
Rely on interprofessional collaboration, follow the evidence.
- Acute kidney injury (AKI) is a common condition affecting hospitalized patients, particularly those who are critically ill.
- Monitoring serum creatinine, estimated glomerular filtration rate, and urine output is essential to AKI management.
- Prompt treatment of AKI aids in preventing life-threatening complications.
Learning Objectives
- Explain causes and pathophysiology of acute kidney injury (AKI).
- Describe pre-renal, intra-renal, and post-renal AKI and AKI staging.
- Discuss nursing interventions in interdisciplinary collaborative management that can impact patient outcomes.
The author, planners, and peer reviewers of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity.
Acute kidney injury: Causes, phases, and early detection
Stemming the rising tide of acute kidney injury
Expiration: 6/1/26
Kay Dempsey,* a 70-year-old woman, arrives by ambulance at the emergency department (ED) after being found lethargic, pale, and diaphoretic in the nursing home where she lives. Her medical history includes hypertension, hyperlipidemia, type 2 diabetes, heart failure (HF), and kidney stones. On admission, her vital signs are blood pressure (BP) 86/40 mmHg, heart rate (HR) 136 beats per minute (bpm), respiratory rate (RR) 30 breaths per minute, oxygen saturation 94% on 6 L of oxygen by nasal cannula, and temperature 101.4 F (38.5 C). In addition, she has +1 edema of her lower extremities.
Abnormal findings from Ms. Dempseys initial basic metabolic panel (BMP) include blood urea nitrogen (BUN) 35 mg/dL (normal: 823 mg/dL), serum creatinine (SCr) 1.6 mg/dL (normal: 0.61.2 mg/dL), potassium 5.2 mEq/L (normal: 3.55 mEq/L), and glucose 224 mg/dL (normal: 70110 mg/dL).
Notable findings from the complete blood count (CBC) upon admission include white blood cells 24,000/mm3 (normal: 4,50011,000/mm3), hemoglobin 10 g/dL (normal: 1214 g/dL), and hematocrit 30% (normal: 3644%). Arterial blood gasses show that Ms. Dempseys are pH 7.30 (normal: 7.357.45), PaO2 116 mmHg (normal: 80100 mmHg), PaCO2 30 mmHg (normal: 3545 mmHg), and HCO3 16 mEq/L (normal: 2226 mEq/L). Her serum lactate is 5.4 mmol/L (normal: 0.62.2 mmol/L).
In the ambulance, Ms. Dempsey received a 500 mL bolus of 0.9% normal saline without improvement in her vital signs. A physical exam in the ED reveals a weeping Stage 4 sacral pressure injury. Following sepsis protocol, the ED physician initiates 30 mL/kg of normal saline and consulted the intensivist.
Understanding kidney injury
The renal system comprises the kidneys, ureters, and urethra, which maintain homeostasis via filtration and excretion of waste products, participate in acidbase balance, produce renin for maintaining hemodynamics, and produce erythropoietin to stimulate red blood cell production. Insult to this system can result in electrolyte derangements, increased risk of stroke, long-term renal failure, or death. Kidney failure is broadly classified as either acute or chronic (chronic kidney disease [CKD]). This article focuses on acute kidney injury AKI. (See AKI by the numbers.)
AKI by the numbers
Worldwide, an estimated 1 in 5 adults and 1 in 3 children may experience AKI during hospitalization. The prevalence can be as high as 50% among patients in the intensive care unit, with mortality rates as high as 80% among those who require renal replacement therapy. AKI can increase cost of care over two-fold, depending on severity of disease, as a result of increased length of stay and costly interventions, such as dialysis.
AKI, a subset of acute kidney disease (AKD), is characterized by a sudden decrease in renal function, which develops over a few hours or several days. It can lead to significant increases in creatinine and reductions in urine output. Practice guidelines developed by the Kidney Disease Improving Global Outcomes (KDIGO) workgroup defines AKI as meeting any of the following criteria:
- Increase in SCr by 0.3 mg/dL or more within 48 hours
- Increase in SCr to 1.5 times baseline or more, which is known or presumed to have occurred within the past 7 days
- Urine output less than 0.5 mL/kg/hour for 6 hours
These criteria rely on monitoring the patients creatinine and accurately measuring urine output of at-risk patients, including older adults, who have lower baseline renal function as measured by the glomerular filtration rate (GFR). Other risk factors include hypertension, diabetes, heart failure, cardiovascular disease, and liver disease. Use of nephrotoxic agentssuch as antibiotics, non-steroidal anti-inflammatory drugs (NSAIDs), and radiocontrast dyesalso increase AKI risk.
