
What’s the nurse’s role in risk assessment?
- Although personal lifetime breast cancer risk assessment isn’t a new concept, it’s infrequently incorporated into the routine healthcare visits for women.
- Missed opportunities exist to personalize healthcare for each individual woman.
- The Federal Drug Administration, the National Comprehensive Cancer Network, and the American College of Obstetricians and Gynecologists support the integration of this type of screening and encourage nurses in all settings to have these discussions with women based on this assessment.
THROUGH EVIDENCE-BASED education and shared decision-making, nurses play a vital role in closing knowledge gaps and empowering all patients at risk for breast cancer. This article focuses on one of those patient populations—cis-gender women. By providing education on the latest screening guidelines, offering personalized breast cancer risk assessments, and encouraging screenings based on individual risk profiles, nurses can significantly enhance awareness and early detection. (See Breast cancer facts.)
Calculating personal risk
The American College of Obstetricians and Gynecologists (ACOG), the National Comprehensive Cancer Network (NCCN), and the American College of Radiology (ACR) recommend using a lifetime breast cancer risk assessment tool in clinical practice. These validated tools use a patient’s demographics, gynecologic and obstetric history, and family history to calculate the risk of developing breast cancer in their lifetime. Some also include previous cancer or genetic mutation history and breast density in the calculations to further define the estimation of personal risk. Although no universal guideline for assessment frequency exists, the ACR advises completing an initial evaluation by age 30 and updating it periodically. ACOG and the NCCN also agree on the need for personal risk screenings and re-evaluations based on changes in either personal or family history. Integrating risk assessments into patient care supports a personalized approach, encourages shared decision-making, and may improve access to earlier and more comprehensive breast cancer screenings.
Cancer treatment delays and survival outcomes
Recognizing oncologic emergencies
According to ACOG and NCCN, risk assessment calculations that show a <20% lifetime risk for breast cancer indicates average risk. The American Cancer Society, ACOG, and NCCN recommend that individuals at average risk receive education about risk factors and screening guidelines for clinical breast exams and mammography. According to NCCN, women with ≥20% lifetime risk are at elevated risk for breast cancer and should receive education on the impact of the assessment findings and offered additional, optional screenings, including a genetic counseling referral, more frequent clinical breast exams, and supplemental breast imaging (magnetic resonance imaging or ultrasound).
Breast cancer facts
According to Berg and colleagues, breast cancer is the second leading cause of cancer-related deaths in cis-gender women in the United States. The American College of Obstetricians and Gynecologists (ACOG) states that those at average risk for breast cancer face a 1 in 8 chance of being diagnosed during their lifetime.
Risk factors
According to ACOG, several factors can increase breast cancer risk in cis-gender women, including the following.
- Alcohol use
- Dense breast tissue
- Early onset of puberty
- Family history
- Genetic mutation presence
- Late menopause
- Never having given birth
- Obesity
- Post-menopausal hormone use
- Tobacco use
Breast tissue density
In 2023, the U.S. Food and Drug Administration (FDA) amended the Mammogram Quality Standards Act (MQSA) to focus on the impact of density on breast cancer. Dense breast tissue serves as an independent risk factor for breast cancer, and its presence can mask tumors on imaging. As a result, the level of density is now a standardized component of radiological screenings for breast cancer. Healthcare providers must educate women on the risks associated with dense tissue and disclose the category of density found.
Screening guidance
ACOG notes that screening for breast cancer reduces the mortality rates via early detection. In the United States, several resources guide breast cancer screening recommendations for cis-gender women, including the American Cancer Society (ACS), the United States Preventive Services Task Force (USPSTF), ACOG, and the National Comprehensive Cancer Network (NCCN).
- ACOG and NCCN recommend that women at average risk for breast cancer have a basic awareness of their normal breast appearance and feel. They should undergo a clinical breast exam every 1 to 3 years starting at age 25 years and switch to annual clinical breast exams and screening mammograms at 40.
