This project aimed to decrease fall rates.
- Falls and falls with injury are monitored as a quality metric by hospitals.
- The Agency for Healthcare Research and Quality recommends patient education as an essential element for fall prevention.
- This project aimed to enhance the patient education process related to fall prevention, enabling patients to understand staff interventions while making the education process easier for nursing staff to complete.
ACCORDING TO THE Centers for Disease Control and Prevention (CDC), one out of four people over age 65 falls each year; falling once doubles the chance of falling again. Falls frequently require medical attention, and the CDC states that falls contribute to about 3 million emergency department visits and 1 million hospitalizations among older adults. The National Center for Injury Prevention and Control estimates the annual cost related to adult falls at $50 billion, with Medicare responsible for $29 billion yearly.
Patient falls in the acute inpatient setting remain a common safety concern for hospitals. According to 2019 Patient Safety Network (PSN) data, falls occur at a rate of three to five per 1,000 bed-days; 700,000 to 1 million hospitalized patients fall each year. PSN also notes that more than one-third of hospital falls result in injury, including fractures and head trauma. Death or serious injury resulting from a fall while in a healthcare facility is considered a never event, and the Centers for Medicare & Medicaid Services doesn’t reimburse hospitals for additional costs associated with patient falls.
Nurse-driven frailty screening
The situation at one hospital
A patient fall committee at an acute care hospital in a midwestern state reviewed their quality metric data for patient falls and falls with injury in December 2021. The committee, which included bedside nurses, a physical therapist, a nurse manager, a nursing director, a clinical nurse specialist (CNS), and quality department members, observed a concerning trend: At least half of the falls between July and December 2021 resulted from lack of patient adherence to their fall prevention plan of care. This finding led the committee to question whether patients fully understood their fall prevention instructions or if they chose not to follow them despite understanding the plan.
A quality improvement (QI) team, consisting of a CNS and a nurse educator, facilitated random interviews with 150 patients on the two inpatient units (progressive care and medical–surgical) with the highest number of falls. The data indicated that 25% of patients on the progressive care unit and 31% of the patients on the medical–surgical unit couldn’t identify interventions used by staff to prevent falls.
Fall prevention in hospitals remains complex with limited research using randomized control trials. A systematic review and meta-analysis by Morris and colleagues concluded that education remains the most effective fall reduction strategy. PSN emphasizes the need for individualized fall prevention measures. However, individualized patient education can prove challenging for nurses prioritizing various patients’ needs.
Could a simple, easy-to-use, one-page education tool listing common interventions for fall prevention improve patients’ understanding of their plan of care and decrease falls? The QI team identified an opportunity for a project with the PICOT (Problem, Intervention, Comparison, Outcome, Time) question: For patients on the medical–surgical and progressive care units at the project site, does a standardized one-page patient education sheet compared to current practice affect the rates of patient falls and falls with injury during a 12-month period?
The literature search
The Poster
The quality improvement team developed the following poster after reviewing similar posters created by other organizations. Upon patient admission to a room, the nurse circles the relevant risks and interventions as a reminder to patients, family, visitors, and staff.

The QI team conducted a literature search targeting peer-reviewed, full-text articles from January 2018 through May 2022. Within CINAHL Complete and PubMed databases, they searched the terms “fall prevention in hospitals” and “patient education or patient teaching.”
CINAHL Complete yielded 50 potential articles and PubMed returned 65. After narrowing down the articles to those specific to patient fall education content or tactics, 13 articles met inclusion criteria for the final review.
The intervention
Using a standard patient education poster, this QI project aimed to decrease patient falls on a progressive care unit and a medical–surgical unit. The QI team conducted monthly reviews of fall rates and falls with injury rates on these inpatient units to determine the intervention’s effects.
Poster design
The committee designed a patient fall education poster (PFEP) similar to those used by Fowler and Reising and Rohm and colleagues. Their posters listed patient fall risk factors and interventions for prevention. Both demonstrated various reductions in fall rates; however, neither tool had been tested for validity or reliability.
Fowler and Reising’s Fall TIPS Poster appears as an organized chart with simple language, colors, and pictures. An inclusive list of patient fall risks runs down the first column but without common interventions related to fall prevention, such as gait belts, socks with grips, and calling for help to get up. Similarly, Rohm and colleagues’ Safety Plan poster presents fall risks in the top row but omits important risk factors (such as previous falls and confusion) and misses key interventions, including gait belts and assistive devices. Both studies stressed that the poster should be at least 11΄΄ x 17΄΄; Rohm and colleagues specifically noted the use of a 48-point font.
Fall rates decreased after several months in both studies; however, neither decrease showed statistical significance. Similarly, a study by Rochon and Salazar developed a fall prevention program using an educational flier with discussion about fall safety at the bedside. They saw patient falls trend down and experienced two consecutive months with no falls.