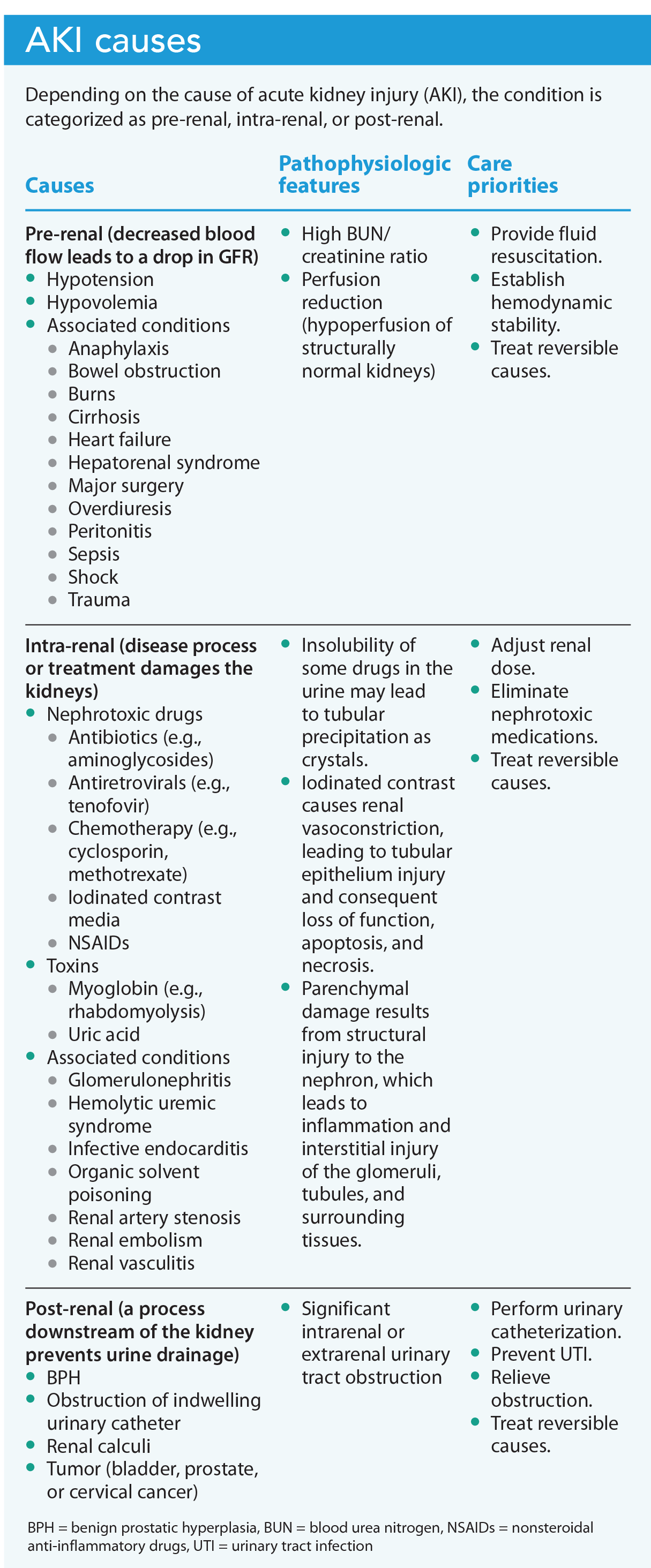
Causes and pathophysiology
Susceptibility to AKI increases in the presence of combinations of exposures, risk factors, and comorbidities. For example, an older adult diagnosed with sepsis who has a history of diabetes and experiences volume depletion is at increased risk for AKI. When admitting at-risk patients, providers should conduct risk assessments that target interventions to address reversible causes of AKI. (See AKI causes.)
Intraoperative hypotension (mean BP less than 60 mmHg for at least 10 minutes) among noncardiac surgery patients is associated with an increased risk for postoperative AKI. In addition, AKI is more common among patients with a history of CKD, a body mass index >32 kg/m2, and a GFR <60 mL/minute.
