
This multi-targeted approach includes novel elements aimed at sustaining practice adherence and improving patient safety.
- Central-line associated bloodstream infections (CLABSIs), a nurse-sensitive indicator, remains a common adverse outcome in patients receiving hemodialysis
- CLABSIs result in hospitalizations, morbidity, mortality, and increased healthcare costs.
- Nursing and the entire healthcare team are fundamental to preventing these infections. A multitargeted approach offers an opportunity for success prevention.
Many individuals receiving hemodialysis require a central venous catheter (CVC), which places them at risk for central-line associated bloodstream infections (CLABSIs). The Centers for Disease Control and Prevention (CDC) Making Dialysis Safer for Patients Coalition partnership with the American Society of Nephrology’s Nephrologists Transforming Dialysis Safety Initiative aims to eliminate CLASBIs in these patients. The CDC’s core interventions serve as the gold standard for preventing intravascular CLABSI. In addition, healthcare facilities continue to implement strategies to prevent hemodialysis-related CLABSIs by creating a culture of collaboration and safety for this vulnerable population. (See CLABSI data.)
The acute dialysis unit in a quaternary teaching hospital had four cases of hemodialysis-related CLABSI from January 2019 through May 2019 (compared to no CLABSIs in 2018). The dialysis team (nephrology nurse leaders, nephrology clinical RNs, and nephrologists) partnered with key stakeholders (infection prevention, vascular physicians, advance care providers, and hospitalists) to form an interprofessional CLABSI prevention team focused on examining the problem and developing a multi-targeted approach to prevent CLABSI in hospitalized patients receiving hemodialysis.
Acute kidney injury: A nursing challenge
Central lines: Recognizing, preventing, and troubleshooting complications
CLABSI data
According to the U.S. Renal Data System, more than 85% of individuals who began hemodialysis in 2021 did so via a central venous catheter (CVC) (up from 80% in 2019). Each of these patients is at risk for a central-line association bloodstream infection (CLABSI), which is linked to
hospitalizations, morbidity, mortality, and increased healthcare costs.
- As noted by Rha and colleagues, 2020 National Healthcare Safety Network surveillance data indicated that 4,840 dialysis facilities reported 14,822 bloodstream infections with Staphylococcus aureus. In seven facilities, the rate of S. aureus infection among patients receiving hemodialysis was 100 times higher than in those not receiving hemodialysis.
- Darma and colleagues reported a CLABSI rate of 11.3 cases per 1,000 catheter days. Sahli and colleagues’ study of patients with a femoral hemodialysis catheter, as opposed to a jugular catheter, reported a higher incidence: 16.6 cases per 1,000 catheter days.
- Pitiriga and colleagues reported an association between higher rates of infection and catheter colonization with femoral site catheters compared to internal jugular and subclavian site catheters.
- A study by Poinen and colleagues found that bacteremia (the most common cause of CVC-related hospitalizations) occurred in approximately 9% of hemodialysis patients with a CVC at 1 year.
The literature review
Findings in a study by Shalaby and colleagues indicated that a CVC bundle can significantly reduce CLABSI rates from 6.7 cases per 1,000 catheter days to 4.1 cases. The bundle included hand hygiene; maximal barrier precaution; skin site cleaning with an alcoholic chlorhexidine solution (>0.5 chlorhexidine and 70% alcohol) before CVC insertion and during dressing changes; optimal access site selection; use of a sterile transparent, semipermeable dressing or gauze to cover the catheter site; and scrubbing the catheter ports and hub with an appropriate antiseptic.
Fisher and colleagues cited novel interventions for infection prophylaxis, including a chlorhexidine-coated impregnated transparent exit dressing, a chlorhexidine-coated rod hub device, and an antimicrobial lock. The researchers also reported the importance of a multi-targeted approach that incorporates active patient engagement, staff education, and strict adherence to the CDC’s core strategies for infection prevention.