Ultimately, the PFEP listed patient risks and interventions (with color illustrations based on the project site’s fall prevention policy. The committee edited the poster based on feedback from a progressive care staff nurse, a med–surg staff nurse, the hospital’s shared governance council, and the clinical nurse educator group. (See The poster.)
Poster education
The QI team established a procedure for the PFEP intervention, which included poster maintenance, fall risk determination using the Morse Fall Scale, and discussion with patients and families about risks and appropriate interventions. In September 2022, the team provided education on current fall rates and the PFEP process in PowerPoint presentations at unit staff meetings. (See Intervention procedure.)
Intervention procedure
The quality improvement team developed the following procedure for implementing the patient fall education poster (PFEP) intervention.
To aid understanding, remember to do the following:
- Progressive care and med–surg nursing leadership maintain PFEPs.
- Laminated PFEPs hang on the closet door below the television in all patient rooms on each unit.
- On admission to the room, after completing the Morse Fall Scale, the nurse circles the patient’s risks for falls in the top row of the PFEP with the whiteboard marker.
- The nurse circles the interventions in the following rows applicable to the patient.
- The nurse narrates the risks and the interventions, briefly explaining them to the patient and family during or immediately after marking them on the PFEP.
- The nurse answers patient and family questions.
- During every bedside shift report, the off-going nurse reviews the PFEP with the oncoming nurse, patient, and family. Changes are made as necessary using a paper towel to wipe off previous information and the whiteboard marker to circle new risks and interventions.
- If a patient moves to a different room, the PFEP remains in the room and staff use the PFEP located in the new room.
- Environmental services wipes off the PFEP during terminal room cleans.
To ensure patients and family members can easily see the posters, the QI team hung them on the closet doors beneath the televisions in all patient rooms on both units. On patient admission, the nurse circles characteristics that put the individual patient at risk for falls as well as the appropriate fall prevention interventions. The nurse then reviews the poster with the patient and family or support person, and nurses reference it with every bedside shift report.
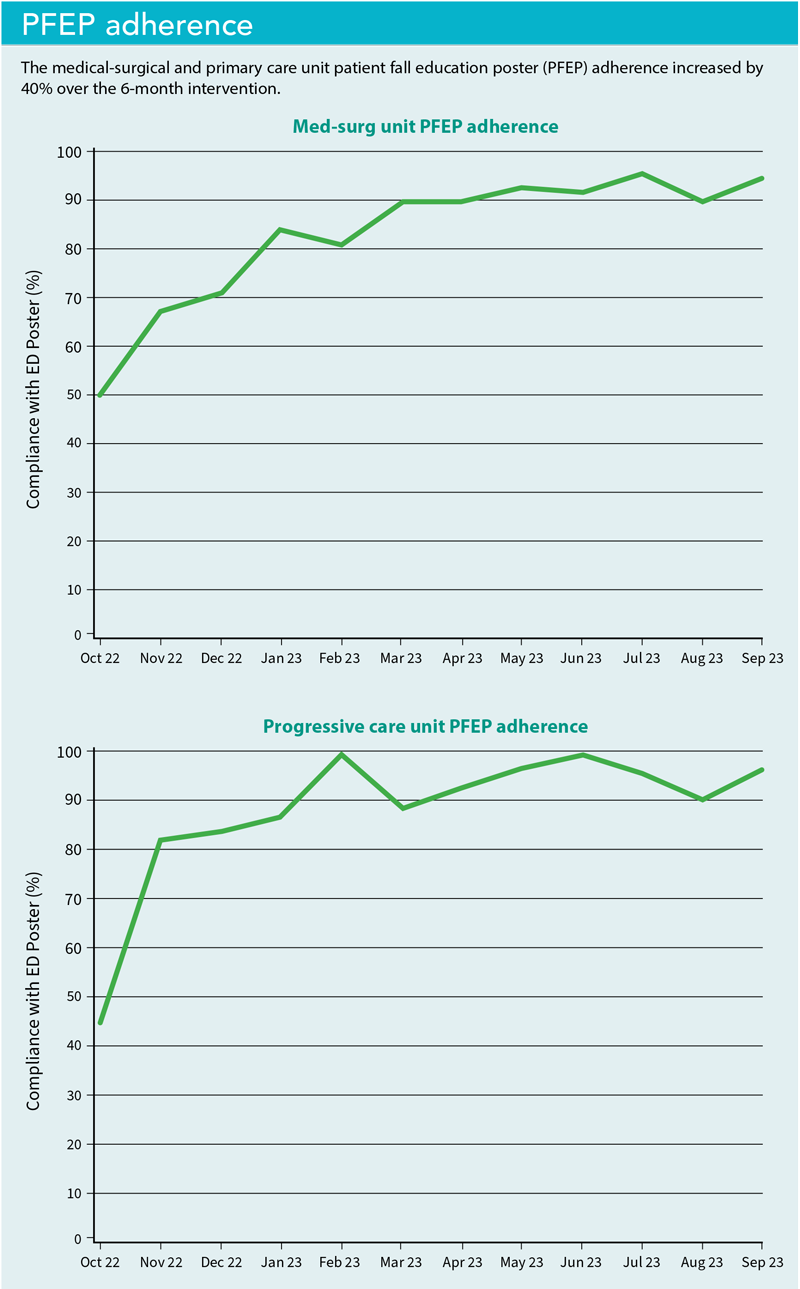 To validate and improve intervention adherence, the QI team performed random weekly audits beginning in October 2022. Aiming to improve poster use by nurses and to stress the importance of the intervention, the team shared with staff percentages of audit results on each unit’s private Facebook page. Both units started with a 50% adherence rate. After 6 months, both achieved 90% adherence, consistently demonstrating a change in practice. (See PFEP adherence figures illustrating this improvement)
To validate and improve intervention adherence, the QI team performed random weekly audits beginning in October 2022. Aiming to improve poster use by nurses and to stress the importance of the intervention, the team shared with staff percentages of audit results on each unit’s private Facebook page. Both units started with a 50% adherence rate. After 6 months, both achieved 90% adherence, consistently demonstrating a change in practice. (See PFEP adherence figures illustrating this improvement)
Process improvements
Beginning in November 2022, leaders already assigned to a block of rooms to visit patients and address topics related to patient experience added support for the project by acknowledging the PFEP and reviewing interventions with patients. Leaders identified an opportunity to provide the PFEP in Spanish to meet the needs of a small population of patients. The committee created a Spanish language poster in February 2023.
