
This project addressed social isolation and lack of mental stimulation.
- An acute care facility implemented a senior social program to help address the growing issues of cognitive decline and social isolation among older adults.
- Participants reported a positive experience when participating in the senior social.
- Unexpected outcomes included team bonding, improved relationships among nurses and patient care technician, and the development of a more positive work environment that benefited the unit and the hospital as a whole.
According to Knight and colleagues, many older adults remain in acute care settings longer than anticipated due to insufficient insurance and lack of beds in long-term care or assisted living facilities. James and colleagues note that that these longer stays place patients at risk for cognitive impairment.
Our Magnet®-recognized, Level I academic, acute care hospital addressed this issue with a program developed and driven by nurses and patient care technicians (PCTs). The program aimed to provide a daily opportunity for older adult patients to engage socially with their peers and participate in various stimulating activities.
Developing the program
The senior social concept originated with our unit practice council (UPC), which meets monthly to develop initiatives that improve the unit and patient care. The American Nurses Credentialing Center states that a shared governance model, such as a UPC, empowers nurses and enhances ownership and accountability while aligning with the organization’s goals, which include leveraging staff expertise to improve job satisfaction, increase retention rates, and enhance patient care.
Creating the senior social allowed nurses to demonstrate their commitment to evidence-based practice and use their NICHE (Nurses Improving Care for Healthsystem Elders) training. NICHE education emphasizes the importance of understanding the unique health challenges faced by the elderly. Development of this program highlights several key components of the Magnet model, including effective nursing leadership to foster a culture of excellence and professional governance. The UPC, supported by the nursing director, nurse educator, and members of the senior nursing staff, played instrumental roles in creating and implementing the program. The senior social exemplifies professional practice, highlighting the nursing role and its impact on patient care.
Although the program primarily aimed to provide mental stimulation and opportunities for social connection among older adult patients, we structured the intervention as a quality improvement (QI) initiative. Using the Plan-Do-Study-Act (PDSA) model as a guide, we developed the program (Plan), executed it (Do), evaluated outcomes (Study), and made necessary adjustments (Act) based on feedback and observed results. By following the PDSA cycle, we ensured that ongoing improvements were evidence-based and responsive to participant needs.
The outcomes of this strategy met our expectations, facilitating a positive experience for patients. Our UPC defined a positive experience as cultivating a welcoming environment where older adult patients could socialize and feel a sense of belonging through group participation.
The program focused on including activities that promote mindfulness, which Zhang and colleagues define as being present in an open, friendly, nonjudgmental environment. Galassi and colleagues described activities like bingo and arts and crafts as improving cognition and sensorimotor function, fostering self-esteem, enhancing socialization, and promoting overall well-being in older adults.
We also encountered unexpected outcomes, such as team-bonding, strengthening of nurse and PCT relationships, and creating an overall positive work environment. These outcomes had positive effects on the unit and the organization. Although examining our retention rates wasn’t a primary aim, our PCT and nursing retention rates have had no significant change since the implementation of our program.
Importance of a senior social
Jones and Dolsten described an ever-changing hospital landscape with a rapidly growing population of seniors, which is estimated to rise to 83.7 million by 2050. Along with this population increase, the prevalence of high-acuity disability and disease will grow. Several authors, including James and colleagues and Park and colleagues, found that older adults without pre-existing cognitive issues before an extended hospitalization, may experience cognitive decline during the stay, with worsening effects depending on age, illness severity, and duration of hospitalization. Both groups of authors also note that even hospitalizations without delirium or elective surgery can still be associated with significant cognitive decline.
According to the National Institute on Aging, older adults who are hospitalized have an increased risk for anxiety and depression. Dementovych noted that the dullness of hospital stays and isolation from family can have a negative impact on a patient’s long-term cognitive function.
To complicate matters, many patients experience longer stays in acute care settings as they wait for respite beds, rehabilitation beds, and long-term placement because of a lack of insurance coverage and limited bed availability. Most acute care settings don’t offer patient activities as the anticipated length of stay traditionally has been only a couple of days. Assisted living and extended care settings, on the other hand, conduct daily activities to support residents’ cognitive function and socialization.
According to Alzahrani, re-admissions, common among older adults with comorbidities, and extended hospital stays, can negatively impact well-being. Our unit cares for older adults, many with cardiac conditions, who frequently experience readmissions.
Our senior social initiative focused on encouraging patients to participate in various activities and helping them to feel welcome. In an effort to keep this project as simple as possible, we concentrated on patient experience of the senior social. Other factors that could be measured in the future include belonging and cognitive function.
