The right dressing helps to ensure moisture balance and promote wound healing.
- Appropriately treating and dressing wounds can be an intimidating, confusing, and frustrating issue for clinicians.
- Evidence-based care involves moist wound healing and proper antimicrobial treatment.
- To identify underlying diseases and etiologies, clinicians should perform comprehensive patient assessments before establishing a wound treatment plan.
Learning Objectives
- Identify evidence-based principles of wound care, including moist wound healing and appropriate antimicrobial use.
- Apply clinical reasoning to select appropriate wound treatments and dressings based on individual patient needs and current best practices.
Consider these reflective questions as you read:
- How does this information on wound care challenge or reinforce my current practice, and what steps can I take to ensure my assessments are more comprehensive and patient-centered?
- What systems-level changes (e.g., policies, workflows, education) could be influenced by this knowledge to improve wound healing in my patients?
No relevant financial relationships were identified for any individuals with the ability to control content of the activity.
Expiration: 11/1/28
Some nurses find wound dressing selection intimidating and frustrating. Businesswire estimates that more than 5,000 wound care products exist in the United States, in a myriad of shapes and sizes, each designed to address different wound characteristics and stages of healing.
For many years, the standard of wound care included applying normal saline wet-to-dry dressings, typically twice a day. However, according to Ovington, this dressing choice can potentially impede healing by disrupting healthy tissue upon removal; cool the wound when used with room temperature saline; create pain with dressing removal; prolong the inflammatory response; distribute bacteria into the air, leading to cross contamination; and promote inefficiency with multiple dressing changes per day. Since the 1962 publication of veterinarian George Winter’s seminal paper, which demonstrated that film dressings heal wounds quicker than wet-to-dry dressings, additional studies have determined that wounds heal best in a properly balanced moist wound environment.
According to Jaszarowski and Murphree, organizations frequently cite cost as a reason to shy away from advanced wound dressings, which, depending on their properties, may provide exudate control, maintain a moist wound surface, reduce bacterial loads, and protect the wound against trauma and pathogenic invasion. Ovington presented a study in home care showing the cost-effectiveness of dressings such as hydrocolloids, foams, and absorptive dressings (calcium alginates and hydrofibers), rather than gauze dressings, when factoring in labor costs and faster wound healing along with reduced patient pain. Gauze dressings are no longer the standard of care in modern wound healing.
So how do nurses choose the appropriate wound care dressing for the best evidence-based outcomes, including faster healing times, less pain with application and removal, and cost effectiveness? A wound dressing algorithm can prove helpful.
Before implementing the wound dressing algorithm, the clinician must complete a comprehensive patient assessment that includes a past medical history. Knowing underlying conditions and the wound’s likely etiology can help the healthcare team address any physiologic or systemic issues that may impact healing. (See What to consider.)
What to consider
During wound assessment, ask the patient the following questions:
- How long has the wound been present?
- Do you have a history of pressure wounds?
- Do you have any mobility or continence issues?
- What wound treatments have already been implemented and how did the wound respond?
- Do you have any underlying nutrition or hydration issues, including recent unintended weight loss, decreased appetite, or swallowing or chewing difficulties?
- What medications do you currently take? Do you have any allergies?
- Do you smoke, have alcohol use disorder, or use recreational drugs?
- If the patient has diabetes, also ask the following: What is your diabetes regimen? How successful is it at controlling your diabetes?
- Do you have an advanced directive? What are your goals of care?
- What cultural, religious, or ethnic factors should the team consider?
- What is your living situation? Do you have sufficient support?
Consider the following with regard to the patient’s medical history:
- Assess the patient’s cognitive status. Cognitive status can impact the patient’s ability to understand the plan of care and follow instructions.
- Determine whether any pressure issues exist. Continued pressure on the wound results in compromised blood flow and impedes wound healing.
- If the patient has a lower extremity wound, perform a brief vascular exam (palpate pulses, and check extremity temperature, capillary refill, and sensation) to assess arterial blood supply and possible need for vascular referral. Wounds can’t properly heal in the presence of vascular compromise.
- If the patient has diabetes, review their lab results (HbA1c and daily glucose data) to assess diabetic control. Elevated blood sugar levels can lead to reduced circulation, neuropathy, compromised immune response, and increased inflammation.
