin reviewing the literature to support the creation of NMMCs.
Although little evidence related to NMMCs exists, available research, such as from Ropp, encourages creating a template to structure morbidity and mortality (M&M) conferences and includes all stakeholders in the discussion. Other evidence, such as from the Department of Veterans Affairs, as discussed by Veazie and colleagues, describes implementing high-reliability organization principles and developing clinical policies driven by evidence to address gaps in knowledge and executing clinical practice guidelines and performance measures.
Based on this information and following the Plan-Do-Study-Act framework (PDSA), we developed a format for ongoing NMMCs, including an agenda focused on nursing-centric processes and care systems. (See PDSA cycle.)
PDSA cycle
In establishing the nursing-led morbidity and mortality conferences, the project team follows the Plan, Do, Study, Act format.
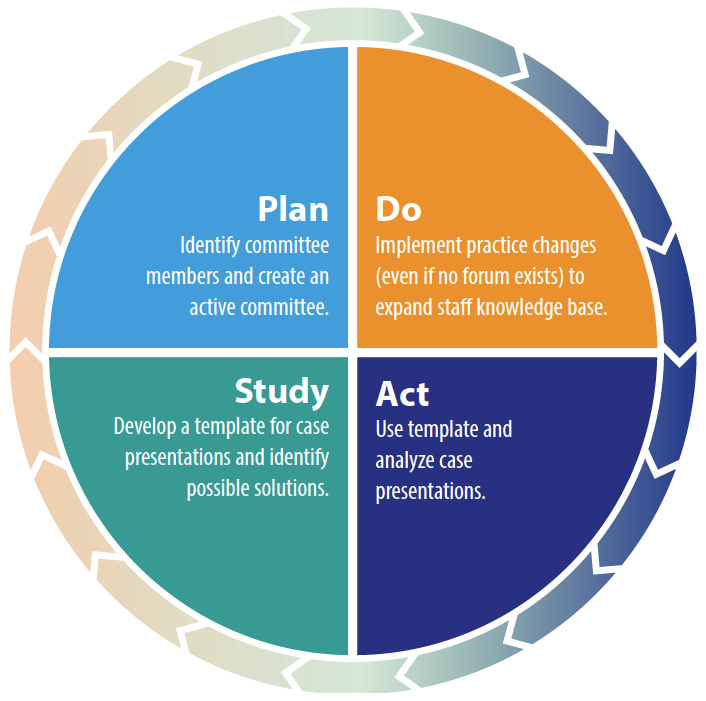
Plan
A member of the NMMC committee attended physician-led M&M conferences to gain a better understanding of their structures and processes. The committee met monthly to review the literature, organize a conference structure, and identify presenter, facilitator, recorder, and timekeeper roles.
After developing a method for case presentation, the committee asked a newer RN and an experienced RN who served as an NMMC committee member to present a case. Partnering with newer nurses improved staff participation and empowered nurses to broach questions related to nursing care.