The intensivist evaluates Ms. Dempsey in the ED, where a comprehensive physical exam, including a bedside ultrasound of various organs, is performed. Bibasilar mild consolidation are noted on the lung ultrasound. The abdominal and renal ultrasound rule out post-renal causes and bowel obstructions. The intensivist orders the patient transferred to the medical intensive care unit (MICU) for further evaluation and treatment.
The provider determines urosepsis as the most likely cause of Ms. Dempseys AKI. He orders two sets of blood cultures, urine and sputum cultures, and a wound culture and sensitivity. After an infectious disease consult, the provider orders an empiric I.V. antibiotic regimen of piperacillin/tazobactam. (See Gerontologic considerations.)
Manifestations
Unlike myocardial infarction (MI) or stroke, which frequently have immediate signs such as chest pain or hemiparesis, respectively, AKI signs are nonspecific or occur later because of downstream effects that take time to manifest. These signs include fluid overload (which presents as edema, most noticeably in the lower extremities), electrolyte imbalances (such as hyperkalemia and hyperphosphatemia, which may cause nausea and vomiting), generalized weakness, and ECG abnormalities (such as peaked T waves, heart blocks, and ventricular tachycardia).
Urea accumulation in patients with AKI can lead to metabolic encephalopathy, which may manifest as altered mental status, seizures, and coma. In patients who exhibit these signs and symptoms as a direct result of AKI, mortality and morbidity rates are high. Theyll require renal replacement therapy and multimodal symptom management.
On her first MICU day, Ms. Dempsey remains lethargic. She maintains adequate ventilation and continues to receive 4 L of oxygen via nasal cannula with 96% O2 saturation. In anticipation of septic shock, the intensivist orders a multilumen central venous catheter inserted via the right internal jugular vein. Urinalysis indicates the presence of nitrites, leukocyte esterase, and large amounts of white blood cells and bacteria.
Repeat BUN and SCr are 38 mg/dL and 1.8 mg/dL, respectively, an increase from baseline. Ms. Dempseys BMP is significant for increasing potassium (5.8 mEq/L) and phosphorus (5.3 mg/dL). A 12-lead ECG reveals peaked T-waves and a PR interval of 0.24 seconds (normal: 0.12 to 0.20 seconds). The provider orders 10 units of regular insulin I.V. push, 1 ampule of 50% dextrose I.V. push, and 10 g of oral sodium zirconium cyclosilicate. After 4 hours, Ms. Dempseys potassium is 5.3 mEq/L, and a repeat ECG shows a PR interval of 0.18 seconds and peaked T waves with less amplitude. The ECG changes signify resolution of the first-degree AV block and a return to baseline of T-waves as the serum potassium moves closer to the normal range.
Gerontologic considerations
Physiologic renal changes associated with aging include the following:
- reduced kidney size and weight
- lower glomerular filtration rate
- glomerulosclerosis
- decreased sodium reabsorption and potassium excretion
- reduced ability to concentrate urine
With the overall reduction in physiologic reserves, older adults have a higher risk for acute kidney injury. Complications associated with kidney disease, such as cardiovascular disease, contribute to decreased quality of life, frailty, higher care costs, and increased mortality.