Moist wound healing
At the center of the algorithm sits the concept of moist wound healing. Since Winter’s 1962 study, we know the old adage “let it get air” no longer holds true. Rather, a moist wound environment allows for epithelialization at a rate twice as fast as that of dry conditions, prevents desiccation, enhances neoangiogenesis and collagen synthesis, and increases the breakdown of dead tissue and fibrin. According to Ermer-Seltun and Rolstad, a proper dressing choice will maintain moisture balance based on wound exudate. In the process, patients may experience reduced pain, a lowered risk of infection, less scar tissue and necrosis, and faster healing with better outcomes. (See Wound algorithm.)
Wound algorithm
Moist wound healing sits at the center of the wound algorithm.
![]()
The amount of exudate at the wound–dressing interface guides the selection of an appropriate dressing to maintain optimal moisture balance within the wound. To determine the amount of exudate, use the following guideline by Richlen:
- None (no drainage)—Dry dressing and wound bed
- Scant—Nothing measurable on the dressing, wound bed moist
- Small/minimal—<25% of the dressing involved, wound bed very moist
- Moderate—25% to 75% of the dressing involved, wound bed wet
- Large/copious—>75% of the dressing involved, wound filled with fluid
Wound assessment
After a comprehensive patient assessment, evaluate the wound through visual inspection, palpation, and odor assessment. Examine and document the wound’s exact anatomic location and parameters, such as size (length, width, depth), and any undermining or tunneling. Undermining involves destruction of tissue under the intact skin around the wound edge; tunneling refers to a tract that can occur anywhere in the wound bed and tunnels into the tissue below it. Include wound bed descriptors such as percentages of granulation and/or necrotic tissue, amount and type of exudate, any odor, signs of infection, staging if the wound is a pressure injury (don’t stage wounds not directly attributable to pressure), any pain related to the wound, and the condition of the periwound area.
According to Nix, standard of care calls for at least weekly wound assessment, guided by patient factors, setting, and wound severity. Some wounds may require more frequent assessment, especially if they don’t respond to treatment. Both initial and subsequent wound assessments should include data collection and documentation of the same parameters described above. In addition, determine how adequately the dressing maintains proper moisture balance, absorbs and contains exudate, and provides adequate wound coverage.
Wound cleansing
Meticulous cleansing of the wound and surrounding skin is critical to removing liquid or crusted exudate, debris, bacteria, and foreign bodies such as hair, visible soil, liquefied dead tissue, and biofilm without damaging viable tissue in the wound bed.
The solution and the cleansing method used should reduce bacterial load but not interfere with healing. No global consensus on the best method and solution exists. Percival and Mayer describe the use of appropriate solutions, including saline and commercial wound cleansers, which have the advantage of containing wetting agents, emulsifiers, and antimicrobials, as well as a surfactant to loosen, soften, and sequester debris and necrotic tissue. Haesler and colleagues and Swanson advise cleansing the skin around the wound with a mild skin cleanser or pH-balanced soap and water.
For dirty, infected, or chronic wounds, which inevitably have a high bioburden (presence of pathogenic organisms), consider antiseptic solutions such as sodium hypochlorite, hypochlorous acid, or acetic acid. Ideally, apply these with irrigation using low pressure (4 to 15 psi), such as with a 35 mL syringe and a 19-gauge catheter (7 psi), and a commercial cleanser packaged in a pressurized container, or pulsatile lavage. After establishing a clean wound bed, consider discontinuing the use of cytotoxic solutions or antiseptics, unless it’s a low concentration. In general, cytotoxic antiseptics can impede the laying down of collagen and consequently impede wound healing.
Debriding necrotic tissue
Wound bed debridement (the process of removing necrotic tissue as well as biofilm and bioburden) is critical to preparing the wound bed for granulation and healing. Wounds with necrotic tissue may respond to autolytic, enzymatic, mechanical, sharp, and/or biologic debridement, depending on the status of the wound, patient health status and tolerance, and available resources. Debridement methods can occur in isolation or concomitantly.