- USPSTF aligns with ACOG and NCCN regarding imaging recommendations; ACS recommends annual mammography in patients age 40 to 54 years and every 1 to 2 years in those ≥54.
- NCCN recommends that women at high risk for breast cancer initiate screenings earlier and states that they may benefit from additional tests to reduce morbidity and mortality risk.
- Screening for personal breast cancer risk determines whether a woman is at average or high risk for breast cancer; the importance of which helps to establish screening recommendations.
Risk screening options
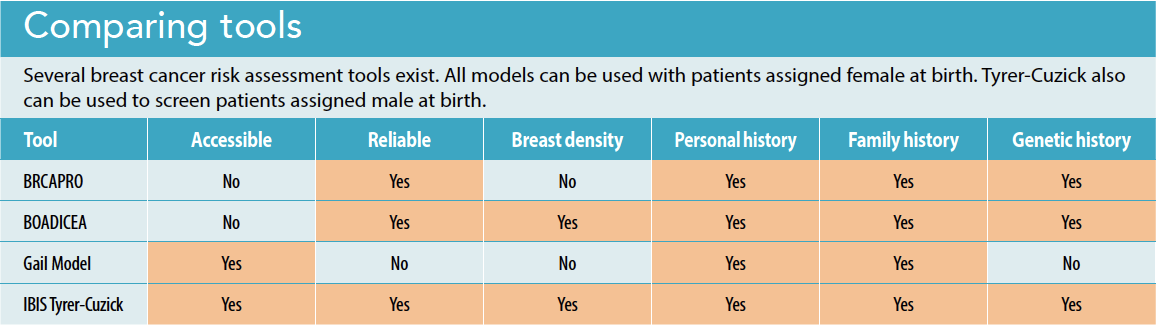
Many validated tools exist for breast cancer risk screening. The Gail Model, BRCAPRO, and Breast and Ovarian Analysis of Disease Incidence and Carrier Estimation Algorithm (BOADICEA) tools all include personal and family history in the risk estimation; however, each has limitations for widespread use. For example, the Gail Model doesn’t include breast density in the risk calculation. Therefore, it’s less reliable when used in certain patient populations, including women with a personal history of breast cancer; women who carry genetic mutations; and Black, Hispanic, and Asian women. The BRCAPRO model also doesn’t include breast density in the calculation, and it requires a subscription, which limits its accessibility. The BOADICEA includes density in the risk assessment, but it’s not easily accessible.
The International Breast Cancer Intervention Studies Tyrer-Cuzick risk evaluation tool stands out for its ability to estimate individual lifetime risk of breast cancer across all age groups and ethnicities. This model includes breast density in the risk calculation; the presence of dense breast tissue not only lowers the sensitivity of mammograms in detecting cancer but also serves as a causative factor for the disease. Nurses across various specialties, practice settings, and licensure levels can easily access the free Tyrer-Cuzick tool. (See Comparing tools.)
Risk education
According to ACOG, Berg and colleagues, and Krueger, exposure to health-related information via social media as well as the experiences of family and friends, which sometimes involve bias and misinformation, can prove highly influential. Healthcare providers, including nurses, serve as valuable resources for evidence-based health-related education. Krueger notes that individuals with little awareness of breast cancer risk factors are less likely to participate in risk-reducing behaviors (such as breast cancer screenings) compared to those who’ve received evidence-based education. Offering education and assessments can help to dispel misconceptions about individual risk and promote adherence to recommended screenings.
Nurses’ role in risk reduction
The Association of Women’s Health, Obstetric, and Neonatal Nurses (AWHONN) issued a position statement supporting nurses as advocates and change agents with regard to educating patients about breast cancer risk, discussing screening standards, and conducting risk assessments in everyday practice. After these conversations, nurses can collaborate with patients to help them make informed decisions about risk-reducing strategies and screening options that fit their needs and preferences. Using a breast risk assessment tool that incorporates breast density is crucial in providing comprehensive care.