Belonging. Belonging is a fundamental need. According to Allen and colleagues, someone who feels as though they don’t belong will more likely experience physical illness, cognitive decline, and emotional disorders.
Cognitive function. The National Institute on Aging defines cognitive impairment as a disruption to one or more of the following: thinking, reasoning, memory, attention, and social awareness. According to Murphy and Husain, contributors to cognitive decline in older adults include medications such as sedatives, tranquilizers, and anticholinergic drugs; blood chemistry imbalances; vitamin deficiency; hormonal imbalances; neurodegenerative conditions; substance use; stroke; and toxin exposure.
After assessing and treating underlying potential causes of cognitive decline, promoting social contact and mental stimulation becomes critical. However, few studies consider interventions aimed at older adults experiencing cognitive impairment.
Implementing the program
All RNs on our unit have become geriatric resource nurses based on the NICHE model, which uses evidence-based practice resources to deliver care that improves clinical outcomes, reduces costs, and meets national quality goals for the elderly. A study by Davis and colleagues found that nurses with education and experience related to cognitive impairment positively influence the care they provide.
Before initiating the senior social, we asked 10 older adult patients to complete a baseline survey (using a 5-point Likert scale). The data we collected indicated that patients didn’t feel connected to each other and they felt neutral or disagreed with the statement, “I have activities to stimulate my mental cognition while in the hospital.”
Plan
A senior social gathers older adult patients in a designated area to participate in an activity and converse with one another. We’re fortunate to have ample space with a beautiful view, in which we placed small circular tables. Our UPC found research by Tobia and colleagues and Sharp and colleagues that supports using circular tables to enhance conversations.
The UPC developed a calendar of events in collaboration with key stakeholders, including the nurse director, volunteer services to procure a harpist to play music, and the pet therapy department. Patients requiring these services already participated in physical and occupational therapy; therefore, these departments weren’t included in the senior social.
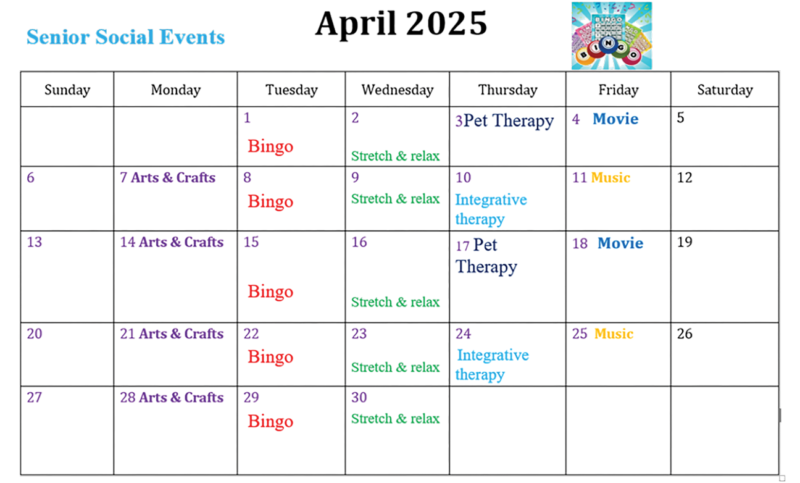
Cost of the evidence-based socialization strategies (bingo, movies, music therapy, arts and crafts) was minimal. The unit already had a bingo game, and we conducted several activities (including music therapy) using a large screen TV. (see Senior social calendar.)
Senior social calendar
The unit-based council created a monthly calendar of activities.
Do
PCTs participated in a brief in-service training led by the nursing staff. The PCTs then facilitated the daily senior social events, which took place Monday through Friday, from 11:30 am to 1:00 pm. Some PCTs flourished in this role, while others required additional guidance, support, and assistance from the nursing staff and nursing director.
