Learn about the symptoms and treatment options, and cultivate a referral network.
Takeaways:
- Anxiety disorders commonly present in primary care settings, and advanced practice RNs (APRNs) will benefit from understanding treatment options that promote positive outcomes.
- Several effective nonpharmacologic options exist that APRNs can recommend to patients with anxiety symptoms.
- Pharmacologic options should be provided with a clear understanding of safety and efficacy.
Amanda, a 45-year-old woman, visits her primary care office with trouble sleeping, heart racing, and a tingling sensation around her mouth. She reports frequent headaches and GI discomfort. Despite a normal physical exam and diagnostic test results, the patient continues to have symptoms. The advanced practice RN (APRN) notes that Amanda’s symptoms, which disrupt her home and work life, seem to increase during stressful life events. The APRN wonders how to help relieve this patient’s distress and reduce her anxiety.
Preparing RNs for emerging roles in primary care
Succeeding as a primary care nurse
Anxiety attack or myocardial infarction?
Many primary care APRNs may recognize patients like Amanda in their difficulty providing relief. Anxiety disorders, some of the most common mental health conditions seen in primary care, frequently manifest with physical symptoms (including chronic headaches, muscle tension and pain, GI upset, heart palpitations, chest pain and tightness, fatigue, trembling or shaking, sweating/sweaty palms, shortness of breath, dizziness, chills or heat sensation, and sleep disturbances). Anxiety may be the predominant disorder or it may be a symptom of other disorders.
APRNs working in primary care should be prepared to discuss anxiety with their adult patients and offer appropriate treatments. Anxiety in children is beyond the scope of this article.
Etiology
Distress, uncertain circumstances, and even positive-yet-stressful situations (such as an upcoming wedding) can trigger anxiety. Intact coping skills aid spontaneous anxiety resolution with time. Anxiety disorders are diagnosed when symptoms persist for a specified length of time, depending on the diagnosis. Anxiety becomes clinically relevant when it causes significant distress or interferes with an individual’s social, work, or academic functioning.
Most psychiatric disorders are multifactorial and multifaceted. For example, an individual’s genetic predisposition for psychiatric disorders can be triggered by stressors in the environment that cause changes in the brain’s function. The Adverse Childhood Experiences Study demonstrated an association between early childhood trauma and physical and mental health conditions in adulthood.
Screening tools
All patients who report physical symptoms (such as pain, shortness of breath, and fatigue) should be screened for depression and anxiety. Screening for depression starts with the Patient Health Questionnaire (PHQ)-2, a validated two-item tool that can be integrated into intake forms and nursing triage during primary care appointments. Patients who score more than 3 should then be screened with the PHQ-9. Another tool specific for anxiety disorders but less widely known is the Generalized Anxiety Disorder (GAD)-2 tool, which if positive (score >3) is followed by the GAD-7.
Diagnostic criteria
The Diagnostic and Statistical Manual of Mental Disorders 5th Edition (DSM-5) categorizes anxiety as either a predominant symptom in a condition identified as an anxiety disorder or a symptom of another mental health disorder. Anxiety diagnoses include (those most commonly treated in primary care are noted in green)
- agoraphobia
- anxiety disorder due to another medical condition
- generalized anxiety disorder
- other specified anxiety disorder
- panic disorder
- selective mutism
- separation anxiety disorder
- social anxiety disorder
- specific phobia
- substance/medication-induced anxiety disorder
- unspecified anxiety disorder
Primary care APRNs can assess and treat several of the anxiety disorders described in the DSM-5. However, patients with symptoms of more complex problems, such as mutism, phobias, bipolar disorder, psychotic disorders, obsessive–compulsive disorder (OCD), and post-traumatic stress disorder (PTSD), should be referred to a mental health professional (psychiatric mental health nurse practitioner, clinical nurse specialist, psychiatrist, or psychiatric physician’s assistant) for further evaluation and treatment. Patients may present with symptoms of anxiety due to other diagnoses such as adjustment disorder with anxiety, autism, and attention deficit and hyperactivity disorder.
Patient assessment
Evaluate anxiety symptoms beginning with a clear understanding of the history and course of illness. Some patients experience primarily cognitive anxiety-related symptoms (excessive worry, difficulty controlling worry, trouble concentrating), whereas others experience physical symptoms (jittery, keyed-up, or on-edge; fatigue; rapid heart rate; shortness of breath). Other patients may have a combination of both cognitive and physical symptoms.
Determine whether the symptoms are constant or intermittent, and ask about aggravating and alleviating factors. Start with open-ended questions such as, “Tell me more about what’s going on?” After obtaining a general description of the symptoms, narrow down the assessment with closed questions such as “How many days per week do you experience the anxiety?” To gauge severity, consider the level of functional impairment. (See Anxiety assessment.)