Therapeutic implications include ensuring the following:
- adequate hydration
- effective management of comorbidities such as diabetes and hypertension to reduce renal damage
- close monitoring of serum creatinine levels and urine output
- comprehensive geriatric assessment
Diagnosis
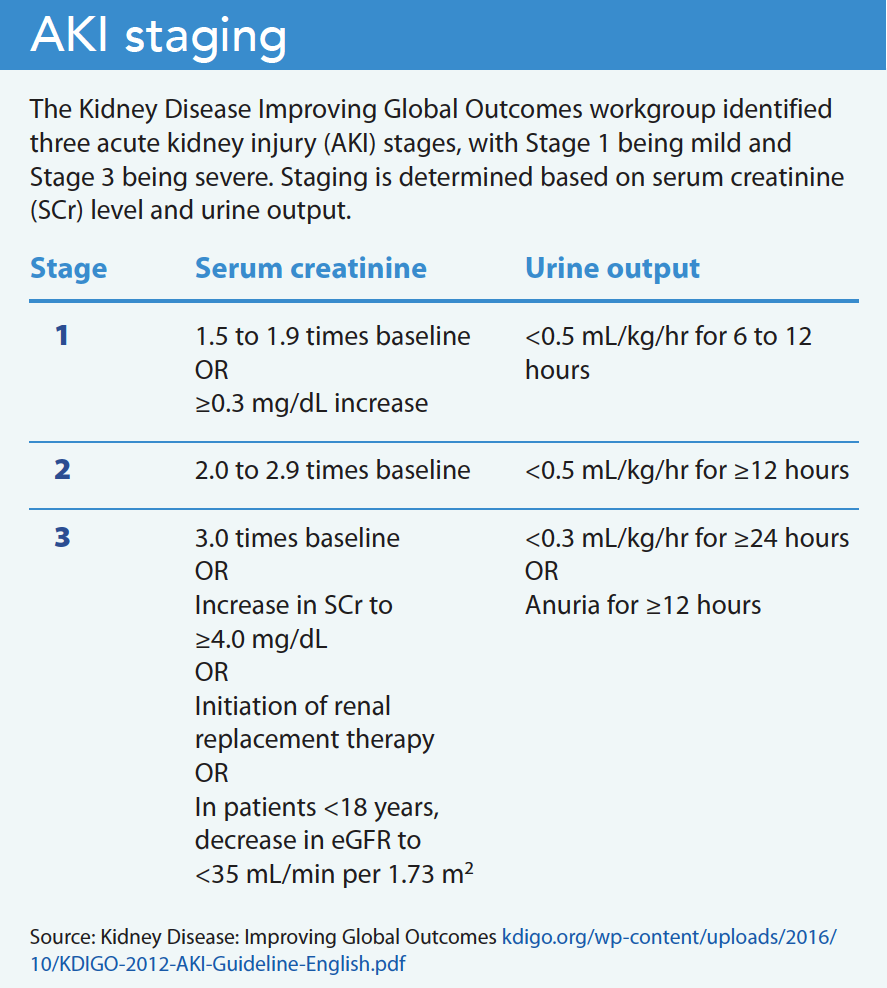
The KDIGO workgroup identified three stages of AKI from Stage 1 (mild) to Stage 3 (the most severe). The AKI stage serves as a predictor of mortality, and the guidelines recommend staging patients according to the criteria with the highest stage. For example, if SCr is at Stage 3 and urine output is at Stage 2, the patient should be staged at Stage 3 based on SCr. (See AKI staging.)
Because renal and non-renal factors can influence SCr, staging criteria have limitations. For example, SCr measurements may be confounded by outside factors such as diuretic use, creatine supplementation, variable volumes of distribution in different patients, and altered creatinine production. Differentiating between chronic kidney injury and AKI without a baseline for the individual patient can prove difficult.
In addition to monitoring SCr, BUN, electrolytes, CBC, and urinalysis, providers may order imaging procedures based on the suspected cause of AKI. For example, the provider may order a kidney ultrasound to rule out urinary tract obstruction or structural abnormalities.
The provider orders a daily BMP and CBC but decides against any imaging procedures requiring an iodinated contrast to prevent exacerbating AKI with a nephrotoxic substance. The patients central venous pressure ranges from 14 to 18 mmHg (normal: 812 mmHg). A chest x-ray indicates bilateral infiltrates, and an echocardiogram shows an ejection fraction of 30%.
Novel biomarkers
To aid CKD diagnosis, Inker and colleagues recommend using cystatin C levels to estimate GFR or in confirmatory testing for eGFR. Cystatin C is a protein produced by nucleated cells and eliminated by the kidneys. Its processed similarly to SCr, but is less dependent on muscle mass and isnt affected by race, which allows for more accurate GFR estimation. In critically ill patients, cystatin C has been shown to detect AKI 1 to 2 days before an increase in SCr. An increased cystatin C level indicates reduced GFR. Normal cystatin C values vary according to the lab and assay manufacturer, so note lab reference values.
Contrast-induced AKI
Providers make a diagnosis of contrast-induced AKI (CI-AKI) based on various values. For example, theyll diagnose CI-AKI if the patient experiences increased SCr of 0.5 mg/dL or a 25% increase from baseline within 7 days after exposure to contrast medium, increased plasma creatinine level by at least 0.3 mg/dL over baseline within 48 hours after exposure, or urinary output of less than 0.5 mL per kg of body weight per hour that persists for at least 6 hours after exposure.
Collaborative management
AKI management requires interdisciplinary collaboration aimed at making renal dose adjustments, providing hemodynamic support, avoiding nephrotoxic medications, and preventing hyperglycemia. Nurses play a vital role in this care, as well as in managing continuous renal replacement therapy (CRRT).