The committee presented outcomes of these meetings to the nursing NICU staff after practicing with four cases and PDSA cycles.
Do
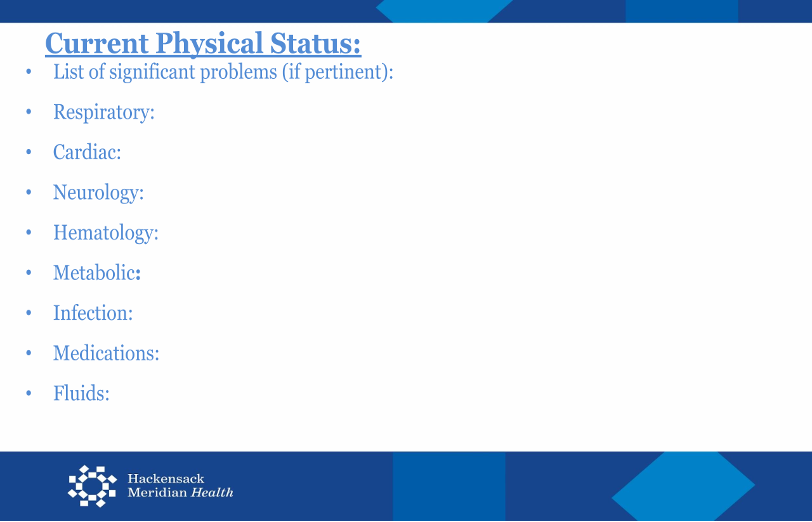
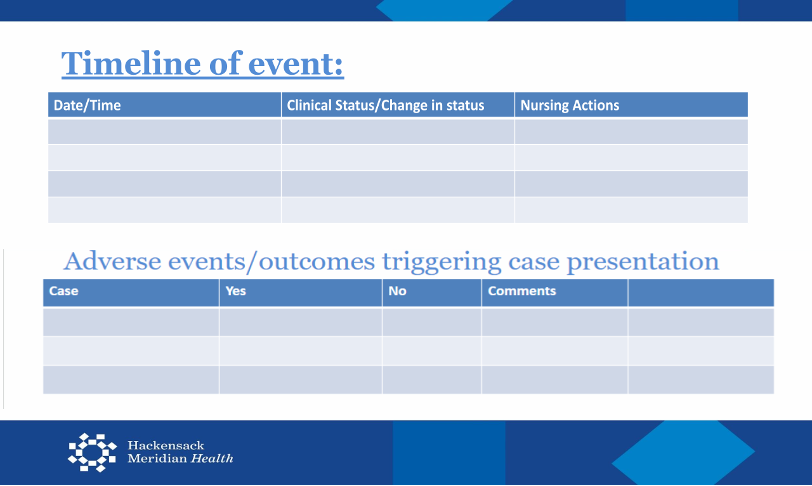
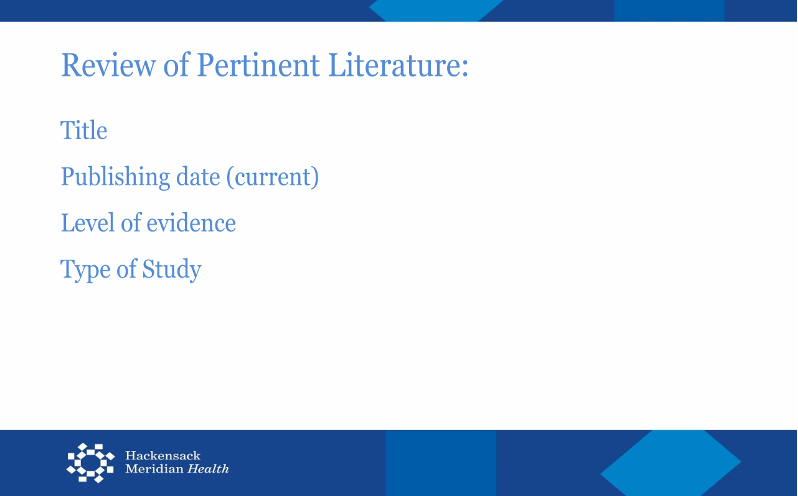
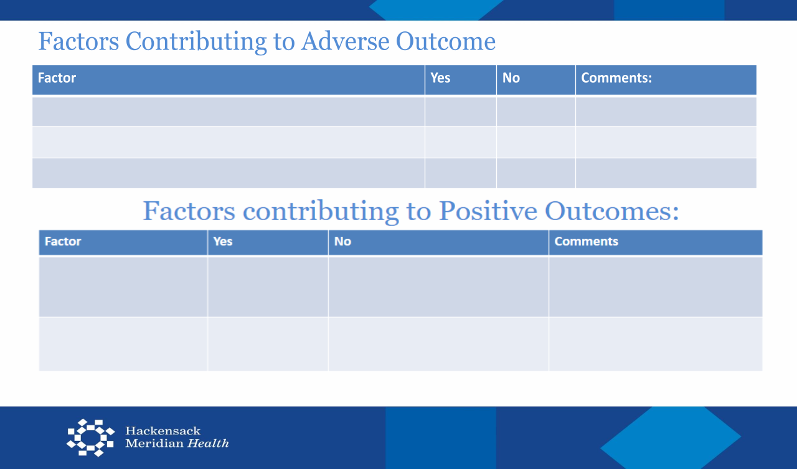
While presenting cases in monthly meetings, the NMMC committee identified the need to provide case-specific education to the nursing staff. The committee developed templates for case presentations based on modified fishbone diagrams, which divided the presentation into categories for adverse outcomes and proposed solutions. (See Case presentation templates)

Study
The committee presented four cases (including three trial cases). The first three cases were complex nursing cases; the fourth involved a multidisciplinary approach and provided a learning opportunity for everyone based on the nurses’ findings. The first case addressed a very low birth weight (premature) neonate and hyperkalemia that required treatment with insulin and albuterol. Discussion of this case identified the need for education in using the online medication data and safety tool. In collaboration with the respiratory team, the unit established an alternative for administering nebulizers via high-frequency ventilators.
