Staffing, AI, bullying, and DEI have nurses talking.
- More than 1,000 nurses participated in the 2025–2026 nursing trends survey.
- Difficulty in staff turnover and nurse recruitment increased from the previous survey.
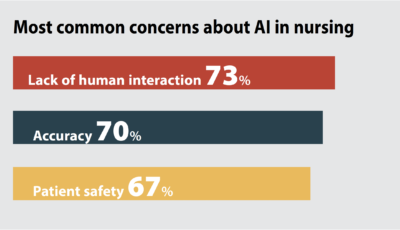
- The most common concern about AI is lack of human connection.
- When asked if they would still choose a nursing career, 81% said yes.
Editor’s note: If you were one of the more than 1,000 nurses who took the American Nurse Journal’s ninth annual Trends Survey, you already know that it was significantly shorter and introduced new topics, including artificial intelligence (AI) and misinformation. It still asked nurse managers (258) and clinical nurses (593) about staffing, recruitment, turnover and job satisfaction. It did not, however, include salary-related questions as it had in years past.
Instead, you’ll see a separate report here on nursing salaries as compiled by the U.S. Bureau of Labor Statistics, which should provide a more comprehensive view of nurse pay throughout the country.
The Trends Survey, conducted between November 4, 2025 and February 16, 2026, was shortened by reducing the number of questions in some areas while introducing new topics, such as artificial intelligence (AI) in nursing; how you handle misinformation with patients; and whether the healthcare workplace experienced any significant changes to diversity, equity, and inclusion (DEI) programs.
These changes aim to address new, timely issues without increasing the amount of time required to complete the survey.
We hope you find the results as enlightening as we did.
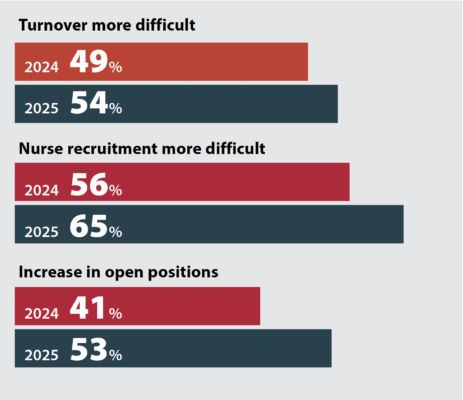
STAFFING STRUGGLES CONTINUE
Turnover, recruitment, and staffing all became more difficult in the last year, nurse managers reported.
We also saw the struggle to find and retain nurses reflected elsewhere in the survey. When managers and clinicians were asked to name the most important issues affecting nursing, many cited burnout, retention, recruitment, the loss of experienced nurses, and the resulting concern for adequate staffing levels.
“Retention of nurses at the same workplace to build experienced and seasoned nurses at that workplace—this is for safety and proper functioning of the workplace,” one respondent said about the issues facing nursing.
“The push to get new grads/nurses onto the floor/clinic ASAP whether they are appropriately trained,” said another.
Clinical nurse responses reflected an increased concern with safe staffing levels when they were asked, “Do you believe that staffing assignments are appropriate to meet patient needs at least 80% of the time?” Fewer than half (46%) said the statement was true—a 13 percentage point drop from the previous survey.
Despite concerns with staffing and other issues, job satisfaction remains relatively high. Most nurse managers (67%) and clinical nurses (66%) report they’re either very or somewhat satisfied with their jobs, down slightly from 70% and 74%, respectively, in 2024. However, this year slightly more nurses (26% vs. 22%) said they plan on looking for a job within 6 months.
What are nurses thinking about?
Similar to past surveys, when asked to name one or two important issues facing the nursing profession, struggles surrounding staffing rose to the top. But respondents also mentioned education and training for young nurses, the federal government’s proposal to not include nursing as a profession for student-loan purposes, AI in healthcare, and bullying/violence in the workplace. Here are some examples:
- Accountability to provide the basic, hands-on care to patients, from oral care and bathing to ambulation and patient teaching to prevent readmission. I also think we need to re-evaluate 12-hour shifts. Having worked both, there is less comradery, teamwork and more errors and worsening patient outcomes with 12-hour shifts.
- Keeping nurses in the hospital setting. Mentor nurses at all levels, even the DNP nurses, in the hospital setting. Having DNP and PhD nurses work together in the hospital setting, but leadership does not see the value of this and what it can do for nursing.
- Reversing the department of education’s decision to downgrade nursing as a profession and therefore make advanced degree loans more expensive and potentially reducing the numbers of nurses able to take on advanced degrees [and] limiting the numbers of APRNs and DNPs for rural healthcare access and nursing faculty to educate nursing students.