Autolytic. Autolytic debridement involves a dressing or product that supports an optimum amount of moisture for cell proliferation, while simultaneously promoting proteolytic enzymes to liquify and separate dead from healthy tissue. Dry wounds may not support cell proliferation, and heavy exudate interferes with new cell growth. Monitor the wound routinely for type and quantity of exudate, and modify the dressing to maintain proper moisture levels. Autolytic debridement is highly selective, impacting only dead tissue and not newly granulating cells. It can be performed in all settings as long as the proper dressings are available. According to Ramundo, these include hydrocolloids, transparent films, Manuka honey, hydrogels, or any topical agent that adds or maintains a moist wound bed, as well as absorptive dressings for moister wounds.
Autolytic debridement alone isn’t appropriate for wounds with a significant amount of slough or eschar or for infected wounds. However, it can be used alongside other debridement methods, such as surgical and mechanical debridement. Autolytic debridement can prove slower than other debridement methods; its effectiveness depends on adequate leukocyte function, which if absent, can leave the wound in an inflammatory and nonhealing state.
Enzymatic. Enzymatic debridement involves a 2-mm-thick edge-to-edge application of a prescription ointment that contains collagenase enzymes, which selectively digest necrotic tissue. Although slow, this method is faster than autolytic debridement alone and should be done daily.
Cover the wound with a moist normal saline dressing or some other type of a moisture-retentive dressing. According to Ramundo, enzymatic debridement is compatible with topical antibiotics but not with iodine products and some products containing silver. It can be combined with other methods of debridement and also with negative-pressure wound therapy.
Mechanical. Nonselective, mechanical debridement removes not only necrotic material and surface bacteria but also healthy cells and tissue. In addition, it’s potentially painful for the patient. According to Ovington, although saline-moistened gauze dressings applied multiple times a day are the most common type of mechanical debridement, they’re no longer considered standard of care. Other methods of mechanical debridement include high-pressure pulsed irrigation or lavage, typically performed in the operating room or at a specialized clinic.
Sharp. Advanced providers (physicians, nurse practitioners, physician assistants, and in most states, wound care certified RNs) can perform conservative sharp debridement, which generally involves selective removal of loose necrotic tissue at the bedside. The provider removes only nonviable tissue. For larger wounds, nonselective sharp debridement—performed in the operating room, in a clinic setting, or at the bedside by a provider with surgical expertise—involves removing necrotic tissue down to bleeding tissue. It typically requires local or general anesthetic for pain control.
Biologic. Biologic debridement uses sterile maggots placed on the wound bed. The larvae assist in controlling infection and debriding wounds by digesting biofilm and devitalized tissue, thereby promoting the regeneration of healthy tissue and healing. The larvae, which accomplish this without harming viable tissue, increase in girth from about 2 mm to about 10 mm within 48 to 72 hours. According to Jordan and colleagues, the number of necessary treatments depends on the size, depth, and complexity of the wound.
Treating biofilm and infection
Shree and colleagues describe biofilm, which consists of polymicrobial communities of bacteria and other pathogens, as being held together by a sticky matrix of polysaccharides, proteins, and DNA, which make them more resistant to antibiotics, disinfectants, and the body’s immune system. Biofilm typically can’t be seen with the naked eye, but visual markers can suggest critical colonization or its presence. Excessive exudate, odor, unhealthy tissue that bleeds easily, and a lack of response to antiseptics and antibiotics can point to the presence of biofilm.
Treatment of biofilm involves removing as much necrotic tissue as possible via meticulous wound hygiene, sharp debridement, and application of topical antiseptic and antimicrobial dressings. Sen and colleagues describe the importance of managing systemic and host factors, such as correcting high blood glucose values and addressing vascular and pressure issues.
Infected wounds typically display signs of inflammation, including warmth, swelling, pain, foul odor, increased exudate, and periwound erythema that extends more than 2 cm from the wound edge. The patient also may have a fever. Chronic wounds, as defined by Netsch, typically don’t show improvement within 2 to 4 weeks of comprehensive evidence-based therapy. Additionally, according to the International Wound Infection Institute, only subtle signs of bacterial overgrowth may exist. Some covert and overt signs of local infection in a chronic wound include hypergranular tissue (an overgrowth of friable granulation tissue), pale and smooth granulation tissue, new or increasing pain, and increased exudate with malodor.