A similar study by Hamid and colleagues attributed success at CLABSI reduction to an interprofessional team approach and bundled intervention, including patient and family/caregiver education as well as revalidation of nurse competency on CVC care and catheter access management. According to Parker and colleagues, implementing a standardized care and infection prevention program can reduce the risk of hemodialysis bloodstream infections. Staff behavior and practices impacted the success of these interventions, and leadership and teamwork facilitated infection prevention.
The structure and process
In May 2019, the CLABSI prevention team developed and implemented a multi-targeted approach aimed at preventing hemodialysis-associated CLABSIs. The nephrology nurse leaders created the educational module based on the CDC guidelines for the prevention of intravascular catheter–related infections as well as organizational and departmental policies and procedures. (See Multi-targeted approach.)
Multi-targeted approach
Prevention of central line–associated bloodstream infections in hospitalized patients receiving hemodialysis included the following bundle elements.
*Novel strategies
Before implementing the new approach, nephrology RNs completed mandatory education (via the organization’s learning management system) in initiating and discontinuing hemodialysis treatment and performing catheter care. Through direct observation (during initial orientation, ongoing, and annually), nephrology nurse leaders assess nephrology RN competency. (See Nurse competencies.)
Nurse competencies
Through direct observation, nephrology nurse leaders assess initial and ongoing nurse competencies, including initiation and discontinuation of hemodialysis treatment and catheter site care.
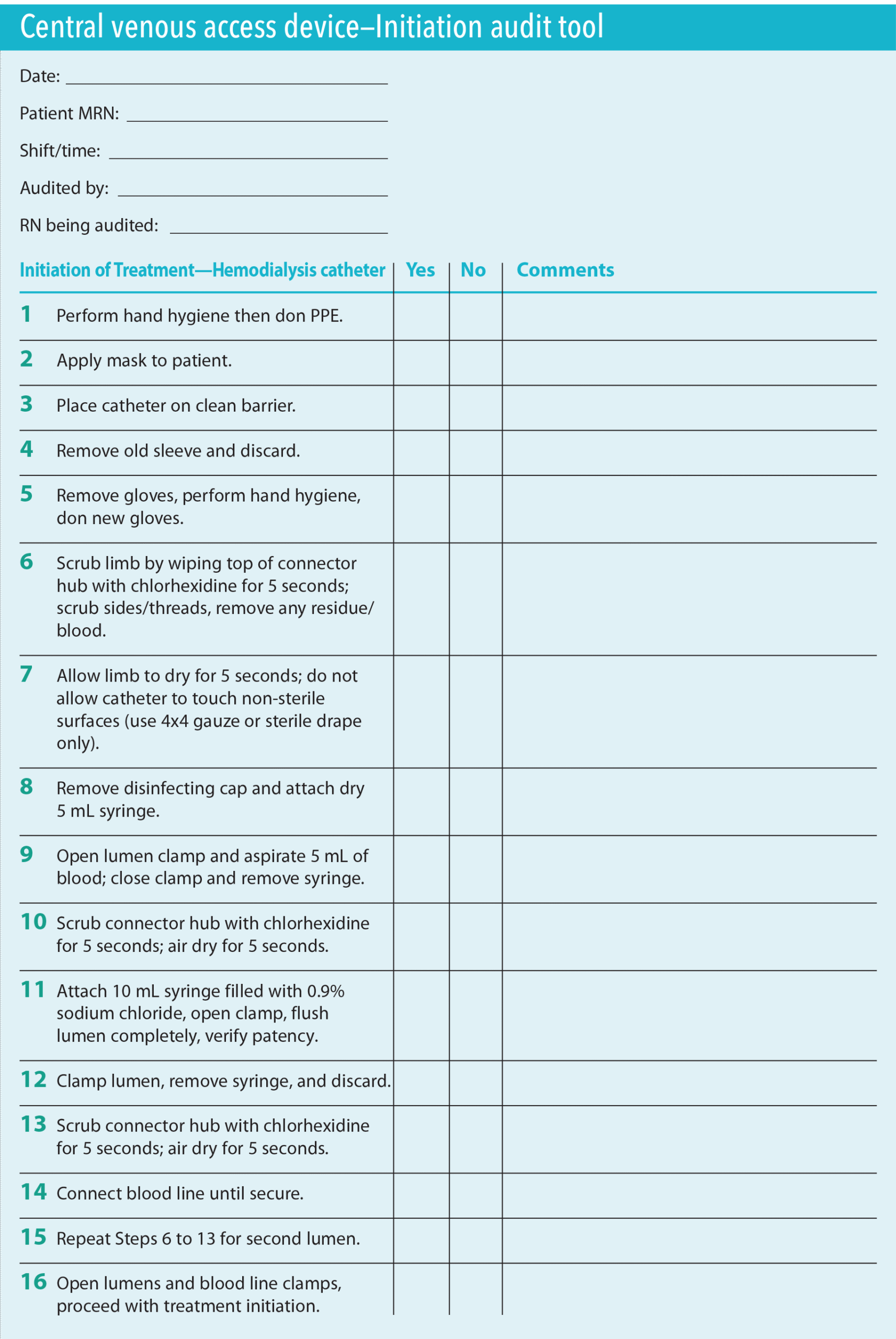
Initiation of hemodialysis with a central venous catheter (CVC) using aseptic technique
- Perform hand hygiene and then don personal protective equipment (such as disposable gown and clean gloves).
- Place mask on yourself first and then the patient.
- Place the catheter on a clean barrier.
- Scrub the catheter hub with a chlorhexidine gluconate (CHG) swab for 5 seconds and allow to air dry.
- Connect the blood line aseptically.
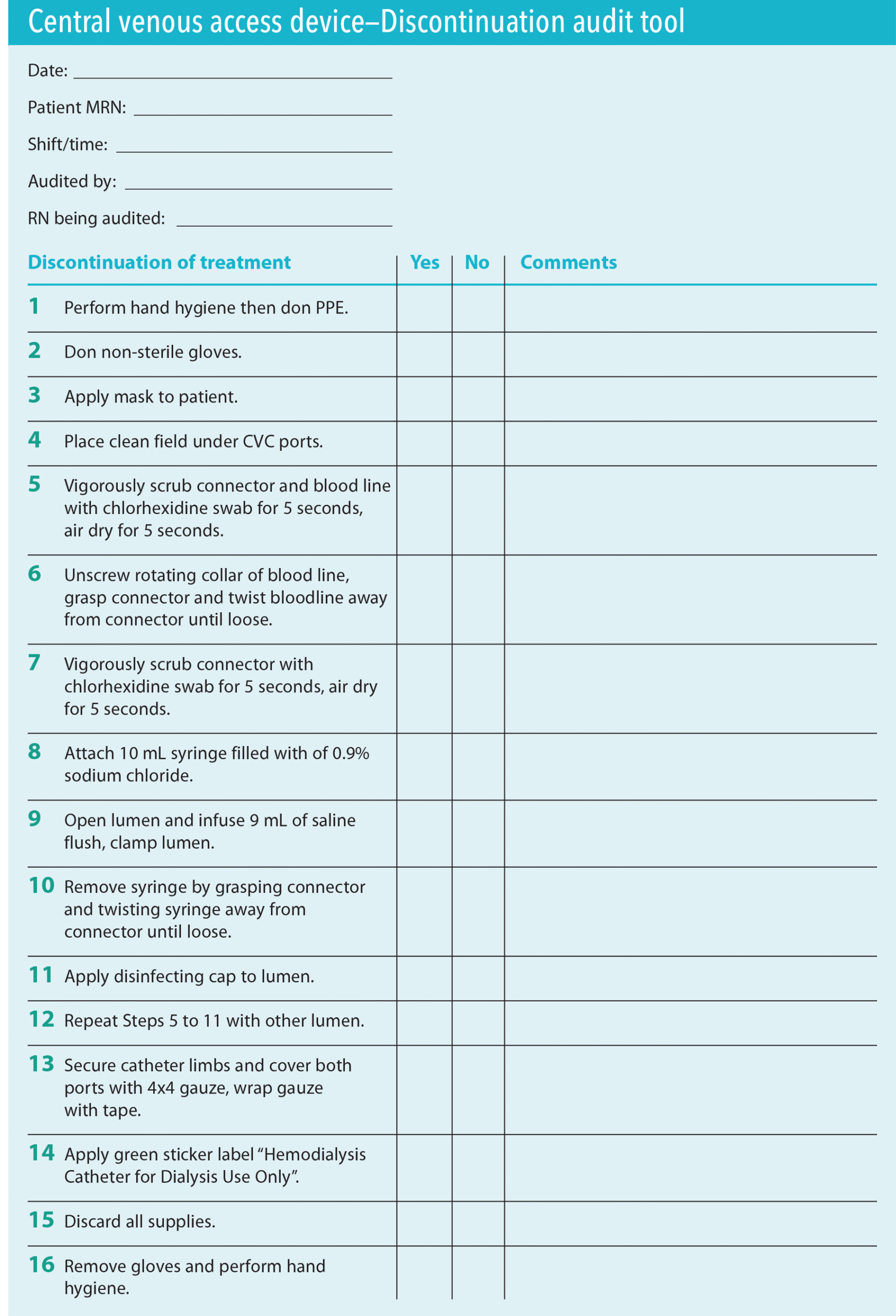
Discontinuation of hemodialysis with a CVC
- Perform hand hygiene and then don personal protective equipment (such as disposable gown and clean gloves).
- Place mask on yourself first and then the patient.
- Scrub the catheter hub and blood line with a CHG swab for 5 seconds and allow to air dry.
- Disconnect the blood line aseptically.
- Flush the line with 0.9 normal saline and then attach a disinfecting cap.
- Apply a gauze sleeve to cover both lumens.
Hemodialysis catheter exit site care
- Check for allergies (verify patient isn’t allergic to CHG).
- Perform hand hygiene and then don personal protective equipment (such as disposable gown and clean gloves).
- Place mask on yourself first and then the patient.
- Remove the old dressing and assess the exit site for signs and symptoms of infection.
- Remove dirty gloves and perform hand hygiene.
- Apply sterile gloves.
- Vigorously clean the exit site with an alcohol swab; repeat the procedure two more times with separate swabs each time.
- Vigorously clean the exit site with a CHG swab stick and then allow to air dry.
