
A simple, scalable, and holistic innovation
- The independent double-check (IDC) process for high-alert medications requires two clinicians to independently review and verify the five rights of medication administration.
- A nurse-led team developed a visual mobile safety zone in the form of a light-up lanyard that nurses could activate while performing IDC.
- Initiatives like this demonstrate the benefits of nurse-led safety and innovative care efforts.
Medication errors contributing to adverse events remain one of the leading causes of death in the United States. According to Rodziewicz and colleagues, medical errors (a broad category that includes medication errors) cost between $20 billion and $40 billion annually. Across healthcare settings, nurses play a key role in the medication process, particularly around administration. In acute care settings, a study conducted by Walsby and colleagues suggests that nurses spend 20% to 40% of their clinical time administering medications.
Errors can occur at all steps in the medication process, from ordering to administration. In a systematic review of the literature, the World Health Organization found a 22% prevalence of administration errors in the review of 41,000 patients with medication-related harm.
I.V. medications add a layer of complexity, with many additional opportunities for error. Pump programming and simultaneously administering multiple medications can lead to errors related to confusion associated with the various pumps, I.V. lines, and tubing. Pump programming requires several steps, and infusing multiple medications through one or more pumps increases the risk of mixing up lines, selecting incorrect channels, or connecting the wrong medication to the wrong infusion site. This work takes place in a setting where nurses manage multiple care needs, offer support and education to patients and families, and foster a culture of professional collegiality.
According to the Institute for Safe Medication Practices (ISMP), high-risk medications, such as insulin, anticoagulants, and parenteral nutrition, carry the greatest risk of significant harm if given incorrectly. Healthcare organizations create their own high-alert medication lists, combining recommendations from the ISMP and internal safety event data.
The independent double-check (IDC), a common practice aimed at decreasing the risk of errors when administering high-alert medications, involves two licensed clinicians (nurse, prescriber, pharmacist) independently reviewing and confirming the five rights of medication administration. The duplicity of this process assumes that redundancy will improve accuracy.
Nurses act as partners in patient safety and frequently provide the last layer of protection in the medication process, identifying and preventing errors. They have first-hand insight into the clinical environment, patient complexity, and workflow challenges, positioning them to function as solutions-oriented, problem-solving innovators. This knowledge and expertise provides opportunities to develop safety interventions.
Understanding the problem
When an internal database indicated challenges related to IDC, an interprofessional team of nurses, quality improvement specialists, and clinical innovation personnel used the Lean Six Sigma approach and the define, measure, analyze, improve, and control (DMAIC) framework to implement a quality improvement (QI) project aimed at understanding the IDC component of medication administration. The Lean Six Sigma approach and DMAIC framework provided a step-wise, data-driven structure to the team’s evaluation of the problem and implementation of interventions.
Initially, two nurse executives sponsored the project, which was led, in part, by a former neo-natal intensive care unit nurse working as a clinical quality improvement specialist. The interprofessional team divided into a smaller core team responsible for conceiving the solution and included nurses from diverse clinical areas such as ICUs and surgical floors. Their frontline experiences proved instrumental in shaping the solution design and functionality.
Using Lean Six Sigma tools, such as process mapping and fishbone diagram creation, the team confirmed that the medication administration process is laden with risk for human factor–related error. Several factors can complicate medication administration, including nurse workload, nurse experience and knowledge, competing priorities, interprofessional communication, nurse fatigue, and technology challenges. By identifying and focusing on two elements associated with medication errors—distraction and competing priorities—the team designed an intervention to reduce risk within the medication administration workflow.
For baseline data collection, a nurse conducted observations of 36 high-alert medication administrations. The average time to complete the IDC was 8 minutes, which confirmed previous literature and QI work by Konwinski and colleagues. During the 36 observations, the number of disruptions ranged from 0 to seven and the length of time to complete the IDC increased in line with the disruptions.
The QI team used a mind mapping exercise and a decision matrix to conceive and prioritize interventions. Mind mapping, a type of brainstorming, allows ideas or topics to branch into related thoughts or subtopics. In talking informally with nursing staff about medication administration and the IDC process, the team determined that nurses found the process burdensome and time-consuming. Nurses commented on the amount of time it can take to find a colleague to complete the IDC and the number of barriers and interruptions that can occur during the process. After this review, the team selected two root causes to focus on: lack of a standardized person with whom to complete the IDC and interruptions during the process. (See Selecting a solution.)
Selecting a solution
The project team used mind mapping and a decision matrix to develop solutions and determine which should take priority.