Wound infection management can include local treatments such as antimicrobial wound dressings; serial sharp debridement, if needed; and surgical incision and drainage of underlying abscesses. Systemic antibiotics are then prescribed. Suspicion of wound bed infection typically calls for culturing. According to Weir and Schultz and colleagues, swab cultures are acceptable, although a tissue biopsy is the gold standard. If osteomyelitis is suspected, imaging should be performed, as the presence of bone infection can delay or prevent wound healing or require antibiotic treatment. MRI is the most accurate test for this condition.
Balancing moisture
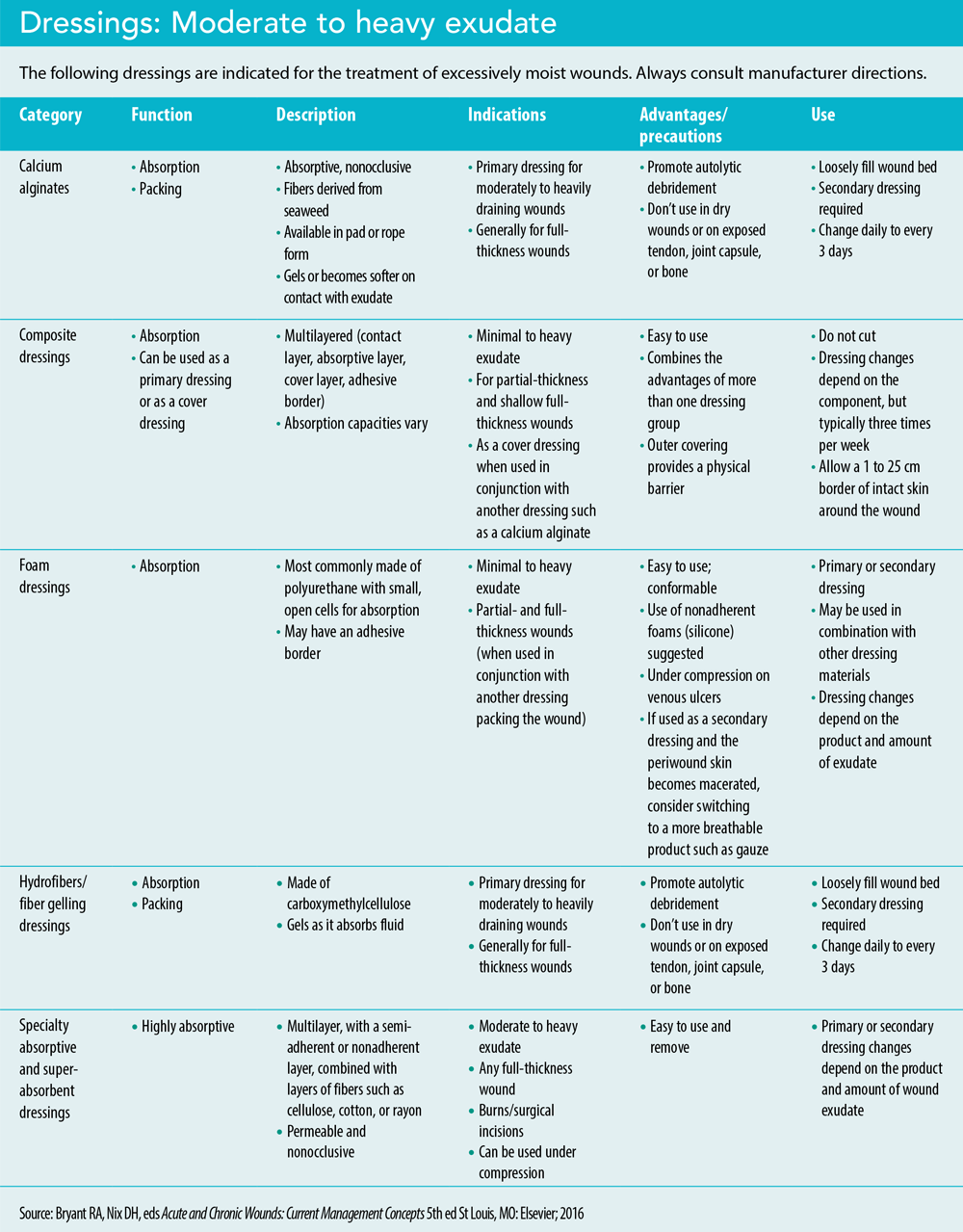
Assess the dressing and the amount and type of exudate with each dressing change. A quickly saturated dressing or macerated skin around the wound indicates a large amount of drainage (exudate), overpowering the dressing. Maceration, an overhydration of the skin, increases the risk of altered skin integrity. Thayer and colleagues describe macerated skin as typically appearing moist, white, and wrinkled. In the event of large amounts of exudate, select more absorptive dressings such as calcium alginates, fiber gelling dressings (hydrofibers), composite dressings, or foam dressings. Treatment for macerated skin includes using a skin barrier wipe or other barrier product, such as zinc oxide. (See Dressings: Moderate to heavy exudate)
Note the type of exudate. Is it serous, sanguinous, serosanguinous, seropurulent, or purulent? Purulence, odor, and increased exudate may suggest developing biofilm or infection, which may require a topical antimicrobial dressing with consideration of systemic antibiotics. (See Exudate types.)