Renal dose adjustment
Based on the severity of kidney dysfunction, many renally cleared medications require serum-level checks, as well as dosage and frequency reviews and adjustments based on creatinine clearance or eGFR. Nurses must monitor for signs of drug toxicity among patients with AKI, especially those prescribed medications with a narrow therapeutic range, such as digitalis and antibiotics. (See GFR estimation.)
Hemodynamic support
To prevent AKI resulting from hypotension and shock, hemodynamic monitoring can include checking cardiac filling pressures. Providers may order volume expansion with normal saline, particularly for patients at increased risk for CI-AKI. KIDGO recommends avoiding diuretics to treat AKI, except when managing volume overload. Hourly urine output monitoring is essential for critically ill patients. The theoretical advantage of urine output monitoring over SCr monitoring is the speed of the response. For example, if GFR suddenly falls to zero, an SCr increase wouldnt be detected for several hours; however, urine output would be affected immediately.
Patients with pre-renal AKI require adequate volume and perfusion pressure. If the patient is in shock, the provider may order vasopressors. Concern that normal saline may result in hyperchloremic acidosis and increase AKI risk (or worsen existing AKI), has resulted in use of balanced salt solutions (crystalloids with a chloride concentration closer to that in human plasma). Henninger and colleagues found that, among ICU patients with sepsis, the incidences of AKI didnt differ when using either lactated Ringers solution or normal saline for fluid resuscitation. When initiating fluid resuscitation, nurses should consider the patients comorbidities; contraindications for both normal saline and lactated Ringers solutions exist but are outside the scope of this article.
Nephrotoxic medication avoidance
Nephrotoxic drugs play a role in 20% to 30% of AKI cases. On admission, nurses should obtain a full list of the patients medications, including nonprescription drugs and herbal supplements. Prescribers should always check each prescription for renal adverse effects. For example, controversy exists around the use of vitamin C in the treatment of sepsis; evidence indicates that high doses of vitamin C can lead to AKI in these patients.
Providers should avoid procedures that require iodinated radiocontrast in patients at risk for AKI. Routine administration of acetylcysteine isnt recommended to prevent AKI or long-term adverse events after angiographic procedures. Nurses should monitor SCr and urine output for all patients who have a radiocontrast procedure. Periprocedural use of normal saline has been shown to prevent CI-AKI, although the optimal volume isnt known. The American College of Radiology guidelines on the administration of contrast media recommend isotonic saline at a rate of 100 mL per hour for 6 to 12 hours before angiography and 4 to 12 hours after angiography. After angiography, nurses should monitor patients for signs of pulmonary edema. All clinicians should know the eGFR thresholds below which antibiotic, contrast medium, chemotherapy, and other agents shouldnt be used or their doses adjusted.
Hyperglycemia prevention
Acute or critical illness can cause stress hyperglycemia as a result of insulin resistance and anxiety response. Uncontrolled hyperglycemia is associated with increased incidences of AKI in patients with MI. The KDIGO workgroup recommends insulin therapy with a target plasma glucose of 110 to 149 mg/dL in critically ill patients. To avoid hypoglycemia, nurses should frequently monitor the blood glucose of patients at risk for AKI and those on insulin therapy. A study by Marenzi and colleagues has shown that in patients with diabetes experiencing an acute MI, AKI is better predicted by the combined evaluation of acute and chronic glycemic values. This means that clinicians also should check A1C levels.
On Day 2 in the MICU, Ms. Dempsey develops hypotension (BP 8892/5054 mmHg) with an HR of 100 to 120 bpm and sinus tachycardia, even after a 2-liter normal saline bolus. Shes electively intubated, which reduces her BP to as low as 52/28 mmHg. The provider orders norepinephrine at 5 mcg/minute, which is titrated up to 20 mcg/minute. A mean arterial pressure of 6268 mmHg is achieved. To facilitate ventilator adherence, the provider orders I.V. fentanyl and propofol.
The nurse inserts a nasogastric tube and an indwelling urinary catheter. Ms. Dempseys hourly urine output is 10 to 15 mL/hour for the next 5 hours. A nutrition consult is requested to optimize the patients nutrition while minimizing electrolyte imbalance. The consult results in Ms. Dempsey receiving a diet low in protein, sodium, potassium, and phosphorous. The patients blood cultures grow Escherichia coli, so the provider orders continuation of I.V. piperacillin/tazobactam and adds I.V. meropenem.