Nurses have a unique opportunity to use holistic assessments to improve patient health during screening events, gynecological appointments, or at primary care encounters. The standards for professional practice in women’s health nursing, as established by AWHONN, identify opportunities for nurses to impact breast cancer morbidity and mortality. For example, nurses can create a positive rapport with patients by initiating conversations that explore their thoughts and feelings about breast cancer and personal risk. This connection is reinforced when nurses provide nonjudgmental and safety-focused education that explains evidence-based information about breast cancer risk factors and encourages patients to address modifiable risk factors (such as tobacco and alcohol use).
Nurses should consider implementing breast cancer risk assessments—using a free, easily accessible validated risk assessment tool such as Tyrer-Cuzick—in women by age 30 years. When accessing the online tool, nurses can include, with the patient’s permission, unidentifiable data for analysis. After completing the screening, nurses can partner with advanced practice providers to identify patients at average and high risk. This collaborative team should work with the patient to reinforce breast self-awareness and develop a personalized care plan that includes screenings based on risk assessment findings.
Make a significant impact
Using evidence-based education and shared decision-making, nurses can positively impact patient health by closing knowledge gaps surrounding breast cancer and encouraging participation in screenings based on personal risk. Integrating personal breast cancer risk assessments into practice has the potential to significantly impact health outcomes through early identification and proactive risk management.
Ashley Wittler is an Assistant Professor at Southern Illinois University in Edwardsville.
American Nurse Journal. 2025; 20(11). Doi: 10.51256/ANJ112542
References
American Cancer Society. American cancer society recommendations for the early detection of breast cancer. December 2023. cancer.org/cancer/types/breast-cancer/screening-tests-and-early-detection/american-cancer-society-recommendations-for-the-early-detection-of-breast-cancer.html
American College of Obstetricians and Gynecologists. Breast cancer risk assessment and screening in average-risk women. July 2017. acog.org/clinical/clinical-guidance/practice-bulletin/articles/2017/07/breast-cancer-risk-assessment-and-screening-in-average-risk-women
American College of Obstetricians and Gynecologists. Family history as a risk assessment tool. March 2011. acog.org/clinical/clinical-guidance/committee-opinion/articles/2011/03/family-history-as-a-risk-assessment-tool
Association of Women’s Health, Obstetric and Neonatal Nurses. Standards for professional nursing practice in the care of women, newborns, and people across the life span, ninth edition. J Obstet Gynecol Neonatal Nurs. 2024;53(1):e4-40. doi:10.1016/j.jogn.2023.09.004
Berg WA., Seitzman RL., Pushkin J. Implementing the national dense breast reporting standard, expanding supplemental screening using current guidelines, and the proposed find it early act. J Breast Imaging. 2023;5(6):712-23. doi:10.1093/jbi/wbad034
Centers for Disease Control and Prevention. Breast cancer statistics. June 2025. cdc.gov/breast-cancer/statistics/index.html
Kim G, Bahl M. Assessing risk of breast cancer: A review of risk prediction models. J Breast Imaging. 2021;3(2):144-55. doi:10.1093/jbi/wbab001
Krueger L. Employing a risk assessment tool for shared decision-making in breast cancer screening. Creat Nurs. 2024;30(1):21-8. doi:10.1177/10784535241228582
National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Breast Cancer Risk Reduction. August 28, 2024. https://www.nccn.org/professionals/physician_gls/pdf/breast_risk.pdf
National Comprehensive Cancer Network. Guidelines for Patients: Breast Cancer Screening and Diagnosis. NCCN.org. Published online April 9, 2024. https://www.nccn.org/professionals/physician_gls/pdf/breast-screening.pdf
United States Food and Drug Administration. Mammography quality standards act. Federal Register. March 2023. federalregister.gov/documents/2023/03/10/2023-04550/mammography-quality-standards-act
Key words: personal breast cancer risk, breast cancer risk assessment, breast cancer


