- Key issues include workplace bullying and the rising demand for specialized nursing care.
- Be able to spend time to interact with patients to know of their illnesses, physical and mental situations
- Increased use of ChatGPT by nurses/nursing students, who “brain dump” to sound intelligent, but can’t put together a cogent discussion verbally.
- Keeping up with the most recent/current health and science information and maintaining an open mind to all changes related.
- Lack of research in some areas, especially new and emergent technologies.
- Misinformation to the public from propaganda.
- Nursing shortages in both hospital and academic settings. The U.S. government not acknowledging nurses as a profession such as doctors, lawyers, etc.
- How to avoid errors, ensure medication safety, prevent complications, and provide standardized and effective care. How to achieve empathy, respect, and effective communication in a busy environment to reduce misunderstandings, conflicts, and complaints
- Nurses need to be better prepared to work bedside. It is an issue since COVID and changes in education.
- Elevating the profession and ensuring we are leaders in the c-suite making decisions that impact nursing. Non-nurses should not make decisions impacting nursing or manage nurses.
Nurses also had a few things to say about healthcare misinformation.
Battling misinformation
Over 500 nurses shared suggestions—primarily focused on listening and education—for how to handle misinformation during patient encounters. One nurse leader said, “I train my team to avoid arguing with patients and instead use open-ended questions to help patients reflect on misinformation and its potential to impact on their care.” Another said, “I listen to my patients carefully and use simple, evidence-based facts to gently correct health misinformation.”
Misinformation: Education and empathy
When asked “How do you address health misinformation with your patients?” more than 500 responded, many citing the importance of educating patients with evidence-based information while listening with patience and empathy. Here are some examples:
- I listen to my patients carefully and use simple, evidence-based facts to gently correct health misinformation.
- As a nurse manager, I lead my team to first listen to patients’ concerns, then share evidence-based information from trusted medical sources to clarify misinformation gently and consistently.
- I organize workshops for my nursing staff to teach patients basic health information evaluation skills—such as verifying sources and identifying evidence-based claims—to empower them to avoid misinformation long-term.
- I attempt to re-educate patients but it’s often ineffective.
- Patient Health Educator position dedicated to address information/working along with public affairs and medical media.
- Do what I can with the time that I have without making them mad.
- I focus on building trust, correcting misconceptions gently, and encouraging patients to ask questions so they feel comfortable making informed decisions
AI: PROMISE AND PERIL
AI has already entered the healthcare workplace, and it’s been greeted with the same mix of hope and fear that it faces in society at large.
Most survey respondents (76%) said AI will be or might be helpful in healthcare. However, their views varied: 19% believed it would be very helpful, 38% felt it might be helpful but had concerns about issues such as patient safety, and 19% said AI shouldn’t be used in patient care at all.
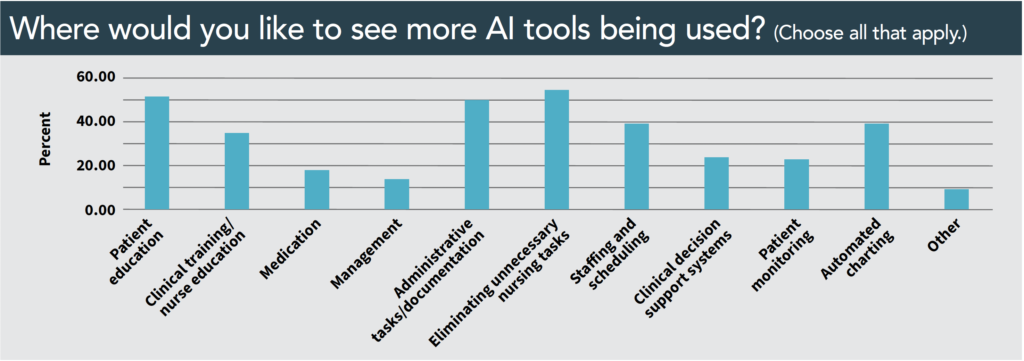
When asked to identify areas where they would like to see more use of AI tools, the top three responses were nearly equal: patient education (50%), administrative tasks/documentation (50%), and eliminating unnecessary nursing tasks (54%). Slightly fewer respondents said they thought AI could be helpful with automated charting (39%), staffing/scheduling (39%), and clinical training/nurse education (34%).
When asked to expand on their views, more than 150 respondents offered detailed explanations of their concerns and hopes for AI in healthcare.