- Apply the CHG gel dressing aseptically.
- Secure the catheter to the patient; label the dressing with the date and RN initials.
- Remove gloves and perform hand hygiene.
Initiating and discontinuing treatment
Steps involved in initiating and discontinuing treatment include drawing the privacy or cubicle curtain, hand hygiene, and scrubbing the hemodialysis catheter hub with chlorhexidine gluconate (CHG) swabs for 5 seconds and allowing it to air dry during each access and de-access. RNs place a Food and Drug Administration-approved, needle-free, closed connector system at the initiation of each treatment and close it with a disinfecting cap upon completion. The device prohibits microbial entry.
RNs use a gauze sleeve to cover both lumens and place a neon green sticker on top of the sleeve labeled, “FOR HD [hemodialysis] USE ONLY.” Typically, nephrology RNs perform the sterile dressing change every 7 days and as deemed necessary (for example, if the dressing is wet, loose, soiled, or not intact).
Assessments and rounding
The standard of practice for patients receiving hemodialysis via a CVC includes a daily visual and tactile assessment of the insertion site, dressing, closed connector system, and disinfecting cap. Nephrology RNs assess for pain, tenderness, edema, redness, purulent drainage, malposition, migration, and obstructed or kinked tubing. To ensure thorough assessment, the CLABSI prevention team developed a checklist. RNs escalate abnormal findings to the nephrologists, primary medical–surgical RN, and nephrology nurse leaders. If necessary, they report clinical findings to the infection prevention team.