For critically ill patients with AKI, nurses should conduct daily and periodic eGFR checks to monitor disease progression and treatment response. Even after an apparent resolution of AKI, long-term risks exist for CVD (especially HF) and CKD.
Continuous renal replacement therapy
If a patient with AKI becomes anuric and shows signs of a prolonged inability to clear electrolytes and waste (for example, refractory hyperkalemia, severe metabolic acidosis, and metabolic encephalopathy), they meet the criteria for renal replacement therapy, which may include intermittent hemodialysis (IHD) and CRRT. Providers may opt for CRRT over IHD for patients who are hypotensive and cant tolerate the large shifts in volume.
CRRT for patients with severe AKI due to sepsis has the added benefit of removing endotoxins and cytokines (such as interleukins) and tumor necrosis factor alpha, which have a direct correlation with mortality. The electrolyte composition of the therapy fluid is tailored to the patients electrolyte panel, so nurses should draw serial metabolic panels. The nurses role also includes maintaining asepsis to prevent central line-associated bloodstream infection.
Over the next 12 hours, Ms. Dempseys metabolic acidosis worsens, her serum lactate increases to 10.2 mmol/L, she has persistent hyperkalemia up to 6.0 mEq/L, and shes unresponsive to medical treatment. The patients hemodynamic instability prompts the provider to order CRRT, which Ms. Dempsey tolerates well. After 12 hours of uninterrupted therapy, her vasopressor requirements decrease, and her metabolic acidosis improvesserum lactate falls to 5.8 mmol/L and potassium to 5.4 mEq/L; however, urine output remains <10 mL/hour.
After 2 weeks in the MICU, Ms. Dempsey recovers from sepsis and the provider orders extubation. She completes 48 hours of CCRT and is weaned off of norepinephrine. Her serum lactate drops to 2.0 mmol/L, and her potassium returns to normal. At the time of transfer to a stepdown unit, Ms. Dempseys urine output is 0.5 mL/kg/hour and her SCr is 1.3 mg/dL.
Apply the best evidence
AKI is common in hospitalized patients, especially those who are critically ill. Nurses play an integral role in applying the best evidence in the screening, management, and prevention of AKI.
*Name is fictitious.
Fidelindo Lim is a clinical associate professor at New York University Rory Meyers College of Nursing in New York, New York. Allen Li is a staff nurse in the medical intensive care unit at Mount Sinai Hospital in New York, New York.
American Nurse Journal. 2023; 18(6). Doi: 10.51256/ANJ062306
References
American College of Radiology. ACR Manual on Contrast Media. 2023. acr.org/-/media/acr/files/clinical-resources/contrast_media.pdf
Benoit SW, Ciccia EA, Devarajan P. Cystatin C as a biomarker of chronic kidney disease: latest developments. Expert Rev Mol Diagn. 2020;20(10):1019-26. doi:10.1080/14737159.2020.1768849
Birkelo BC, Pannu N, Siew ED. Overview of diagnostic criteria and epidemiology of acute kidney injury and acute kidney disease in the critically ill patient. Clin J Am Soc Nephrol.2022;17(5):717-35. doi:10.2215/CJN.14181021
Collister D, Pannu N, Ye F, et al. Health care costs associated with AKI. Clin J Am Soc Nephrol. 2017;12(11):1733-43. doi:10.2215/cjn.00950117
Davison E, Affleck A, Daratha KB. Intraoperative hypotension and acute kidney injury in non-cardiac surgery at a large tertiary care medical center. AANA J. 2022;90(1):58-63.