“It’s coming, whether we like it or not,” said one. “We have an ethical obligation to ensure that nursing is actively involved in development and implementation of AI incorporation as it affects patients and nursing care.”
Most saw the potential positives and negatives.
“I see AI as having strong potential to support nursing—especially in triage, documentation, and decision support—but patient safety, data privacy, bias, and overreliance on algorithms must be carefully addressed before widespread use in direct patient care,” noted one respondent.
For others, the use of AI isn’t theoretical, allowing them to provide real-world examples of its impact.
“It may have a place but must be used carefully. I have encountered AI-generated patient summaries that are not at all reflective of the patient condition or presentation,” one wrote. “It scripted normal assessments that were not even completed. This could impact patient referrals, treatment, and payment from insurance companies.”
Beyond patient care, several respondents voiced concern about the impact on nursing education.
“I am worried that today’s students will rely on AI and not develop critical thinking and clinical judgement skills if they can just ask AI,” said one respondent. However, another noted the benefit it can have for instructors: “I use it nearly every day in teaching and developing curriculums.”
Many nurses, when asked to specify their hesitancy with AI, cited privacy concerns and accountability when an algorithm gets it wrong.
“AI can support nursing, but concerns about reliable outputs, patient safety, preserving human-centered care, protecting sensitive data, and ensuring adequate staff training must be addressed for safe integration,” said one.
Despite rveservations, many respondents said they would like to see AI used more for charting, space and equipment planning, and tracking clinical guidelines.
“Adding AI to an EHR *could* add value but will certainly add cost” said one nurse, noting their frustration with existing EHR systems. “I am constantly dismayed by [EHR’s] inability to do value added computing (such as warn me if I’m about to exceed an acetaminophen 3g/24 hours limit).”
Although many nurses were open to the potential of AI, a vocal group of respondents disagreed.
“AI does not belong in nursing,” said one, reflecting several others’ comments.
AI: Pros and cons
Respondents had a wide variety of views on the use of artificial intelligence (AI) in nursing. Here are some of their concerns, hopes, and recommendations:
- We’ve already started using AI for care plans and it puts more work and charting on the floor RN.
- It can be very helpful in the right application
- Concerned with academic dishonesty and the temptation for students to take shortcuts.
- Must use caution. AI is still learning and the ultimate responsibility for documentation lies on the human. AI requires excellent editing skills.
- I absolutely love it!
- Nurses not learning how to interact with real people, relying on AI/equipment versus learning actual needed skills.
- I think AI could be a great partner with nursing—50/50 relationship.
BULLYING AND VIOLENCE IN THE WORKPLACE
Workplace violence remains a major issue in healthcare workplaces. More than half (56%) of respondents had witnessed or experienced bullying in the past year, and 40% had witnessed other forms of workplace violence in that same time frame.
When asked for suggestions on how to reduce bullying and violence in their workplaces, more than 500 respondents offered their suggestions or their frustration.
Many noted the need for zero-tolerance, with comments like this: “Implement a zero-tolerance policy for all forms of violence and bullying, with clear consequences for perpetrators.” Several called for more security. For example, one respondent said, “Increase the number of security personnel on duty, especially during peak hours and in high-stress units.”
Many survey respondents noted that adequate staffing levels also can serve to discourage and control inappropriate behavior. Others called for additional education on bullying and training on how to de-escalate potentially violent situations.
Several people said their workplace already offers education and training and have zero-tolerance policies, although their views on the effectiveness of those measures varied.
“Take it seriously and hold staff accountable. On a positive note, it’s gotten better over the years,” said one. “In [long-term care], I deal with all levels of cognitive impairment, so I have to anticipate behavior and try to prevent it. When in acute care, it tends to depend on the patient, but again I had to anticipate it/try to prevent it.”
Bullying: What can be done?
When asked “What can be done to reduce bullying or workplace violence in your workplace?” more than 500 survey participants responded, many highlighting the need for zero-tolerance policies and better nursing and security staffing. Here are some of their other suggestions:
- Create a confidential reporting system that protects staff from retaliation when they report incidents.
- Provide regular de-escalation and self-defense training for all clinical staff to handle aggressive situations safely.
- Encourage increased reporting of incidents and publishing follow up/outcome to each incident within privacy guidelines.
- Talk about incivility in meetings. Give examples. Address it directly with those displaying those behaviors.
- Hold our patients more accountable for their actions. We attribute behaviors to their disease way too often and I feel they use it as an excuse.