The nephrology nursing team developed a novel approach for proactive rounding assessments during non-dialysis days. Nephrology nurse leaders review the daily schedule of patients for hemodialysis treatment (typically 10 to 12) and create a list of those with CVC access for catheter rounding. They then provide that list for the nephrology RN assigned to conduct rounding that day.
Common assessment findings during non-dialysis days include loose dressings, skin irritation, and exit sites with drainage. The nephrology RNs document their assessments in the electronic health record (EHR) and escalate any non-tunneled catheter in place for more than 7 days to the nephrology provider for a line change or catheter removal.
CHG bathing
To reduce bacteria on the skin, all patients with a hemodialysis catheter receive daily CHG wipe baths (chest, abdomen, upper and lower extremities, back, and buttocks). CHG bathing is linked to significant reductions in infections caused by gram-positive pathogens. A study by Scheier and colleagues showed a decline in CLABSI incidence in ICUs that implemented daily CHG bathing.
In addition to documenting CHG baths in the EHR, nurses also note them in the infection prevention CHG bath report, which provides vital information about the completion of baths in the last 24 hours and aids practice sustainment. All clinicians and leaders can access the auto-generated report. Hemodialysis patients without a CHG bathing order won’t appear on the report; nurses escalate these cases to the primary provider so an order can be placed.
Ongoing instruction and observation
Nephrology nurse leaders reinforce the multi-targeted approach via daily briefs, huddles, and staff meetings to improve and enhance nurses’ knowledge of infection prevention practices and central venous access care and maintenance. In turn, the RNs provide patient education. Tools for staff education include the clinical practice guidelines for catheter care embedded in the EHR as well as audit tools and checklists designed to ensure consistent adherence to guidelines, policies, and procedures. (See Audit Tools)
During implementation of the new approach, nephrology nurse leaders performed 10 observations per month (the standard recommendation from hospital quality management) to assess protocol adherence. These observations allowed nurse leaders to provide real-time feedback while reinforcing evidence-based practices. In addition, clinical RNs engaged in real-time peer-to-peer monitoring and feedback. After rounding, the assigned nephrology RN shared their findings with the patients’ primary RNs, who described them as learning opportunities and welcomed the teaching moment.
The data and results
Each day, the nephrology nurses track the number of CVCs and device days. The infection prevention team submits those numbers to the CDC’s National Healthcare Safety Network each month. In addition, clinical department managers and directors share monthly data with the clinical staff during unit meetings, nursing quality council meetings, and patient care services leadership meetings, as well as through the hospital performance improvement coordinating group. CLABSI data and direct observation by nephrology nurse leaders indicate that this process has helped improve staff adherence to key processes and increased understanding of trends and gaps in care.
At their monthly meeting, dialysis staff review the CLABSI multi-targeted approach, CVC rounding, CLABSI data, and improvement opportunities. Staff members share ideas, suggestions, and challenges in sustaining strict adherence to the CDC’s core interventions. These reviews have helped team members gain a deeper understanding of the importance of hardwiring the interventions and maintaining these infection prevention efforts.
The hospital reported zero CLABSIs for 7 consecutive months (June 2019 through December 2019) after implementation of the multi-targeted approach. This significant reduction continued in 2020 and 2021 with no hemodialysis catheter-related CLABSIs. So far in 2025, one case of CLABSI has occurred. These results have led to substantial cost savings of $384,864 related to treating infections. Additional cost reductions occurred as a result of decreased lengths of stay. The CDC estimates an additional savings of $48,108 per CLABSI case, above and beyond the cost associated with an inpatient stay for a similar patient without a CLABSI.
The challenges
Although proactive rounding proved beneficial, it also created team stress. Initially, some clinical staff voiced reluctance due to additional rounding work, which averaged 2 hours per day and resulted in staff overtime of approximately 0.32 FTE. Ultimately, the practice change incurred additional costs of $9,400 annually related to CVC supplies needed for more frequent dressing changes requested by nephrology RNs.