Finfer S, Micallef S, Hammond N, et al. Balanced multielectrolyte solution versus saline in critically ill adults. New Engl J Med. 2022;386(9):815-26. doi:10.1056/nejmoa2114464
Gameiro J, Fonseca JA, Outerelo C, Lopes JA. Acute kidney injury: From diagnosis to prevention and treatment strategies. J Clin Med. 2020;9(6):1704. doi:10.3390/jcm9061704
Griffin BR, Faubel S, Edelstein CL. Biomarkers of drug-induced kidney toxicity. Ther Drug Monit. 2019;41(2):213-26. doi:10.1097/FTD.0000000000000589
Henninger M, Fiorenza M, Feroz A. Lactated ringer versus normal saline in critically patients: Incidence of acute kidney injury. Crit Care Med. 2020;48(1):723. doi:10.1097/01.ccm.0000645888.86937.bf
Igiraneza G, Ndayishimiye B, Nkeshimana M, Dusabejambo V, Ogbuagu O. Clinical profile and outcome of patients with acute kidney injury requiring hemodialysis: Two years experience at a tertiary hospital in Rwanda. Biomed Res Int. 2018;2018:1716420. doi:10.1155/2018/1716420
Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737-49. doi:10.1056/NEJMoa2102953
Karkar A, Ronco C. Prescription of CRRT: A pathway to optimize therapy. Ann Intensive Care. 2020;10(1):32. doi:10.1186/s13613-020-0648-y
Kidney Disease: Improving Global Outcomes (KDIGO). Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. 2012;2(suppl):1-138. kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-AKI-Guideline-English.pdf
Legrand M, Rossignol P. Cardiovascular consequences of acute kidney injury. N Engl J Med. 2020;382(23):2238-47. doi:10.1056/NEJMra1916393
Levey AS, Grams ME, Inker LA. Uses of GFR and albuminuria level in acute and chronic kidney disease. N Engl J Med. 2022;386(22):2120-8. doi:10.1056/NEJMra2201153
Marenzi G, Cosentino N, Milazzo V, et al. Acute kidney injury in diabetic patients with acute myocardial infarction: Role of acute and chronic glycemia. J Am Heart Assoc. 2018;7(8):e008122. doi:10.1161/JAHA.117.008122
Matsue Y, van der Meer P, Damman K, et al. Blood urea nitrogen-to-creatinine ratio in the general population and in patients with acute heart failure. Heart. 2017;103(6):407-13. doi:10.1136/heartjnl-2016-310112
McCune TR, Toepp AJ, Sheehan BE, Sherani MSK, Petr ST, Dodani S. High dose intravenous vitamin C treatment in sepsis: Associations with acute kidney injury and mortality. BMC Nephrol. 2021;22(1):387. doi:10.1186/s12882-021-02599-1
Meeusen JW, Kasozi RN, Larson TS, Lieske JC. Clinical impact of the refit CKD-EPI 2021 creatinine-based eGFR equation. Clin Chem. 2022;68(4):534-9. doi:10.1093/clinchem/hvab282
Mehran R, Dangas GD, Weisbord SD. Contrast-associated acute kidney injury. N Engl J Med. 2019;380(22):2146-55. doi:10.1056/NEJMra1805256
Mohsenin V. Practical approach to detection and management of acute kidney injury in critically ill patient. J Intensive Care. 2017;5:57. doi:10.1186/s40560-017-0251-y
National Kidney Foundation. GFR. kidney.org/kidneydisease/siemens_hcp_gfr
Ogobuiro I, Tuma F. Physiology, renal. StatPearls. 2023. ncbi.nlm.nih.gov/books/NBK538339/
Ostermann M, Randolph AG. Resuscitation fluid composition and acute kidney injury in critical illness. N Eng J Med. 2022;386(9):888-9. doi:10.1056/nejme2200294
OSullivan ED, Hughes J, Ferenbach DA. Renal aging: Causes and consequences. J Am Soc Nephrol. 2017;28(2):407-20. doi:10.1681/ASN.2015121308
Palacio-Lacambra ME, Comas-Reixach I, Blanco-Grau A, Su-Negre JM, Segarra-Medrano A, Montoro-Ronsano JB. Comparison of the Cockcroft-Gault, MDRD and CKD-EPI equations for estimating ganciclovir clearance. Br J Clin Pharmacol. 2018;84(9):2120-8. doi:10.1111/bcp.13647
Perazella MA, Rosner MH. Drug-induced acute kidney injury. Clin J Am Soc Nephrol. 2022;17(8):1220-33. doi:10.2215/CJN.11290821
Susantitaphong P, Cruz DN, Cerda J, et al. World incidence of AKI: A meta-analysis. Clin J Am Soc Nephrol. 2013;8(9):1482-93. doi:10.2215/CJN.00710113
Tandukar S, Palevsky PM. Continuous renal replacement therapy: Who, when, why, and how. Chest. 2019;155(3):626-38. doi:10.1016/j.chest.2018.09.004
Key words: acute kidney injury, AKI, acute kidney disease, renal failure, nephrology nursing

















2 Comments. Leave new
excellent information and review
Hello Beverly,
Thank you for reading and for your feedback!
Best wishes,
Fidel