Exudate types
- Serous—Thin, clear/light yellow, watery
- Sanguinous–Bloody
- Serosanguinous—Pink, combination of blood and serum
- Seropurulent—Thin, milky
- Purulent—Thick, typically yellow or green
Frequency of dressing changes also depends on the amount of exudate. According to Jaszarowski and Murphree, very wet or very dry wounds may require more frequent dressing changes to maintain optimal moisture balance. Follow manufacturer directions for proper application and dressing change frequency.
Kelechi and colleagues describe wounds resulting from chronic venous insufficiency as having a moderate-to-heavy amount of exudate in the presence of edema, which also can impede healing. Lower extremity compression garments and wraps, applied over wound dressings from the base of the toes to just below the knee, aid healing by promoting venous return. Before applying compression therapy, complete a bedside vascular exam and, if possible, an ankle brachial index (ABI). Carmel and Bryant describe ABIs as critical to initial assessments, as compression may be contraindicated or require modification in the event that vascular compromise stems from an arterial factor. Suspicion of vascular compromise should trigger referral to a vascular surgeon. (See Venous ulcer.)
Venous ulcer

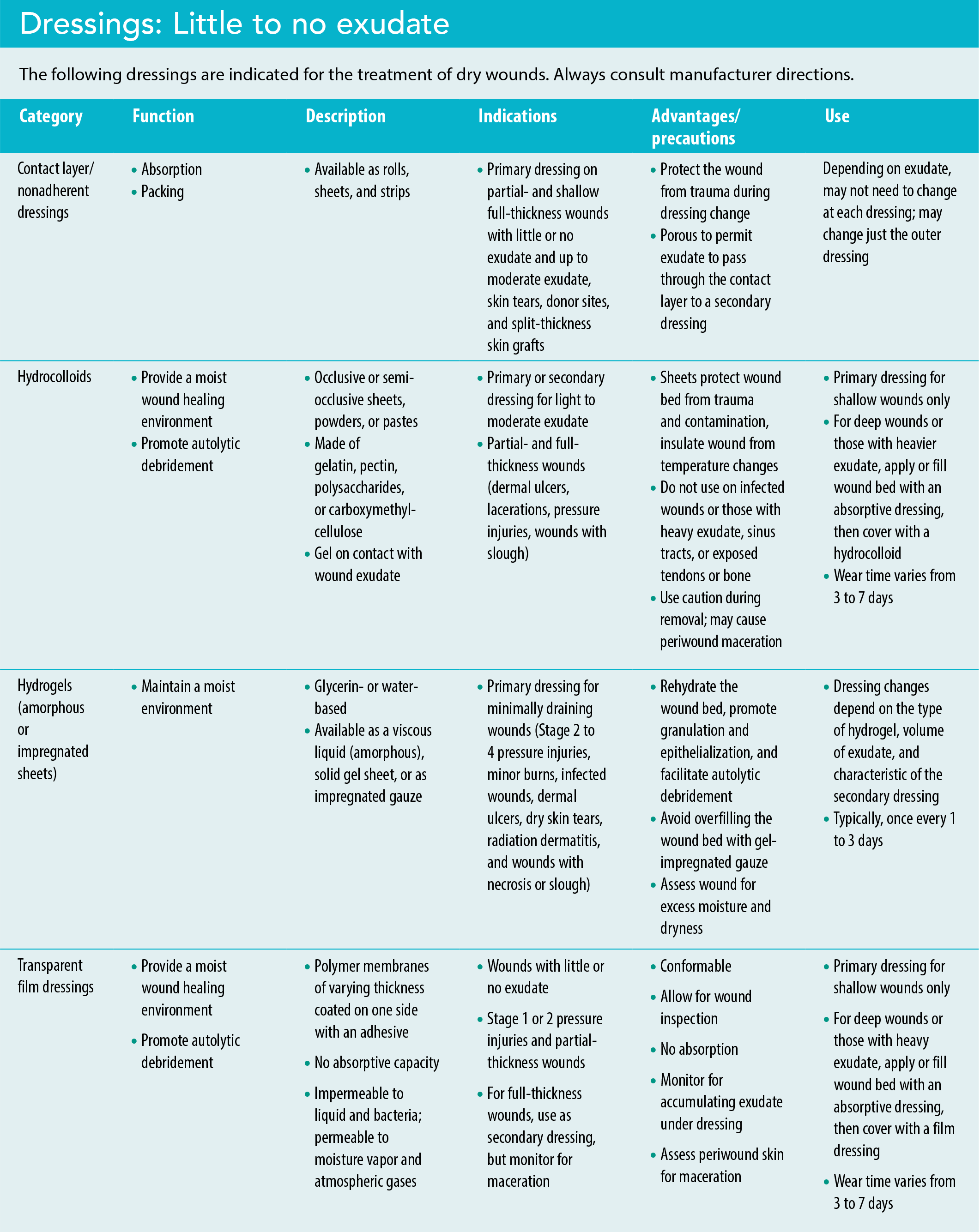
For dry wounds, those with little exudate, or if the dressing adheres to the wound bed during dressing changes, moisture-retentive and hydrating dressings can help. These include hydrogels, contact layer/nonadherent dressings, hydrocolloids, and transparent adhesive dressings. (See Dressings: Little to no exudate)
Filling defects
Wounds heal from the inside out, gradually filling in with granulation tissue from the base up to a level where epithelialization occurs. For this reason, wounds with large soft-tissue defects, including undermining or tunneling, require thorough yet gentle packing to fill (but not overfill) the dead space between the surface of intact healthy skin and the actual wound base. Packing reduces physiologic dead space, absorbs exudate/seroma collection, and limits the potential for infection.