Understanding and addressing the causes of resistance, communicating the importance of the practice change, and engaging clinical staff in the process created a more receptive environment. The CLABSI prevention team initiated various strategies to acknowledge staff efforts and address stress, such as reward and recognition points, real-time feedback, a kudos board, and staff wellness programs.
Nephrology RNs encountered difficulty assessing patients due to scheduled tests and procedures. To avoid conflict with catheter rounding, the nephrology RNs communicated directly with primary RNs about test and procedure scheduling.
Early phases of implementation presented challenges with adherence to CHG bathing, primarily due to lack of provider orders. To address this barrier to success, the infection prevention team reviewed the CHG bath report daily for missing orders. Escalating the missing bath order to providers increased awareness and adherence to placing CHG bath orders for every patient receiving hemodialysis.
A supportive workplace culture, clear and inclusive communication, and a reliable feedback loop helped identify areas for improvement and ultimately resulted in positive outcomes, including zero CLABSIs and staff and leader engagement in the project.
Next steps
In 2025, to hardwire evidence-based CLABSI prevention practices for all patients with CVCs, the team created a multidisciplinary CLABSI champion program, with frontline clinical RNs serving as resources for colleagues and peers as they develop expertise and participate in or lead QI projects on their units. In addition, the organization’s annual mandatory RN skills fair will now include the multi-targeted CLABSI prevention approach.
Review of the correlation of the three novel strategies (proactive daily catheter rounding, cubicle curtain for patient safety, and visual cue “FOR HD USE ONLY”) with heightening situational awareness of clinicians will help the CLABSI prevention team better understand the impact on infection prevention practices specific to the hemodialysis population.
Positive impact
Despite prevention efforts, risk of CLABSI among patients receiving hemodialysis remains a concern. This performance improvement project demonstrated the positive impact of a dedicated and engaged team, effective leadership, timely feedback, and a multi-targeted approach to achieving success.
The authors work at North Shore University Hospital in Manhasset, New York. Elena Memoracion is senior director of patient care. Janis Paulose is assistant manager. Maria Bernal is a nurse manager.
American Nurse Journal. 2025; 20(8). Doi: 10.51256/ANJ082520
References
American Society of Nephrology. Nephrologists Transforming Dialysis Safety (NTDS). epc.asn-online.org/projects/ntds/
Centers for Disease Control and Prevention. CDC approach to BSI prevention in dialysis facilities. cdc.gov/dialysis-safety/media/pdfs/Dialysis-Core-Interventions-P.pdf
Centers for Disease Control and Prevention. Current HAI progress report. November 25, 2024. cdc.gov/hai/data/portal/progress-report.html
Centers for Disease Control and Prevention. Intravascular catheter-related infection (BSI) prevention guidelines. April 12, 2024. cdc.gov/infection-control/hcp/intravascular-catheter-related-infection/index.html
Centers for Disease Control and Prevention. Making Dialysis Safer for Patients Coalition. March 29, 2024. cdc.gov/dialysis-safety/making-dialysis-safer-coalition/index.html
Chapman L, Hargett L, Anderson T, Galluzzo J, Zimand P. Chlorhexidine gluconate bathing program to reduce health care–associated infections in both critically ill and non–critically ill patients. Crit Care Nurse. 2021;41(5):e1-8. doi:10.4037/ccn2021340