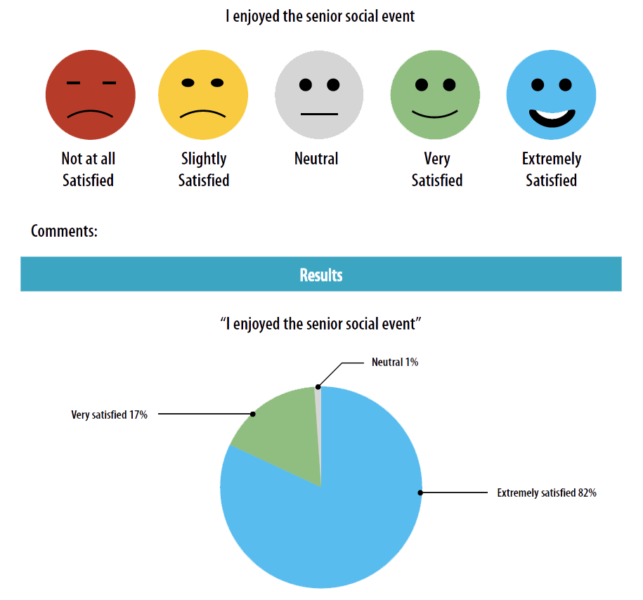
For 3 months, after each event, we asked patient attending the senior social to complete a one-question 5-point Likert scale evaluation form. Administered by the PCTs, the evaluation asked patients to rate their enjoyment of the senior social.
Study
Quantitative survey data indicated that most patients who participated in the senior social enjoyed it—82% described themselves as extremely satisfied and 17%, very satisfied. Qualitative feedback further supported these findings, with patient comments that included “The games were fun to play with new people,” “Thank you for offering an excellent service, this program gave me a great diversion,” “My hospital day did not seem so long,” and “I had a blast.”
Some outcomes proved surprising. The UPC wasn’t anticipating improved relationships among PCTs and nurses, but the senior social program became a team-building experience. Everyone—including the nursing director, floor educator, charge nurses, and nursing students—stepped up to assist when needed. In addition, many patients’ family members, physicians, nurses from other units, caseworkers, and directors commented on how engaging the event was. On days when pet therapy hosted the senior social with five dogs, more hospital staff got involved and laughter from both staff and patients echoed down the hospital corridor.
We invited visiting family members to the senior social. Their feedback, although anecdotal, was positive. They appreciated their loved ones having the opportunity for socialization and expressed gratitude for staff engagement with the patients.
Unfortunately, the Hospital Consumer Assessment of Healthcare Providers and Systems patient experience results don’t represent this patient population, as many patients aren’t discharged home.
Nurse and PCT relationships blossomed as they viewed the senior social as a patient-focused team program. Baek and colleagues describe the relationship between nurses and PCTs as key to good patient care, contributing to a more positive overall work environment. Having PCTs serve in active lead roles enhanced their engagement in this program. In a simple survey, PCTs reported feeling more valued as part of the team. One PCT said, “It was nice to be in charge of running the bingo games and seeing how the patients just loved it.”

Patient response
Patient care technicians administered a simple 5-point Likert scale survey to 160 patients who participated in senior social activities. We factored in the activities patients enjoyed based on topic. Over the 3-month implementation period, bingo rated the highest.
Act
As with the implementation and study of many programs, we made adjustments to ours. We experienced ongoing issues with staff scheduling, which occasionally required unit nurses, rather than a PCT, to run the senior social. To address this issue, we’ve expanded participation to include volunteer services and nursing students working on the floor.
Looking forward, we intend to scale the program to 7 days a week, with a longer-term goal of offering the senior social twice a day and including an evening session for dinner. We’re considering including occupational and physical therapy activities, such as chair yoga.
Replicating the program
Acute care facilities must do more to foster socialization, especially for those at high risk of cognitive decline, such as older adults. Nurses can help create opportunities for socialization in acute care settings, beginning with a resource assessment, including occupational and physical therapy, nursing, PCTs, nursing students, and volunteer services.
In addition, consider a location for the activities and access to supplies. For example, something as simple as coloring pages can be printed from a computer. If you have access to a large screen TV, use it for music therapy and to watch movies.
Rising to the challenge
Although the primary aim of the senior social program was to provide mental stimulation for older adult patients, further research could specifically investigate other outcomes. For example, how does participation in a structured senior social program in an acute care setting affect nursing retention rates, nursing satisfaction, the PCT–nurse relationship, and patient cognitive function over time? Addressing these questions would provide critical insights into the broader impact of such interventions on both staff and patient well-being.
Our senior social program serves as just one example of how implementing a simple nurse- and PCT-driven initiative can lead to positive patient experiences. This initiative becomes even more important as older adults remain in the acute care setting for extended periods. We’re engaging with bedside nurses and other care team members to explore additional patient-centered initiatives. Nurses are rising to the challenge to meet the needs of older patients in new and creative ways.
The authors work at Boston Medical Center in Boston, Massachusetts. Jo Anne Foley is an NPD specialist. Ann Carey is a nurse director.