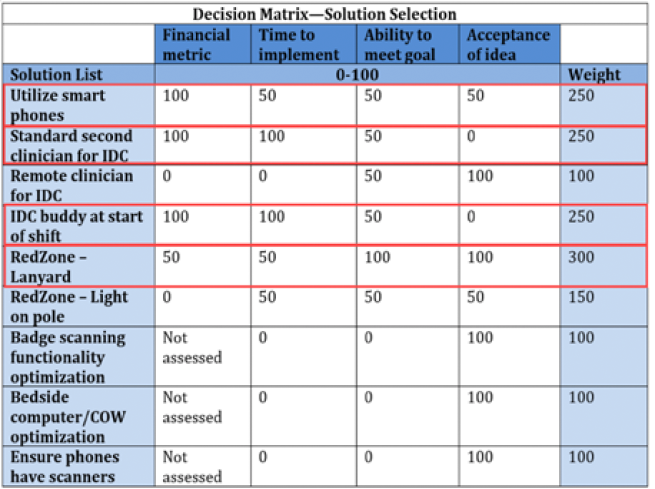
COWS = computers on wheels
Developing the solution
The team’s organization used the red zone strategy, developed by Connor and colleagues, to limit interruptions and distractions. This zone, denoted by badges, signage, and floor decals, identifies the need for distraction-free time. Taking the red zone a step further, nurses on the QI team spearheaded the light-up lanyard innovation, guiding the idea from conception through feasibility testing.
Using design-thinking principles (an iterative approach to problem solving that prioritizes the human involved in the process and their workflows), the nurses built upon the successes of the red zone initiative and identified challenges specific to the IDC workflow. Through collaborative brainstorming sessions, nurse educators, leaders, and interprofessional team members validated the concept to ensure a practical and impactful solution.
In acute care contexts, decision making frequently requires quick thinking and appropriate and recognizable visual cues. However, the types of visual cues used in healthcare aren’t well understood. A systematic review by Patel and colleagues found that no specific recommendations exist for integrated visualizations in an arena such as healthcare. The authors specifically describe holistic integrated visualizations, which convey multiple pieces of information through one display.
Spreading the word
The project team created posters to inform staff of the light-up lanyards and their meaning.
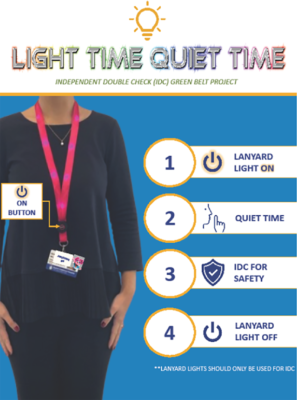
The light-up lanyards, a first of its kind visual mobile safety zone, signals an in-process IDC and that nurses shouldn’t be disturbed. When nurses activate the light-emitting diode lanyards, they create a distraction-free zone that alerts staff, patients, and families to refrain from interruption. The lanyards have an uncomplicated on-off toggle switch to activate and deactivate the lights. The QI team established a catchy slogan—“Light Time Quiet Time!”—to promote the lanyards. (See Spreading the word.)
Key milestones in the creation of the lanyards included a robust proof-of-concept phase, in which the team employed user-centered design principles. Direct care nurses played an active role throughout the process, providing feedback on initial lanyard prototypes to assess functionality and practicality during hands-on design sessions. This feedback informed essential design improvements. For example, one nurse highlighted the need for the lanyard to have a breakaway safety feature to account for pediatric and behavioral health populations. An early prototype included an on-off button, rather than a toggle switch. One nurse found the lanyard had clicked on in their bag after their shift, draining the battery.
One iteration of the lanyards added lights near the breakaway clasp of the lanyard so anyone behind the nurse can see the visual cue. The iterative and user-driven design process resulted in five refined prototypes, the first three of which were rigorously tested to ensure alignment with clinical needs and safety standards. The fourth prototype added antimicrobial fabric and brighter lights. The fifth and final prototype optimized the lanyard color and ensured easy battery access.
Implementing the solution
The team trialed the light-up lanyards, which display several small constant white lights, on a single 42-bed surgical unit in a large Magnet®-recognized, academic, tertiary care, urban pediatric hospital in the Northeast United States. Each nurse on the unit received a lanyard and education on how to use them. Education occurred during staff meetings and unit huddles.
During the pilot, the project team included continuous-infusion high-alert medications in the data collection. They excluded enteral high-alert medications and single doses of high-alert medications, such as insulin. This decision allowed for the inclusion of and control for line reconciliation as part of the time to complete an IDC. Line reconciliation involves a second nurse checking I.V. tubing connections and tracing lines from the source medication container to the patient.
Limitations
The cumbersome data collection process required a nurse to alert the data collection nurse that an IDC was about to begin. Additionally, the inclusion and exclusion criteria limited the number of possible observations.
Occasionally, nursing staff found the lanyards frustrating during busy clinical shifts, as enabling the devices added a step in an already complex process. they also had to ensure others saw the devices and understood what they mean. However, the nurses were engaged and excited to pilot the lanyard, making them excellent partners.
Measuring results
The project team used two primary quantitative metrices to evaluate the lanyards’ efficiency and safety during the pilot. The primary metric, time to complete an IDC, tracked the time from requesting a second nurse to medication administration. The second metric, number of interruptions, accounted for any visual or auditory distractions aimed at one of the two nurses completing the IDC. The team hypothesized that reducing the time to complete an IDC would align with a reduced number of interruptions and reflect improved workflow efficiency.
Even with a limited number of observations (n=12), the team found the results encouraging. The trial revealed a 26% reduction in average IDC completion time; this meant, on average, a decrease of 2 minutes per IDC. Additionally, the team observed a nearly 70% decrease in average interruptions (0.9 fewer interruptions per IDC), showcasing the lanyards’ effectiveness in creating a safer and more focused environment. (See Reduced time.)
