
Careful patient selection, provider and patient education, and well-planned and delivered patient care are critical to success.
Takeaways:
- Home infusion therapy administration is associated with good outcomes but isn’t without risk as patients require an invasive device and must be monitored carefully for potential vascular access and infusion medication–related complications and adverse reactions.
- Home care organizations must provide an infusion therapy program that includes specialized nursing education including competency assessment; up-to-date, evidence-based policies and procedures; and outcome monitoring.
- Careful planning is essential during discharge planning as patients are transitioned from acute to home care; patient and/or caregiver ability to participate in care is a critical aspect of planning.
A combination of factors—aging population, increasing chronic illness incidence, costs of recurrent hospitalizations, and evolving reimbursement models—has led to a growth in home care. The overarching goals of home care are to maintain patients safely in the home setting and prevent hospitalizations. And for patients with compromised immune systems, home care can help them avoid exposure to infectious diseases.
Home infusion therapy (to deliver antimicrobials, hydration solutions, parenteral nutrition, antineoplastic drugs, analgesics, cardiac infusion therapies for heart failure, immunoglobulins, and other biologics and drugs) allows patients of all ages to be discharged earlier from the hospital or even avoid hospitalization altogether. Studies show that patient satisfaction with home infusion therapy is high, clinical outcomes are good, and patients are no more likely to suffer side effects or adverse reactions at home versus inpatient clinical settings.
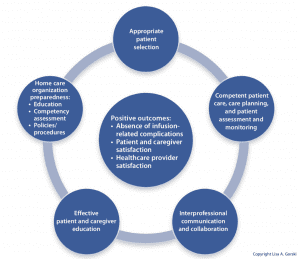
Home infusion therapy is a specialty within home care practice. My Model for Safe Home Infusion Therapy promotes positive outcomes—including the absence of complications and increased patient and healthcare provider satisfaction—when five key elements are addressed. (See A model for safety.)
The goals of the Model for Safe Home Infusion Therapy are to reduce complications and increase patient and healthcare provider satisfaction.
Home care organization preparedness
Some home care organizations and pharmacies specialize in home infusion, but many provide it as a smaller component of their overall program. Home care organizations shouldn’t accept patients for home infusion therapy unless the organizations have a sound program that includes specialized education; up-to-date, evidence-based policies and procedures; and documented infusion-related competencies. In accordance with the Infusion Therapy Standards of Practice, published by the Infusion Nurses Society (INS), competency should be assessed and validated before providing ongoing patient care. An infusion therapy program also should include infection reporting and surveillance and quality assessment and performance improvement.
When an organization is asked to provide infusion medications at home or infusions for which it is less prepared or lacks experience and procedures, it should investigate (in collaboration with the provider and pharmacist) the safety of the infusate, the risks (for example, drug reactions and home management), and the rationale for administration in the home versus in an outpatient clinical setting. Clinician education and preparation is required and patient safety is always a priority in such decision-making.
Home infusion therapy is generally associated with good outcomes, but it’s not without risk in the unmonitored home setting. Patients require an invasive device with a variety of potential complications, and some patients receive high-risk infusions such as antineoplastics, opioids, and inotropes. Even home I.V. antibiotic therapy can result in significant adverse events such as nephrotoxicity or ototoxicity, depending on the medication infused. Thorough preparation and care plan development are essential.
Although not common, lawsuits have been filed against home care organizations for issues such as failure to identify signs and symptoms of infection in patients with central venous access devices (CVAD), failure to monitor for and identify adverse drug reactions, and incorrect programming of electronic infusion pumps. Such failures in care have led to patients dying, losing limbs, and suffering other severe complications.
Appropriate patient selection
Inconsistent discharge planning from acute care to home care is a gap in the current healthcare system. Careful planning is critical for successful patient transition to the home setting, and patients and their caregivers must take responsibility for vascular access device (VAD) safety and, in many cases, learn to administer their own infusions. Not all infusions or patients are appropriate for home care.
The transition should include assessing the patient’s ability to participate in care, the stability of his or her clinical condition, caregiver availability, use of an appropriate infusion access device, and the home environment. In addition, reimbursement for home care, including the infusion drug or solution, must be verified, and patients should be informed of any out-of-pocket costs.