The second case involved the care of an infant born with epidermolysis bullosa. From this presentation, a pain management committee was formed to address dressing changes for patients with this condition, and bimonthly nurse–physician meetings were initiated to improve staff communication.
The third case focused on a patient brought to the operating room (OR) for repair of a tracheoesophageal fistula. Case discussion revealed a knowledge gap with regard to preoperative nothing-by-mouth status and inappropriate administration of sucrose or colostrum. This presentation also led to the creation of in-house OR transport kits.
The fourth case described a morphine drip dosing error. While the infant was body cooling and receiving respiratory support, their pain was inadequately controlled despite administration of continuous morphine. Two direct care nurses verified and initiated the medication order; however, the advanced practice RN and neonatologist wanted to see the written dose increase. This discussion resulted in addressing the identification of correct morphine orders for body cooling with all healthcare providers. This case led to a review of chain of command and a reminder to use the online resource tool for administering and dosing medication.
Key takeaways from these case reviews included a knowledge gap in medication dosing and pain management. A pain management group of RNs and MDs formed to review pain protocols in the unit and educate staff of any changes. The unit recognized that errors can happen to anyone, and open dialogue encouraged comprehensive discussion and collaboration.
Act
Charge nurses, unit-based council members, and nursing leadership encourage staff to recommend quality improvement opportunities to the NMMC committee, who then vote together on which cases to present. After the committee agree on a case, two to three NMMC committee members conduct an extensive chart review to identify potential gaps in knowledge or care. Next, those members present the chosen case to the rest of the committee. The following month, the NMMC committee presents its findings to the unit-based committee and disseminates a written summary to staff members unable to attend.
Challenges and solutions
The committee encountered several challenges in their efforts to establish NMMCs, including lack of peer-reviewed literature and research. However, they ultimately created a user-friendly case presentation algorithm unique to the NICU. The algorithm guides the root cause analysis discussion. (See Getting to the root cause.)
Getting to the root cause
The nursing-led morbidity and mortality conferences use an algorithm to guide root cause analysis. It considers the people, procedures, equipment, environments, and policies involved.
- Staffing issues, burnout, communication among disciplines
- Patient name alerts
- Family and social issues
- Opportunities for staff education in knowledge or best practices related to a particular diagnosis, medication, or treatment
- Lack of knowledge surrounding use
- Malfunctioning equipment
- Supply shortages
- Transitions of care
- Leaving the floor for a procedure or imaging
- Temperature issues on the unit
- Hospital or network policies
- Nursing best practice guidelines
- Bedside references
- Documentation
- Electronic charting system downtime
- Issues in other departments (lab, pharmacy)
Other challenges, many of which impacted establishing consistent meeting times, included staffing concerns related to increased census and acuity, effective processes for communicating important education and information based on conference outcomes, and conflicts with other unit-based quality improvement projects already in process.
Despite these challenges, the committee identified several opportunities for growth that impact day-to-day nursing practice. For example, two RNs now confirm morphine dosing of all patients receiving body cooling against the online resource tool for medications. This best practice has become a standard in the unit. In addition, the NMMCs have provided a platform for nurses to voice concerns and develop productive strategies for addressing and correcting them. Each team member’s commitment to this project’s purpose and success may help to ensure its expansion throughout the network of affiliated hospitals.
Nursing implications
The unit’s goals for initiating NMMCs included fostering a stronger partnership among all NICU multidisciplinary staff. The committee aimed to inspire a workplace where efforts to improve patient outcomes would become an innate part of the unit culture. Before this initiative, nurses on the unit frequently hesitated to call out concerns. The committee strived to take finger-pointing out of the equation, which increased reporting of events and good catches.
The success of this project extended beyond mere improvement of clinical practice to include demonstrative culture changes from a multidisciplinary approach. For example, observation, general discussion at unit-based committee meetings, and nurse engagement after presentations indicate more open communication and positive feedback during nurse hand-off. In addition, the pediatric pharmacy department has applauded the NICU for identifying good catches as well as potential medication errors. Other units that adopt this approach might experience culture improvements, which they could measure by reviewing risk management incident reports. (See Transform unit culture)
Transforming unit culture
To strengthen partnerships across the NICU multidisciplinary team and share the responsibility of patient safety, we focused on these key impacts:
- Shifting culture from blame to collaboration
- Increasing nurse confidence in reporting concerns and good catches
- Enhancing communication during hand-offs
- Recognizing the pediatric pharmacy department for catching potential medication errors
Ultimately, the project achieved the following outcomes:
- Measurable improvements in unit culture
- More transparent, proactive approaches to patient safety
- A model for other units to adopt, with trackable progress via risk management reports
Champions of safe care
The development of NMMCs empowers these NICU nurses to expand their knowledge base, improve collaboration, and enhance care quality. It inspires nurses to encourage one another to evaluate the care provided to their patients, and it gives them the voice to recognize where gaps in care could serve as opportunities for growth rather than blame, criticism, or penalty.