Anxiety assessment
Take a systematic approach to assessing patients for anxiety.
History and course of illness
- Aggravating and alleviating factors
- Constant vs. intermittent
- Duration
- Level of impairment
- Suicide risk
- Symptom quality (cognitive vs. physical)
Rule out medical conditions
- Cardiac conditions
- Hyperthyroidism
- Hypoglycemia
- Pheochromocytoma (rare)
Consider substance use
- Caffeine
- Cocaine or other stimulants
- Marijuana
- ETOH withdrawal
- Opiates
- Prescription or over-the-counter medications
Assessment tools
Trauma assessment
Anxiety symptoms may be associated with past trauma and can be understood as hypervigilance to perceived external threats. People who’ve experienced trauma have a heightened response to threat due to its effect on their nervous systems. Patients may describe these symptoms as “paranoia” or “anxiety.” Further assessment can help you determine whether these symptoms meet the medical definition of paranoia or are more closely aligned with a trauma response. Consider asking, “Some people experience thoughts that the government or the FBI is watching them or out to get them. Is that what you’re experiencing? Or do you have the feeling that you need to constantly look over your shoulder and are easily on edge when you’re around other people?” Patients experiencing hypervigilance as a response to trauma will typically agree that the latter best describes their symptoms.
Medical assessment
Rule out medical conditions that might cause or contribute to anxiety. Hyperthyroidism can cause a jittery, anxious feeling, and anxiety is a symptom of pheochromocytoma. Start with a careful physical exam and assessment of vital signs, and evaluate the patient’s thyroid stimulating hormone levels, complete blood count, and comprehensive metabolic panel to rule out potential differential diagnoses.
Medication assessment
Ask the patient about substance use including illicit drugs, alcohol, caffeine, nicotine, and over-the-counter (OTC) medications. Some drugs can contribute to anxiety symptoms when they’re being actively used (cocaine, methamphetamine, or other stimulants) or when the patient is experiencing withdrawal (nicotine, alcohol, opiates, or marijuana). Patients who use alcohol, even in moderate amounts, can wake up with mild alcohol withdrawal symptoms including feeling shaky and anxious. Some patients find that their anxiety symptoms resolve when they reduce or eliminate caffeine intake.
OTC medications, such as pseudoephedrine and dietary supplements marketed to boost energy or aid weight loss, can produce side effects that resemble anxiety. The same is true of prescription drugs such as corticosteroids and bupropion. Complete a thorough medication reconciliation and substance-use assessment. Also consider a urine drug screen.
Safety assessment
Don’t hesitate to ask patients about suicidal thoughts. No evidence indicates that asking these questions contributes to a higher risk for self-harm or worsens thoughts the patient may already be having. Use a straightforward approach with a mix of open-ended and closed questions. Consider starting with: “Sometimes when people are depressed (or anxious) they contemplate taking their own life. Is this a part of your experience?” Passive suicidal thoughts such as “I feel like life isn’t worth living anymore” should be distinguished from active thoughts with a plan or intent. Patients with active thoughts of suicide should be treated as a medical emergency that requires expert evaluation.
In addition, distinguish nonsuicidal self-harm from suicidal behavior. Some patients engage in superficial cutting, scratching, or burning with no intent to die. These behaviors frequently occur when the person is experiencing heightened emotions such as a depressed mood or severe anxiety. To identify patients who may be having suicidal thoughts, use a comprehensive tool that assesses for both risk and protective factors.
Treatment
Nonpharmacologic approaches comprise the foundation of anxiety treatment. They include providing education about how anxiety occurs, the mind–body connection, and trigger recognition. To improve patient resilience during times of stress, support healthy coping strategies and behaviors—nutritious diet, regular sleep patterns, physical activity, socialization, participation in meaningful activities, and mindfulness (including meditation or prayer). Approach patient follow up and support treatment adherence as you would other chronic conditions. Also provide resources to community groups, books, apps, and YouTube videos that teach mindfulness and meditation skills.
Nonpharmacologic treatment also includes psychotherapy, so develop a referral network of mental health professionals. Cognitive behavioral therapy (CBT) has the best evidence for effectiveness. Other modalities also are supported by evidence, and some patients may prefer a different approach. Interpersonal therapy is based on developing a therapeutic relationship between therapist and client and is less structured than CBT. Psychodynamic therapy addresses developmental experiences and their impact on current functioning. In both alternatives, patient and therapist rapport may be more important than the specific modality.
Other therapies may be indicated for specific conditions. For instance, trauma-focused therapy for patients with PTSD and exposure-and-response prevention therapy for those with OCD. Make referrals to your mental health colleagues to evaluate patients for these therapies.