Patient assessment
Patient motivation, ability, and willingness to participate in care are assessed as part of the planning process. Patients must be informed of their expected level of participation in care. In most cases, particularly with antimicrobial and parenteral nutrition infusions, patients or caregivers are expected to learn how to independently administer infusions. If the patient can’t participate in care, family member or other caregiver assistance is addressed.
Even if a home health nurse administers all infusions (for example, with biologicals or antineoplastic drugs), patients must assume responsibility for living safely with the infusion access device and, in some cases, living with an I.V. solution and/or medication infusion pump. Patients must be able to appropriately respond to alarms, potential complications (such as signs of infection), or adverse reactions.
Many patients and families are anxious or fearful about home infusions, and the nature of the infusion and associated diagnosis (for example, cancer or inability to eat) may evoke additional anxiety. During the transition, the discharging organization, usually the hospital, should communicate significant concerns to the home care agency so the home health nurse can be prepared to address patient fears.
VAD selection
Most patients are referred for home infusion therapy with a VAD already in place, but the home health nurse must ensure that the device is appropriate for the intended therapy. Peripherally inserted central catheters and midline catheters are commonly used in home care; short peripheral catheters are used less frequently because of the length of home infusion therapy or because the prescribed medication or fluid requires central venous access. Tunneled catheters or implanted ports are used when patients require long-term or even lifelong infusion therapies such as chemotherapy or parenteral nutrition. Subcutaneous infusions of medications and hypodermoclysis are increasingly common in home care, home hospice, and palliative care programs.
Home environment evaluation
The home setting should be reasonably safe and clean for medication and supply storage and for infusion administration. It should be assessed for electricity, telephone access, and refrigeration. Home care provider safety also should be evaluated. However, unforeseen safety issues—such as abusive behavior or illegal drug use—may make the home unsafe for the clinician. In such cases, an alternative plan (such as outpatient infusion) is developed with the patient and the provider.
Transitioning a patient to home care should ensure infusion continuity. Antimicrobial medications, for example, should be scheduled to start at home with the next timed dose, although adjustments may be needed for an appropriate home schedule. For instance, a patient prescribed an I.V. antibiotic every 12 hours may have been receiving it at 5 am and 5 pm in the hospital; a more realistic home schedule may be 8 am and 8 pm. In some cases, continuous infusions (such as analgesics, inotropic drugs, or parenteral nutrition) can’t be interrupted as the patient moves from the hospital to home care. In those situations, the infusion pump and medication are delivered to the hospital so the patient can be converted to the home pump before leaving the hospital.
Effective patient and caregiver education
Unlike outpatient or acute-care settings where the nurse typically administers and directly monitors infusion drugs, home infusions frequently require patients and/or caregivers to learn how to administer medications and monitor for adverse reactions and response.
An individual patient’s cognitive ability and willingness to learn, infusion technique complexity, number of available reimbursable home visits, distance from the home care organization, and standards of practice will affect how infusion procedures are taught to patients and family members. Typically, patients or their caregivers are expected to administer solutions and medications, change administration sets, give injections, and adhere to safe and aseptic techniques to reduce complication risk. They’re not routinely expected to place peripheral I.V. catheters or draw blood.
A patient’s readiness to learn and any potential barriers (such as physical weakness, fatigue, or anxiety) will impact his or her ability to learn. Functional limitations (such as manual dexterity or poor memory) also may be a concern. If a patient can’t adequately perform tasks related to infusion therapy or isn’t willing to learn, family members or other caregivers may need to take on this role.
Because the number of authorized home visits for teaching may be limited by the patient’s insurance company, each visit must be used efficiently. If patients or caregivers show difficulty learning, the teaching process must be evaluated. For example: Is teaching consistent (especially a concern when multiple nurses see the patient)? Is the patient experiencing anxiety, functional or cognitive limitations, or lack of motivation? Will additional teaching home visits help?
Interprofessional communication and collaboration
The Infusion Therapy Standards of Practice scope of practice standard states that “members of the healthcare team collaborate to achieve the universal goals of safe, effective, and appropriate infusion therapy.” Along with the patient, the infusion nurse, pharmacist, and physician are the primary healthcare professionals involved in home infusion therapy. Other care team members may include a case manager, physical therapist, social worker, or dietitian.