These NMMCs embrace shared decision-making by providing opportunities for participation in developing and implementing new evidence-based practice. In addition, they foster teamwork, interdisciplinary communication and collaboration, and professional development. Together, healthcare providers can build from their imperfections, harness individual and collective strengths, and become champions for a safer healthcare system.
Joanne Pasinski is a NICU research quality specialist at Hackensack University Medical Center in Hackensack, New Jersey. Bianca Taurozzi is a nurse at Hackensack Meridian Health. Naomi Hanoch is a nurse at Hackensack University Medical Center. Jessica Villarreal is a NICU nurse at Hackensack University Medical Center. Krystyna Toczylowski is a clinical nurse specialist at Hackensack Meridian Health. Marissa Rodriguez is a nurse at Hackensack University Medical Center. Katharine LaCoppola is a nurse at Hackensack Meridian Health. Kelly Gillan is a nurse at Hackensack University Medical Center. Cassandra Martin-Walters is a NICU nurse manager at Hackensack University Medical Center.
American Nurse Journal. 2025; 20(11). Doi: 10.51256/ANJ112514
References
Brunson A, Hooten P, Furst C, Chen W. Driving to zero harm with nursing morbidity and mortality conferences. Am Nurse Today. 2019. myamericannurse.com/wp-content/uploads/2019/09/ant9-Magnet-Stories-ZeroHarm.pdf
Collins E, Owen P, Digan J, Dunn F. Applying transformational leadership in nursing practice. Nurs Stand. 2020;35(5):59-66. doi:10.7748/ns.2019.e11408
Dracup K, Bryan-Brown CW. Nursing morbidity and mortality conferences. Am J Crit Care. 2003;12(6):492-4. doi:10.4037/ajcc2003.12.6.492
Guger C, Daum S, Vacek L, et al. Nursing morbidity and mortality conferences: a tool for enhancing quality patient care. J Nurses Staff Dev. 2011;27(1):35-8. doi:10.1097/NND.0b013e3182061d66
Hiner J, White S, Fields W. Infusing evidence-based practice into interdisciplinary perinatal morbidity and mortality conferences. J Perinat Neonatal Nurs. 2009;23(3):251-7. doi:10.1097/JPN.0b013e3181af6ebb
Institute of Medicine (US) Committee on Quality of HealthCare in America. In: Kohn LT, Corrigan JT, and Donaldson MS eds. To Err Is Human: Building a Safer Health System. National Academies Press (US). 2000.
Pagano LA, Lookinland S. Nursing morbidity and mortality conferences: Promoting clinical excellence. Am J Crit Care. 2006;15(1):78-85. doi:10.4037/ajcc2006.15.1.78
Ropp PW. Establishing a nursing morbidity and mortality conference. Nursing. 2011;41(4):18-9. doi:10.1097/01.NURSE.0000395303.76162.eb
Van Baarle E, Hartman L, Rooijakkers S, et al. Fostering a just culture in healthcare organizations: experiences in practice. BMC Health Serv Res. 2022;22(1):1035. doi:10.1186/s12913-022-08418-z
Veazie S, Peterson K, Bourne D. Evidence Brief: Implementation of high reliability organization principles. Washington (DC): Department of Veterans Affairs (US); 2019. ncbi.nlm.nih.gov/books/NBK542883
Walker M, Rubio D, Horstman M, Trautner B, Stewart D. Stop the blame game: Restructuring morbidity and mortality conferences to teach patient safety and quality improvement to residents. MedEdPORTAL. 2016;12:10475. doi:10.15766/mep_2374-8265.10475
Zavotsky KE, Ciccarelli M, Pontieri-Lewis V, Royal S, Russer E. Nursing morbidity and mortality: the clinical nurse specialist role in improving patient outcomes. Clin Nurse Spec. 2016;30(3):167-71. doi:10.1097/NUR.0000000000000205
Key words: nursing morbidity and mortality conference, shared decision-making, collaboration



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}