- Treat everyone with respect and as human beings.
- [Consider that] …. in some instances we perceive bullying when it is not intended. In addition to education on bullying, could we provide nurses with resources and education to improve self-esteem and self-worth to combat feelings of being less and allowing bullying to affect daily [work].
DEI: A YEAR OF CHANGE?
We asked nurses whether their workplaces’ approach to DEI has changed over the past year. More than half (56%) said it had not, and 17% said it had been “strengthened.” However, 19% said the approach had been “weakened” and 8% said it had been “eliminated.”
The more than 100 people who added additional details to their responses highlighted the wide range of impacts.
“Government mandate/law changed DEI programming and courses, as courses/programs DEI language was changed or eliminated in 2026 due to new government law/mandate,” noted one.
Several respondents commented on subtle changes in terminology and labeling, but not in practice. A response typical of that view: “My hospital immediately changed the name of the initiative, and carried on as before.”
“Because of the current administration’s stance on DEI, we are creatively ‘relabeling’ our work to avoid being targeted,” said another. “This is a shame, as our organization has received multiple awards for its DEI work. People should not be marginalized for their birth and origin.”
Several respondents expressed their displeasure with DEI initiatives in healthcare. For example, one said, “I don’t believe DEI is effective. I think it should be eliminated.”
What changes have you seen?
When asked “Has your facility’s approach to DEI changed over the past year?” most respondents said it hadn’t. More than 100 provided details.
- My FQHC [Federally Qualified Health Center] eliminated specialty programs due to funding cuts.
- Although wording had been modified, our mission and values hold true to DEI. All are welcome and diversity adds value to our organization as a whole.
- Changed the name of DEI hospital-wide committee but it is still functioning.
- I think the resources still exist, but it isn’t able to be advertised in an intentional way.
- No longer exist, some of the work has been recategorized, but I couldn’t even get permission to share ANA materials r/t Racism in Nursing.
- DEI has NO PLACE in HEALTHCARE.
- We seem to be hoping to wait this out without undoing our programs in the hope that we might be able to resume normal operations should the current environment change.
A TOUGH JOB THEY WOULD CHOOSE AGAIN
Slightly fewer nurses reported their emotional health as “healthy” or “very healthy” (60% vs. 64% in the previous survey), and the percentage of those describing themselves as not emotionally healthy (14% vs. 15%) was down slightly. Instead, more respondents chose “neutral” (26% vs. 21%) instead of “healthy” to describe their emotional state.
However, most of those taking the survey this year and in years past said they did not regret their chosen career. In fact, the number improved this year from 76% to 81% who said they would still choose nursing if they had to do it again.
Words of advice from your colleagues
Once again, nurses passed along the best advice they’ve received. Here’s what they shared:
- You are only human, you cannot do, heal, or fix everything.
- Trust the patient along with your nursing experience for best outcomes.
- Continue with personal development and follow standards of practice at all times.
- Always ask questions and never be afraid to ask them.
- As a nurse leader, the best advice I received was to lead with humility. You can’t support your team if you don’t listen to their concerns and meet them where they are.
- Always advocate fearlessly for your patients—their voices deserve to be heard, even when it’s difficult.
- Build a strong support network of colleagues. Nursing can be isolating, and having people to lean on makes all the difference.
- Document like you are going to be called into court years later to justify your documentation.
- Get a good mentor! I only have had one during my career and it was very rewarding and stimulating!
- The only certainty in healthcare is change, so get used to it.
- The best advice is to practice radical empathy. Remember that every patient is someone’s loved one, and treat them as you would want your own family to be treated.
- While in nursing school, say yes to every offer/opportunity to perform/practice a skill.
- It will be the hardest thing you ever do, but it will be worth it.
- It’s okay to take a step back and think before taking a nursing action.
- An ounce of discipline weighs less than a ton of regret.
- The bigger the sign-on bonus the sooner you’ll want to leave.
- A mentor told me to listen to my patients more than I speak to them, because their stories hold the key to providing truly compassionate care.