Reduced time
This box plot visualization shows a decrease in time to complete the independent double-check (IDC).
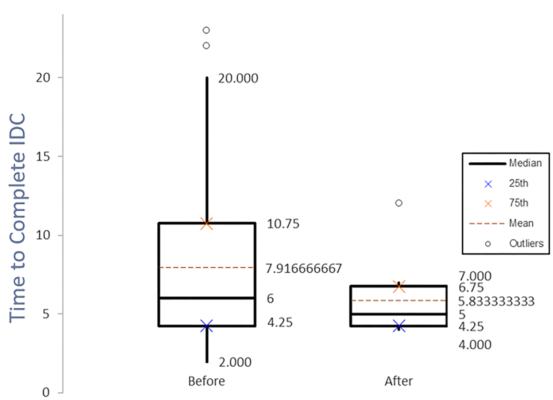
Overall, this straightforward yet powerful innovation minimized interruptions, enhanced nurse focus, and may help eliminate administration errors associated with high alert-medications.
Potential impact
The scalable, low-cost, and adaptable light-up lanyard solution offers a replicable and sustainable approach to improving medication administration safety. The project team will hold the next trial on the medical-surgical ICU in the winter of 2026, with a plan to expand high-alert medication inclusion criteria.
During this next period, the team will collect more extensive data, as well as qualitative data from direct-care nurses, patients, families, and other members of the interdisciplinary team. The results of this next trial will help inform subsequent work. The team aims for hospital-wide adoption, decreased time to complete IDCs, fewer interruptions, and increased patient safety.
In addition to enhancing patient safety, this innovation supports nurse well-being. The light-up lanyard empowers nurses and reduces the stress associated with distractions during medication administration. Simply activating their lanyard may improve job satisfaction, increased autonomy, and visual unity with colleagues.
The broader healthcare team also may benefit indirectly from improved workflows. Although not yet assessed, the project team hopes the lanyards will foster interdisciplinary collaboration and that all members of the care team will recognize the visual cue they provide.
Pharmacists may have greater assurance that medication administration follows strict safety protocols, while technical, administrative, and support staff may better understand when IDCs are in progress, streamlining their interactions with nurses. In this way, the lanyards support a collaborative, safety-centered environment, reinforcing a united approach that can scale across diverse healthcare settings.
From a financial perspective, the lanyards contribute to organizational resilience by reducing costs associated with medication errors and improving operational efficiency.
Safer practice
The light-up lanyard is a simple yet transformative tool crafted with a commitment to practicality, nurse-centered design, and patient safety. Distraction-free zones during IDCs aren’t new, but this innovation leverages visual management that seamlessly integrates into nursing workflows. The lanyards provide an immediate, recognizable, and simple signal to staff, patients, and families of an ongoing IDC that shouldn’t be interrupted.
As the innovation progresses, partnerships with clinical teams and leadership will support expanded use of the lanyards as a scalable model that advances medication safety, fosters patient-centered care, and aligns with organizational quality and efficiency goals. In the evolving healthcare landscape, the light-up lanyards set a new standard for mobile, nurse-led safety interventions, and position nurses as active leaders in patient safety.
The authors work at Boston Children’s Hospital. Julie Murphy is a senior clinical quality improvement specialist. Dorothy Miller is a lead patient safety and quality consultant. Kathryn Gustafson is a retired clinical quality improvement specialist. Alexandra Paulson is a nursing professional development specialist. Jennifer Treseler is a lead clinical safety and quality consultant. Kate Becla is a clinical coordinator. Kate Donovan is director of clinical innovation and education.
American Nurse Journal. 2026; 21(6). Doi: 10.51256/ANJ062624
References
Connor JA, Ahern JP, Cuccovia B, et al. Implementing a distraction-free practice with the red zone medication safety initiative. Dimens Crit Care Nurs. 2016;35(3):116-24. doi:10.1097/DCC.0000000000000179
Konwinski L, Miller K, Steenland C. Leveraging single-checks to improve medication safety. Children’s Hospital Association. 2021. childrenshospitals.org/news/childrens-hospitals-today/2021/07/leveraging-singlechecks-to-improve-medication-safety
Patel AM, Baxter W, Porat T. Toward guidelines for designing holistic integrated information visualizations for time-critical contexts: Systematic review. J Med Internet Res. 2024;26:e58088. doi:10.2196/58088
Rodziewicz TL, Houseman B, Vaqar S, Hipskind JE. Medical error reduction and prevention. StatPearls. 2024. ncbi.nlm.nih.gov/books/NBK499956
Walsby A, Williams S, Gammon J, Best S. The reality of nursing time: How nurses spend their shifts. Br J Nurs. 2024;33(20):968-74. doi:10.12968/bjon.2024.0050
World Health Organization. Global burden of preventable medication-related harm in health care: A systematic review. 2024. www.who.int/publications/i/item/9789240088887
Key words: medication administration, nursing innovation, independent double check, human factors design


