Wicking agents (dressings placed into tunnels or undermined areas) help evacuate fluid and allow the wound to heal from the inside out. This prevents premature closure at a superficial level, which can lead to subcutaneous abscesses and infection. Wicking agents are available in plain and antimicrobial formulations and a variety of materials such as alginates, hydrofibers, foams, textiles, or nonwoven gauze. To aid retrieval of any material in a tunnel, use one continuous piece of wicking and leave a 2- to 3-cm tail protruding from the tunnel. Gently pack the tunnel or undermined area first; then fill the wound with the selected wound dressing. Finish with a cover or secondary dressing.
Lack of wound response
According to Wallace and colleagues, wounds should show improvement or heal in 4 to 6 weeks. If no improvement occurs within that time, re-evaluate the care plan to ensure that all impediments to healing have been addressed, including patient health factors and the treatment plan. Among other factors, revisit whether diabetes is well-controlled, pressure areas have been adequately offloaded, and biofilm and infection are sufficiently addressed with appropriate debridement. In addition, reassess for ample wound perfusion and whether the patient is experiencing anemia or nutritional deficiencies. A wound biopsy may help to rule out malignancy in the wound. Healing of some wounds may not be an option, and care goals may require alteration, especially in the case of skin failure or end of life.
In some cases, changing the wound treatment plan may involve initiating negative pressure wound therapy or making a referral to a wound care center or plastic surgeon. More advanced wound therapies include hyperbaric oxygen therapy, electrical stimulation, growth factors, acellular matrix tissues, biological and bioengineered therapies, amniotic membranes, and skin grafts and flaps.