A valuable salary resource
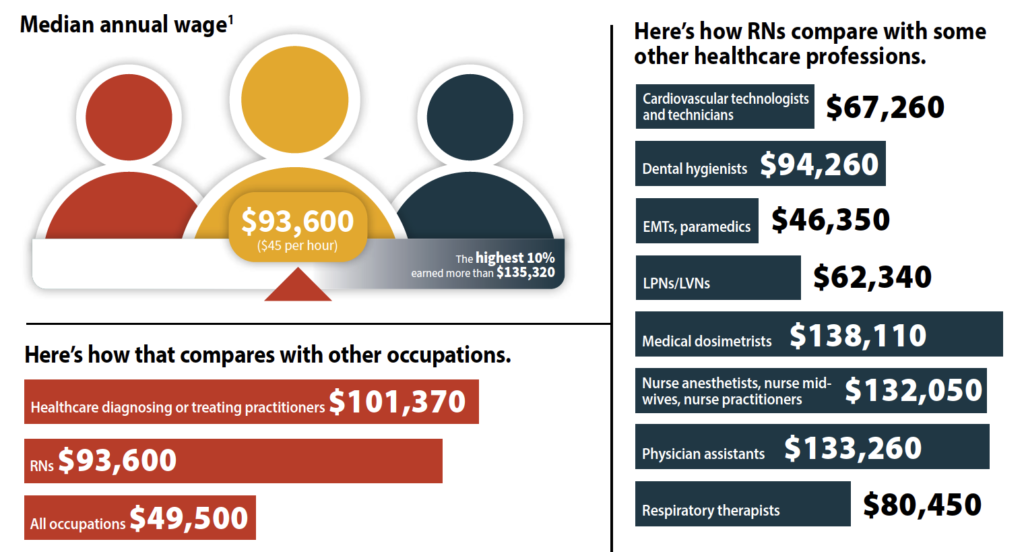
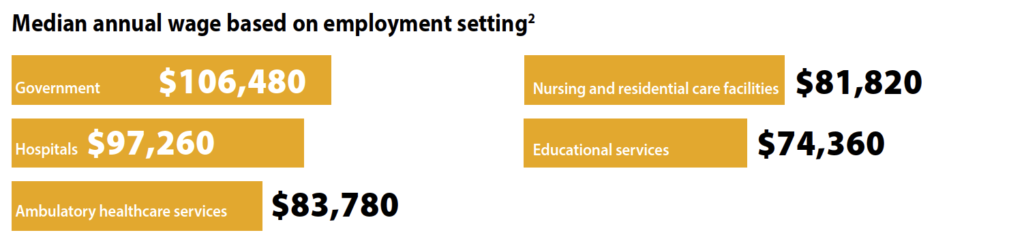
Nurses deserve to be well compensated, but first they need to know their worth. The Bureau of Labor Statistics (BLS) website offers a wealth of salary information that nurses can use to help determine whether they’re receiving fair pay or if a potential new employer might offer sufficient funds to justify a change in position. Below are BLS data related to RNs. The data were last updated in May 2024, so nurses should research current offerings in their region.
Nurses also should consider other factors that affect salary, including cost of living, years of experience, and staff shortages. Salary serves as only one component of a compensation package. Health insurance and tuition reimbursement can compensate for a lower salary. Finally, a higher salary can’t make up for a poor work environment, and nurses seeking a new career path outside their areas of expertise may need to accept a lower salary until they build their skills. With all that in mind, here are the data.
To access pay by state for various nursing occupations, visit www.bls.gov/oes/2024/may/oessrcst.htm. Data points include employment numbers, hourly mean and median wages, and annual mean wage, as well as hourly and annual wages by percentile (10th, 25th, 75th, and 90th). To see two illustrations of the regional variations, see New York and Texas: Regional salary variations.
New York and Texas: Regional salary variations
Go online to see the relative standard errors (RSEs)–a measure of the reliability of a survey statistic. The smaller the RSE, the more precise the estimate.
percentile wage
percentile wage
Go online to see the relative standard errors (RSEs)—a measure of the reliability of a survey statistic. The smaller the RSE, the more precise the estimate.
Pay by state with COL adjustment
In April 2025, Becker’s Hospital Review published the hourly mean wage adjusted for cost of living (COL) for nurses in each state and the District of Columbia, using 2024 BLS data and COL data from the World Population Review. Check your state at: bit.ly/4d1BQRM. After the adjustment, Oregon had the highest hourly mean wage at $51.71, and Hawaii had the lowest at $31.82.
Source: Bureau of Labor Statistics, U.S. Department of Labor, Occupational Outlook Handbook, Registered Nurses. www.bls.gov/ooh/healthcare/registered-nurses.htm#tab-1
David J. Gilmartin is a digital content editor at HealthCom Media in Plymouth Meeting, Pennsylvania. Cynthia Saver is a medical writer in Columbia, Maryland.
American Nurse Journal. 2026; 21(4). Doi: 10.51256/ANJ042613
Key words: artificial intelligence, bullying, DEI, staffing