Communication among the healthcare team is essential to a well-coordinated home infusion program. For example, communication among the nurse, pharmacist, and patient is vital before starting care to establish supply needs based on the access device and infusion. In general, pharmacies deliver supplies to the patient once a week (less or more often based on the stability of the I.V. solutions or drugs). To control care costs, supply needs should be identified up front and throughout therapy to avoid extra deliveries and delays. Most aspects of patient care—such as changing orders, reporting laboratory values, and assessing patients—are communicated via telephone or secure online options. Adverse reactions or significant side effects should be reported to the provider and all relevant members of the healthcare team. In addition, any changes in the patient’s care plan must be communicated to the interprofessional team, the patient, family members, and caregivers. Communicating healthcare information also occurs with the interfacing of computer systems between organizations.
Competent patient care, care planning, and patient assessment and monitoring
Care plan assessment—including home visit frequency, infusion administration procedures, and required assessment and monitoring parameters—are critical to therapy success.
To ensure timely treatment, home visits are scheduled based on individual patient need. At each visit, care is provided with attention to aseptic technique and sound, evidence-based procedures that address VAD care and management, infusion administration, and appropriate monitoring based on infusion type. Attention to safe medication practices includes identifying the patient, comparing and confirming infusion labels to the provider’s orders, checking expiration and beyond-use dates, and verifying infusion pump parameters.
VADs are assessed for dressing and securement device integrity and signs of complications. Routine CVAD and midline site care and dressing changes are completed at least every 7 days. Patency is assessed, including the ability to flush and ascertain a blood return. Peripheral catheters are placed in an appropriate location by competent nurses, with no more than two attempts per nurse and no more than four total in accordance with INS recommendations. This may be a challenge for some home care organizations, which is why clinical competencies are so important. Repeated attempts at venipuncture cause patient pain, delay treatment, limit future vascular access, and increase the risk for complications.
At each visit, nurses should note the effect infusion therapy is having on the life of the patient and caregivers. Simple, short-term home infusion therapies, such as I.V. antimicrobial therapy for an acute and potentially curable infection, generally have little burden. However, complex and long-term infusion therapies associated with chronic illnesses such as cancer may lead to significant disruption in patients’ and caregivers’ lives. Although home infusion therapies (such as chemotherapy, parenteral nutrition, and analgesia) for patients with cancer may extend life and provide symptom palliation and comfort, they also may pose challenges for caregivers as they cope with illness progression and the potential burden of infusion-related interventions and monitoring. Home health nurses must be cognizant of the impact of infusion therapy on patients and their caregivers and address their needs and concerns.
Enhancing safety
Home care organizations can safely deliver home infusion therapy when developed as a specialty program. In accordance with my Model for Safe Home Infusion Therapy, safety is enhanced when the organization implements education, competency assessment, and sound policies and procedures; attention is paid to patient selection and transition to home care; patient education is effective; good communication occurs among the healthcare team and the patient and caregiver; and patient care is well planned and monitored.
Lisa A. Gorski is a clinical education specialist/clinical nurse specialist for Ascension at Home in Wisconsin
References
AAMI Foundation. From Hospital to Home: A Process Map for Successful Infusion Therapy Transition. 2018. aamifoundation.org/wp-content/uploads/dlm_uploads/2018/12/AAMI_HospitaltoHomeGuide_8.5x11_FINAL0918-002.pdf
Gorski LA. Fast Facts for Nurses about Home Infusion Therapy: The Expert’s Best Practice Guide in a Nutshell. New York: Springer Publishing Company; 2017.
Gorski LA. The impact of home infusion therapies on caregivers. Semin Oncol Nurs. 2019;35(4):370-3.
Gorski LA, Hadaway L, Hagle ME, et al. 2016 Infusion therapy standards of practice. J Infus Nurs. 2016;39(1S):S1-159.
Harris M, Gorski LA. Words you never want to hear! Home Healthc Now. 2017;35(8):462-3.
Infusion Nurses Society. Policies and Procedures for Infusion Therapy: Home Infusion. Norwood, MA: Infusion Nurses Society; 2019.
Polinski JM, Kowal MK, Gagnon M, Brennan TA, Shrank WH. Home infusion: Safe, clinically effective, patient preferred, and cost saving. Healthc (Amst.). 2017;5(1-2):68-80.
Zuizewind CA, van Kessel P, Kramer CM, et al. Home-based treatment with immunoglobulins: An evaluation from the perspective of patients and healthcare professionals. J Clin Immunol. 2018;38(8):876-85.

