Darma Siahaan B, Widodo Wardana A. Hemodialysis central-line associated bloodstream infection: Incidence, risk factor, and antibiogram. Ind J Kidney Hyper. 2020;3(1):9-17. doi:10.32867/inakidney.v3i1.26
Fisher M, Golestaneh L, Allon M, Abreo K, Mokrzycki MH. Prevention of bloodstream infections in patients undergoing hemodialysis. Clin J Am Soc Nephrol. 2020;15(1):132-51. doi:10.2215/CJN.06820619
Hamid HA, Hicham B, Ibrahim A, et al. Effective prevention bundle to eliminate catheter-related bloodstream infections in ambulatory hemodialysis patients. Can J Infect Control. 2019;34(1):54-7. doi:10.36584/CJIC.2019.007
Johansen KL, Gilbertson DT, Li S, et al. US renal data system 2023 annual data report: Epidemiology of kidney disease in the United States. Am J Kidney Dis. 2024;83(4):A8-13. doi:10.1053/j.ajkd.2024.01.001
Khalifa ME, Omar TK, El-Gendy FM, Ahmed HM, Saad AA. Effect of nursing care bundle on nurse’s performance regarding central venous line-associated blood stream infection. Int Egyp J Nurs Sci Res. 2022;3(1):554-70. doi:10.21608/ejnsr.2022.247238
Parker SH, Jesso MN, Wolf LD, et al. Human factors contributing to infection prevention in outpatient hemodialysis centers: A mixed methods study. Am J Kidney Dis. 2024;84(1):18-27. doi:10.1053/j.ajkd.2023.12.024
Pitiriga V, Kanellopoulos P, Bakalis I, et al. Central venous catheter–related bloodstream infections and colonization: The impact of insertion site and distribution of multidrug-resistant pathogens. Antimicrob Resist Infect Control. 2020;9(1):189. doi:10.1186/s13756-020-00851-1
Poinen K, Quinn RR, Clarke A, et al. Complications from tunneled hemodialysis catheters: A Canadian observational cohort study. Am J Kidney Dis. 2019;73(4):467-75. doi:10.1053/j.ajkd.2018.10.014
Rha B, See I, Dunham L, et al. Vital Signs: Health disparities in hemodialysis-associated Staphylococcus aureus bloodstream infections—United States, 2017–2020. Morb Mortal Wkly Rep. 2023;72(6):153-9. doi:10.15585/mmwr.mm7206e1
Roderman N, Moore K, Wilcox S, Jellerson J, Bridges Z. Central line-associated bloodstream infection reduction in hemodialysis patients across 9 hospitals and 3 states. Healthc J Med. 2024; 5(5):551-8. doi: 10.36518/2689-0216.1910
Sahli F, Feidjel R, Laalaoui R. Hemodialysis catheter-related infection: Rates, risk factors and pathogens. J Infect Public Health. 2017;10(4):403-8. doi:10.1016/j.jiph.2016.06.008
Scheier T, Saleschus D, Dunic M, et al. Implementation of daily chlorhexidine bathing in intensive care units for a reduction of central line-associated blood stream infections. J Hosp Infect. 2021;110;26-32. doi:10.1016/j.jhin.2021.01.007
Shalaby MM, Eshra KA, Essa RA, Alghazaly GM. A study of central line associated bloodstream infections among patients on hemodialysis before and after implementation of a catheter bundle. Univers J Microbiol Res. 2018;6(1):1-6.
Sohail MA, Vachharajani TJ, Anvari E. Central venous catheters for hemodialysis—The myth and the evidence. Kidney Int Rep. 2021;6(12):2958-68. doi:10.1016/j.ekir.2021.09.009
U.S. Renal Data System. Vascular access. 2023. usrds-adr.niddk.nih.gov/2023/end-stage-renal-disease/4-vascular-access
Wang L, Jia L, Jiang A. Pathology of catheter-related complications: What we need to know and what should be discovered. J Int Med Res. 2022;50(10):3000605221127890. doi:10.1177/03000605221127890
Wooten R, Kothari D, Pryor R, Bearman G. Preventing hemodialysis catheter-related bloodstream infections: barriers, controversies, and best practices. Curr Infect Dis Rep. 2022;24:21-7. doi:10.1007/s11908-022-00773-6
Key words: hemodialysis catheter, bloodstream infections



















{kind=link}
{kind=link}
1 Comment. Leave new
Do you have a reference for placing the gauze sleeve on each port? This has been a hot topic within our facilities.