
Astute nursing assessment facilitates timely treatment.
- Pericarditis, a cardiac condition, requires astute clinical assessment.
- Treatment includes nonsteroidal anti-inflammatory drugs and colchicine.
History and assessment
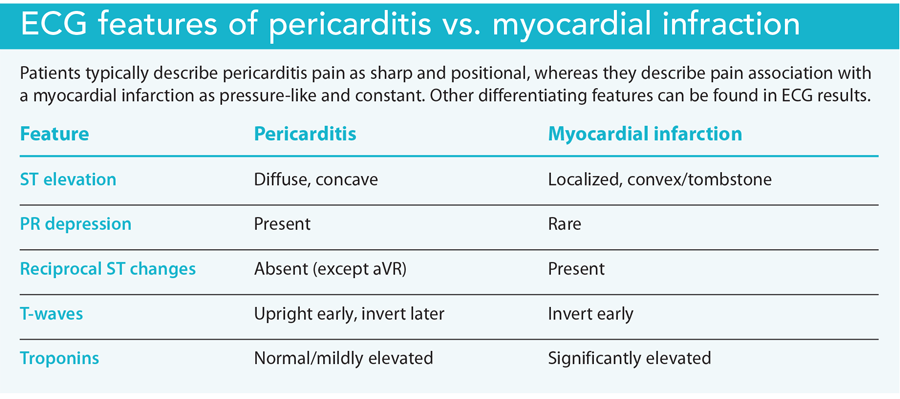
Mr. Webster describes his chest pain to the ED nurse (Marci) as sharp, worse when lying flat, and improved when leaning forward. He reports no radiating pain, nausea, diaphoresis, or shortness of breath. Mr. Webster’s vital signs are temperature 100.8° F (38.2° C), HR 98 bpm, respiratory rate 22 breaths per minute, BP 132/84 mmHg, and SpO2 96% on room air. A 12-lead ECG shows diffuse ST-segment elevation without reciprocal changes. (see ECG features of pericarditis vs. myocardial infarction.)
When auscultating Mr. Webster’s chest, Marci hears a faint, high-pitched “scratching” sound in the left lower sternal border consistent with a pericardial friction rub. Concerned about acute pericarditis, she secures a bed for him in the treatment area.
Taking action
Marci places Mr. Webster on continuous cardiac monitoring, and the attending physician orders a chest x-ray, CRP, ESR, CBC, CMP, and troponin level. Over the next hour, Mr. Webster reports worsening chest discomfort. He becomes anxious, restless, and tachycardic with a heart rate of 124 bpm. His BP drops to 90/62 mmHg. Marci notifies the physician, who notes jugular vein distention and muffled heart sounds, consistent with cardiac tamponade and Beck’s triad (hypotension with narrowed pulse pressure, jugular vein distention, and muffled heart sounds).
A bedside echocardiogram reveals a large pericardial effusion. A cardiologist performs an ultrasound-guided pericardiocentesis, aspirating 400 mL of serosanguinous fluid. Mr. Webster remains hypotensive. The cardiologist orders a 500 mL normal saline bolus and admits the patient to the CICU for close monitoring.
Outcome
While in the CICU, Mr. Webster’s chest discomfort improves. His BP stabilizes at 122/78 mmHg, and his HR decreases to 88 bpm. The cardiologist orders oral ibuprofen 800 mg three times a day for anti-inflammatory management and oral colchicine 0.5 mg twice a day to prevent pericarditis recurrence. (See Pericarditis treatment options)
Pericarditis treatment options
Treatment includes nonsteroidal anti-inflammatory drugs (NSAIDs) for 1 to 2 weeks, tapered after symptoms resolve and the CRP normalizes, as well as colchicine for 3 months to reduce the risk of recurrence. Proton pump inhibitors can provide gastroprotection secondary to NSAID use. Patients who don’t respond to anti-inflammatory therapy and whose pericarditis isn’t the result of an infection may benefit from corticosteroids. ESR and CRP levels aid treatment monitoring. Patients should receive education about the importance of adhering to the prescribed medication regimen and avoiding strenuous activity until cleared by cardiology.
Mr. Webster’s CRP and ESR trend down, and an infectious and autoimmune workup are initiated to identify the etiology of the pericarditis. He’s discharged home 2 days later with primary care and cardiology follow-up.
Education and follow up
Pericarditis, an inflammation of the pericardial sac, typically occurs as a result of a viral infection. It’s most common in men between 20 and 50 years of age and affects 5% of patients who arrive in the ED for non-ischemic chest pain.
Diagnosis requires at least two of the following: sharp, pleuritic chest pain that worsens when lying flat and improves when sitting up; pericardial friction rub; pericardial effusion; and widespread ST elevation or PR depressions. Symptoms typically last less than 4 to 6 weeks.
Acute pericarditis and associated complications, including cardiac tamponade, can prove fatal. Timely diagnosis and treatment are essential. In Mr. Webster’s case, Marci’s astute nursing assessment facilitated prompt implementation of an evidence-based treatment plan.
*Name is fictitious.
Aaron Sebach is dean and professor at Wilmington University in Wilmington, Delaware. Bradley Helmuth is a cardiology nurse practitioner at TidalHealth in Salisbury, Maryland.
American Nurse Journal. 2025; 20(8). Doi: 10.51256/ANJ082518
References
Chiabrando JG, Bonaventura A, Vecchié A, et al. Management of acute and recurrent pericarditis: JACC state-of-the-art review. J Am Coll Cardio. 2020;75(1):76-92. doi:10.1016/j.jacc.2019.11.021
Cremer PC, Klein AL, Imazio M. Diagnosis, risk stratification, and treatment of pericarditis: A review. JAMA. 2024;332(13)1090-110. doi:10.1001/jama.2024.12935
Dababneh E, Siddique MS. Pericarditis. StatPearls. August 8, 2023. ncbi.nlm.nih.gov/books/NBK431080
Imazio M. Acute pericarditis: Treatment and prognosis. February 29, 2024. uptodate.com/contents/acute-pericarditis-treatment-and-prognosis
Ismail TF. Acute pericarditis: Update on diagnosis and management. Clin Med. 2020;20(1):48-51. doi:10.7861/clinmed.cme.20.1.4
Myocarditis Foundation. Pericarditis. www.myocarditisfoundation.org/pericarditis/
Key words: pericarditis, rapid response, cardiology


