Pharmacologic approaches
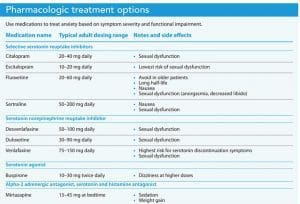
Pharmacologic anxiety treatment typically starts with selective serotonin reuptake inhibitors (SSRI) and serotonin norepinephrine reuptake inhibitors. These medication classes are widely prescribed for both anxiety and depression in primary care settings. They have few contraindications, a low risk profile, and are well tolerated by most patients. One drawback is their relatively slow onset of action (up to 8 weeks for the full effect). An adequate trial of a medication consists of 4 to 8 weeks at a therapeutic dose. Some patients may require higher doses for symptom remission. If the medication is well-tolerated, slowly titrate the dose to the maximum range. If the patient can’t tolerate the medication, try another. To determine effectiveness, look for symptom improvement and overall functioning. To obtain measurable data, consider repeating the PHQ-9 and GAD-7 screening tools.
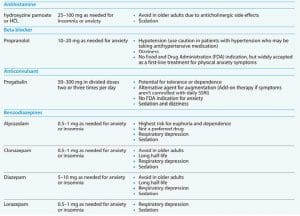
For patients with acute symptoms, a short-term prescription of a fast-acting agent may be needed. Benzodiazepines have several risks. Patients can develop tolerance and dependency and may have adverse outcomes from sedative effects. Tolerance can develop quickly, within 2 to 4 weeks, especially in patients who use these medications daily. Educate patients about benzodiazepines’ potential harmful effects, and limit the medication’s use to short-term symptom relief while waiting for SSRI effects. Prescribe the minimum quantity of pills, and don’t approve refills without seeing the patient.
Another option for acute anxiety relief is hydroxyzine pamoate or hydroxyzine hydrochloride. Early studies indicate that these sedating antihistamines can be effective for anxiety. They’re commonly prescribed as an alternative to benzodiazepines. These medications have anticholinergic effects, so exercise caution when prescribing them to older adults.
Evidence supports using pregabalin as needed or scheduled to treat anxiety symptoms, and the beta-blocker propranolol can be used as scheduled or as needed for panic disorder and social anxiety disorders, especially performance anxiety. Both medications target physical anxiety symptoms, including shakiness, tremors, headaches, and racing heart. (See Pharmacologic treatment options.)
Maintain competency
Primary care APRNs frequently see patients with anxiety symptoms and must maintain their competency in the diagnosis and evidence-based treatment of anxiety disorders. Maintain a strong referral network to connect patients with psychotherapy providers, monitor patients long-term, and provide ongoing education and support.
Amanda’s primary care APRN refers her to a therapist for weekly counseling sessions to learn coping skills to manage feeling overwhelmed and anxious. Her APRN also prescribes escitalopram (10 mg daily) and hydroxyzine pamoate (25 mg as needed) for breakthrough anxiety. Amanda reports nausea when starting escitalopram, but the APRN helps her manage the temporary side effects and continues to monitor her and provide education and support. Several months later, Amanda reports feeling “like herself again” and finds occasional headaches and minor illnesses less disruptive to her daily routine. After Amanda remains symptom-free for 10 months, the escitalopram is tapered off and she continues to see a therapist.
The authors are clinical assistant professors at Virginia Commonwealth University School of Nursing in Richmond.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013.
Centers for Disease Control and Prevention. About the CDC-Kaiser ACE Study. April 6, 2021.
Fergus TA, Kelley LP, Griggs JO. The combination of health anxiety and somatic symptoms: A prospective predictor of healthcare usage in primary care. J Behav Med. 2019;42(2):217-23. doi:10.1007/s10865-018-9956-1
Love AS, Love R. Anxiety disorders in primary care settings. Nurs Clin North Am. 2019;54(4):473-93. doi:10.1016/j.cnur.2019.07.002
Massoudi B, Holvast F, Bockting CLH, Burger H, Blanker MH. The effectiveness and cost-effectiveness of e-health interventions for depression and anxiety in primary care: A systematic review and meta-analysis. J Affect Disord. 2019;245:728-43. doi:10.1016/j.jad.2018.11.050
Slee A, Nazareth I, Bondaronek, P, Liu Y, Cheng Z, Freemantle N. Pharmacological treatments for generalised anxiety disorder: A systematic review and network meta-analysis. Lancet. 2019;393(10173):768-77. doi:10.1016/S0140-6736(18)31793-8
Zero Suicide. Toolkit.
Zhang A, Franklin C, Jing S, et al. The effectiveness of four empirically supported psychotherapies for primary care depression and anxiety: A systematic review and meta-analysis. J Affect Disord. 2019;245:1168-86. doi:10.1016/j.jad.2018.12.008

















1 Comment.
very good assessment and treatment, safe use of pharmacologic non-pharmacologic treatment and good outcome