Results
Fall rates, defined by the Agency for Healthcare Research and Quality as falls per 1,000 occupied bed days, serve as the standard measure for fall prevention success. Similarly, the rate of falls with injury provides another direct measure of success for patient safety. The med–surg unit’s monthly fall rates compared to the national mean for similar units, as determined by Press Ganey National Database of Nursing Quality Indicators (NDNQI), consistently remained above the national mean throughout the project. A spike occurred in April 2023, with one patient falling seven times. Similarly, the hospital’s progressive care unit fall rates remained above the mean with the exceptions of May and October 2023.
Limitations
This QI project focused on only two units at one midwestern hospital. Results mirrored data currently in the literature. Routine audits confirmed nurse adherence with completing the PFEP, but poster review with patients at the bedside shift report wasn’t verified. Nurses may not have regularly reviewed the posters with patients.
During data dissemination with unit staff, several nurses commented that the morning bedside shift report isn’t a suitable time to review fall information with patients just waking up. Staff also suggested adding a patient signature line at the bottom of the poster signifying their agreement to follow the fall prevention interventions.
Potential for success
The PFEP serves as an inexpensive and straightforward process to quickly educate oriented, adult patients on fall prevention tactics in the hospital setting. However, this QI project didn’t show a significant decrease in falls on either unit that implemented the intervention. A decrease in falls with injury occurred throughout the project but showed no statistical significance.
Staff reported appreciating the time saved using the PFEP to educate and facilitate discussion about fall prevention, but further study could identify optimal times for routine PFEP review, audit adherence with poster completion and review, and coach staff in the practice change.
Susan Lilly is a clinical nurse specialist at CHI Health St. Elizabeth in Lincoln, Nebraska. Nicole Ragon is a clinical educator at CHI Health St. Elizabeth. Ryan W. Walters is faculty, at Creighton University in Omaha, Nebraska.
References
Agency for Healthcare Research and Quality. Module 5: How to measure fall rates and fall prevention practices. 2017. search.ahrq.gov/search?q=how+do+you+calculate+fall+rates&siteDomain=archive.ahrq.gov
Centers for Disease Control and Prevention. Cost of older adult falls. July 9, 2020. stacks.cdc.gov/view/cdc/122747
Centers for Disease Control and Prevention. Facts about falls. May 9, 2024. cdc.gov/falls/data-research/facts-stats/?CDC_AAref_Val=https://www.cdc.gov/falls/facts.html
Fowler SB, Reising ES. A replication study of Fall TIPS (Tailoring Interventions for Patient Safety): A patient-centered fall prevention toolkit. MEDSURG Nurs. 2021;30(1):28-34. doi:10.62116/msj.2021.30.1.28
Morris ME, Webster K, Jones C, et al. Interventions to reduce falls in hospitals: A systematic review and meta-analysis. Age Ageing. 2022;51(5): afac077. doi:10.1093/ageing/afac077
Patient Safety Network. Falls. June 15, 2024. psnet.ahrq.gov/primer/falls
Rochon R, Salazar L. Partnering with the patient to reduce falls in a medical-surgical unit. Int J SPHM. 2019;9(4):135-42.
Rohm CD, Whiteman K, Swanson-Biearman B, Stephens K. Interprofessional collaboration to reduce falls in the acute care setting. MEDSURG Nurs. 2020;29(5):303-7.
University of North Carolina Health Sciences Library. Creating a PRISMA flow diagram. October 27, 2025. guides.lib.unc.edu/prisma
Key words: fall prevention, patient education