American Nurse Journal. 2026; 21(6). Doi: 10.51256/ANJ062618
References
Allen KA, Kern ML, Rozek CS, McInereney D, Slavich GM. Belonging: A review of conceptual issues, an integrative framework, and directions for future research. Aust J Psychol. 2021;73(1):87-102. doi:10.1080/00049530.2021.1883409
Alzahrani N. The effect of hospitalization on patients’ emotional and psychological well-being among adult patients: An integrative review. Appl Nurs Res. 2021;61:151488. doi:10.1016/j.apnr.2021.151488
American Nurses Credential Center. Magnet Model—Creating a Magnet Culture. nursingworld.org/organizational-programs/magnet/magnet-model
Baek H, Han K, Cho H, Ju J. Nursing teamwork is essential in promoting patient-centered care: A cross-sectional study. BMC Nurs. 2023;22(1):433. doi:10.1186/s12912-023-01592-3
Davis ER, Aggar C, Bissett M. Nurses’ perception of care practices for adults with cognitive impairment in hospital: A cross-sectional survey. App Nurs Res. 2025;83:151953. doi:org/10.1016/j.apnr.2025.151953
Derrer-Merk E, Ferson S, Mannis A, Bentall RP, Bennett KM. Belongingness challenged: Exploring the impact on older adults during the COVID-19 pandemic. PLoS One. 2022;17(10):e0276561. doi:10.1371/journal.pone.0276561
Dementovych N. Hospitalization can be particularly stressful for elderly patients—It’s important to be aware of the risk and how to help avoid them. Jefferson Health. August 2022. jeffersonhealth.org/your-health/living-well/the-mental-and-physical-effects-of-a-hospital-stay-on-seniors
Galassi F, Merizzi A, D’Amen B, Santini S. Creativity and art therapies to promote healthy aging: A scoping review. Front Psychol. 2022;13:906191. doi:10.3389/fpsyg.2022.906191
James B, Wilson RS, Capuano AW, et al. Cognitive decline after elective and nonelective hospitalizations in older adults. Neurology. 2019;92(7):e960-9. doi:10.1212/wnl.0000000000006918
Jones CH, Dolsten M. Healthcare on the brink: Navigating the challenges of an aging society in the United States. NPJ Aging. 2024;10(1):22. doi:10.1038/s41514-024-00148-2
Knight T, Kamwa V, Atkin C, et al. Acute care models for older people living with frailty: A systematic review and taxonomy. BMC Geriatr. 2023;23(1):809. doi:10.1186/s12877-023-04373-4
Murphy K, Husain, M. Psychotropics and cognitive function: A risk-benefit analysis commentary on “Impact of psychotropic medications on cognition among older adults: A systematic review” by Chandramouleeshwaren et al. Int Psychogeriatr. 2025;37(1):100029. doi:10.1016/j.inpsyc.2024.100029
Murphy TF. Belongingness. Psychology Fanatic. April 2021. psychologyfanatic.com/belongingness
National Institute on Aging. What is mild cognitive impairment? April 2021. nia.nih.gov/health/memory-loss-and-forgetfulness/what-mild-cognitive-impairment
Park D, Kim HS, Kim JH. The effect of all-cause hospitalization on cognitive decline in older adults: A longitudinal study using databases of the National Health Insurance Service and the memory clinics of a self-run hospital. BMC Ger. 2023:23(1):61. doi:10.1186/s12877-022-03701-4
Sharp RA, Williams E, Rörnes R, Lau CY, Lamers C. Lounge layout to facilitate communication and engagement in people with dementia. Behav Anal Pract. 2019;12(3):637-42. doi:10.1007/s40617-018-00323-4
Tobia V, Sacchi S, Cerina V, Manca S, Fornara F. The influence of classroom seating arrangement on children’s cognitive processes in primary school: The role of individual variables. Curr Psychol. 2022;41(9):6522-33. doi:10.1007/s12144-020-01154-9
Zhang D, Lee EKP, Mak ECW, Ho CY, Wong SYS. Mindfulness-based interventions: An overall review. Br Med Bull. 2021;138(1):41-57. doi:10.1093/bmb/ldab005
Zhou Z, Zhang S, Kim YK, Birditt KS, Fingerman KL. Need to belong, daily social engagement, and transient loneliness in late life. J Soc Pers Relat. 2024;41(1):115-36. doi:10.1177/02654075231211617
Key words: cognition, social connection, acute care


