Enhance healing, prevent pain
Over 60 years have passed since George Winter’s groundbreaking research showed that wounds heal best in a moist environment. Knowing wound dressing basics helps all clinicians, including bedside nurses with little experience in wound care, ensure that patients receive evidence-based care aimed at enhancing healing and preventing pain.
Heidi H. Cross is a consultant at HHC Wound Care Consulting in Skaneateles, New York, and works at the University of Rochester Medical Center, Strong Memorial Hospital in Rochester, New York. Cathleen T. Van Houten is the WOC nursing program manager at the University of Rochester Medical Center, Strong Memorial Hospital.
American Nurse Journal. 2025; 20(11). Doi: 10.51256/ANJ112506
References
Alves PJ, Barreto RT, Barrois BM, Gryson LG, Meaume S, Monstrey SJ. Update on the role of antiseptics in the management of chronic wounds with critical colonisation and/or biofilm. Int Wound J. 2021;18(3):342-58. doi:10.1111/iwj.13537
Armstrong DG, Meyr AJ. Basic principles of wound healing. UpToDate. May 12, 2025. uptodate.com/contents/basic-principles-of-wound-healing?search=wound%20healing&source=search_result&selectedTitle=1%7E150&usage_type=default&display_rank=1
Armstrong DG, Meyr AJ. Principles of wound management. UpToDate. May 29, 2025. uptodate.com/contents/basic-principles-of-wound-management?search=wound%20healing&source=search_result&selectedTitle=3%7E150&usage_type=default&display_rank=3
Beitz JM. Wound healing. In: McNichol LL, Ratliff CR, Yates SS, eds. Core Curriculum: Wound Management. 2nd ed. New York, NY: Wolters Kluwer; 2022.
Businesswire. United States wound care market report 2023-2028—Demand for advanced wound care segment remains high and forecast to drive incremental growth of over one billion USD. businesswire.com/news/home/20230809193771/en/United-States-Wound-Care-Market-Report-2023-2028—Demand-for-Advanced-Wound-Care-Segment-Remains-High-and-Forecast-to-Drive-Incremental-Growth-of-Over-One-Billion-USD—ResearchAndMarkets.com
Carmel JE, Bryant RA. Venous ulcers. In: Bryant RA, Nix DH, eds. Acute and Chronic Wounds: Current Management Concepts. 5th ed. St. Louis, MO: Elsevier; 2016.
Ermer-Seltun JM, Rolstad BS. General principles of topical therapy. In: McNichol LL, Ratliff CR, Yates SS, eds. Core Curriculum: Wound Management. 2nd ed. New York, NY: Wolters Kluwer; 2022.
Haesler E, Swanson T, Ousey K, et al. International wound infection institute (IWII). Therapeutic wound and skin cleansing: clinical evidence and recommendations. Wounds International. 2025. woundsinternational.com/wp-content/uploads/2025/03/IWII_2025_Wound-cleansing-web-2.pdf
International Wound Infection Institute. Wound Infection in Clinical Practice: Principles of Best Practice. 3rd ed. London, UK: Wounds International; 2022.
Jaszarowski K, Murphree RS. Wound cleansing and dressing selection. In: McNichol LL, Ratliff CR, Yates SS, eds. Core Curriculum: Wound Management. 2nd ed. New York, NY: Wolters Kluwer; 2022.
Jordan A, Khiyani N, Bowers SR, Lukaszczyk JJ, Stawicki S. Maggot debridement therapy: A practical review. Int J Acad Med. 2018;4(1):21-34. doi:10.4103/IJAM.IJAM_6_18
Junker JPE, Kamel RA, Caterson EJ, Eriksson E. Clinical impact upon wound healing and inflammation in moist, wet, and dry environments. Adv Wound Care. 2013;2(7):348-56. doi:10.1089/wound.2012.0412
Kelechi TJ, Brunette G, Burgess JJ. Lower extremity venous disease, venous leg ulcers, and lymphedema. In: McNichol LL, Ratliff CR, Yates SS, eds. Core Curriculum: Wound Management. 2nd ed. New York, NY: Wolters Kluwer; 2022.
Malone M, Schultz, G. Challenges in the diagnosis and management of wound infection. Br J Dermatol. 2022;187(2):159-66. doi:10.1111/bjd.21612
Netsch D. Refractory wounds: assessment and management. In: McNichol LL, Ratliff CR, Yates SS, eds. Core Curriculum: Wound Management. 2nd ed. New York, NY: Wolters Kluwer; 2022.
Nix DP. Skin and wound inspection and assessment. In: Bryant RA, Nix DH, eds. Acute and Chronic Wounds: Current Management Concepts. 5th ed. St. Louis, MO: Elsevier; 2016.
NSW Government. Harvesting medical-grade maggots for old school wound care. https://pathology.health.nsw.gov.au/articles/harvesting-medical-grade-maggots-for-old-school-wound-care/
Ovington LG. Hanging wet-to-dry dressings out to dry. Home Healthc Nurse. 2001;19(8):477-83. doi:10.1097/00004045-200108000-00007
Percival SL, Mayer D, Kirsner RS, et al. Surfactants: Role in biofilm management and cellular behaviour. Int Wound J. 2019;16(3):753-60. doi:10.1111/iwj.13093
Ramundo JM. Principles and guidelines for wound debridement. In: McNichol LL, Ratliff CR, Yates SS, eds. Core Curriculum: Wound Management. 2nd ed. New York, NY: Wolters Kluwer; 2022.
Richlen B. Learn how to determine what wound exudate is telling you. Wound Care Education Institute. July 1, 2020. blog.wcei.net/learn-determine-wound-exudate-telling
Schultz G, Bjarnsholt T, James GA, et al. Consensus guidelines for the identification and treatment of biofilms in chronic nonhealing wounds. Wound Repair Regen. 2017;25(5):744-57. doi:10.1111/wrr.12590
Sen CK, Roy S, Mathew-Steiner SS, Gordillo GM. Biofilm management in wound care. Plast Reconstr Surg. 2022;148(2):275e-88e. doi:10.1097/PRS.0000000000008142
Shree P, Singh CK, Sodhi KK, Surya JN, Singh DK. Biofilms: Understanding the structure and contribution towards bacterial resistance in antibiotics. Med Microecology. 2023;16:100084. doi:10.1016/j.medmic.2023.100084
Swanson T, Ousey K, Haesler E, et al. Wound infection in clinical practice: Principles of best practice. International Wound Infection Institute. 2022. woundinfection-institute.com/wp-content/uploads/IWII-CD-2022-web-1.pdf
Thayer D, Rozenboom BJ & LeBlanc K. Prevention and management of moisture-associated skin damage (MASD), medical adhesive-related skin injury (MARSI), and skin tears. In: McNichol LL, Ratliff CR, Yates SS, eds. Core Curriculum: Wound Management. 2nd ed. New York, NY: Wolters Kluwer; 2022.
Thomas DC, Tsu CL, Nain RA. The role of debridement in wound bed preparation in chronic wound: A narrative review. Ann Med Surg. 2021;71:102876. doi:10.1016/j.amsu.2021.102876
Tran DL, Huang RW, Chiu ES et al. Debridement: Technical considerations and treatment options for the interprofessional team. Adv Skin Wound Care. 2023: 36(4):180-7. doi:10.1097/01.ASW.0000920660.07232.f7
Vogt PM, Andree C, Breuing K, et al. Dry, moist, and wet skin wound repair. Ann Plast Surg. 1995;34(5):493-9. doi:10.1097/00000637-199505000-00007
Wallace HA, Basehore BM, Zito PM. Wound healing phases. StatPearls. June 12, 2023. ncbi.nlm.nih.gov/books/NBK470443/
Weir D, Swanson T. Ten top tips: Wound cleansing. Wounds International. 2023;10(4):8-11. woundsinternational.com/wp-content/uploads/2023/02/96b7ce193d8c20293723a42c128239cb.pdf
Winter GD. Formation of the scab and the rate of epithelialization of superficial wounds in the skin of the young domestic pig. Nature. 1962;193:293-4. doi:10.1038/193293a0
Key words: wound dressings, chronic wounds, moist wound healing