
Patient falls from chairs are increasing at an alarming rate: What can a hospital’s nursing staff do to stop this trend? That was the challenge faced by unit leaders of the Center for Rehabilitation at Wilmington Hospital.
Notification that falls were increasing came as a surprise to us. Just 2 years earlier, we had lowered our overall fall rate below the goal recommended by the National Database of Nursing Quality Indicators®.
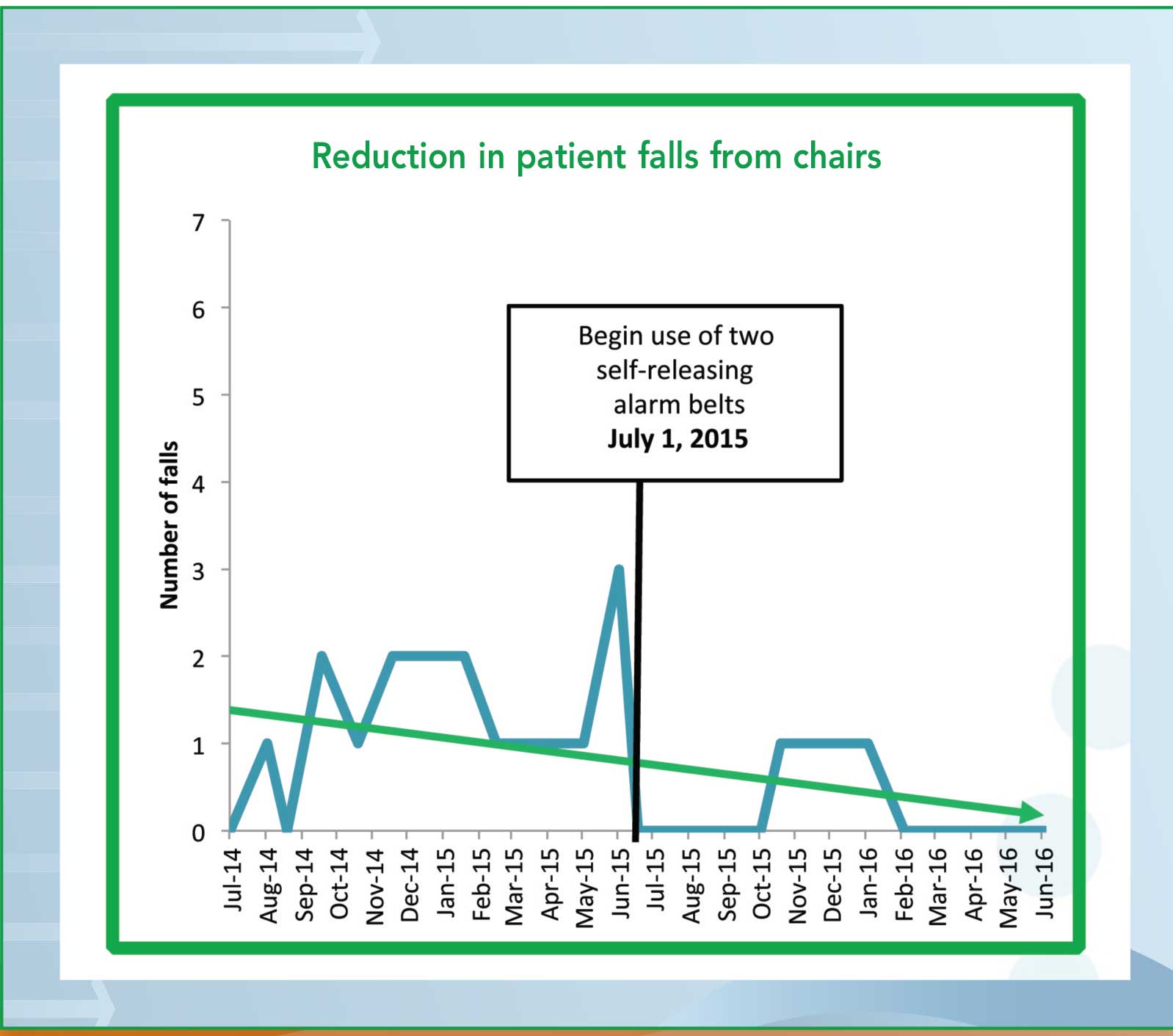
No single factor could explain the increase, indicating a need for system-wide change. We established a goal: Decrease the number of patients falling out of their chairs by 10% for fiscal year 2016 (from July 2015 to June 2016).
We not only met our goal, we exceeded it. We lowered the center’s overall fall rate as well. For fiscal year 2016, we achieved the following results:
• Three total falls from chairs, compared to 16 the previous fiscal year (See Reduction in patient falls from chairs.)
• 81.3% reduction in falls from chairs
• 0 patients requiring observation at nursing station.
Case study
An 89-year old man was admitted to the rehabilitation unit with a fracture of the lower extremity, status post-hemiarthroplasty of the right hip, with posterior hip precautions and weight bearing as tolerated. On initial assessment, we had difficulty evaluating his orientation because he had extreme hearing loss. He needed moderate assistance for transfers and minimal assistance to ambulate with a rolling walker. His Morse Fall Scale score was greater than 45, indicating a high level of risk for falls.
Based on unit criteria for high fall risk and high risk of injury from a fall, we applied dual-alarm, self-releasing belts to the patient’s wheelchair and recliner chair as part of his plan of care. He was placed in a room directly across from the nursing station, and we implemented many of the other components of our action plan for reducing falls from chairs, including using a low bed with mats.
The patient would attempt to get up by himself eight to 10 times each day, even though his call bell was in reach, often without locking his wheelchair. When he opened one of his belts and began to stand up, the alarm would sound while the second belt kept him in place. Before he could get the second belt open, staff would go to his room, thereby preventing a fall.
The patient’s daughters were grateful for the self-releasing alarm belts, telling us these belts prevented their father from falling on many occasions. Staff agreed he would have fallen multiple times had it not been for the belts.
Our action plan
To achieve these results, we gathered and analyzed baseline data, such as which patients were falling from chairs, when and where falls occurred, and what led to falls. We researched options for up-to-date prevention tools.
We implemented use of the Morse Fall Risk Assessment Tool, along with an action plan that incorporates low beds with mats and bed alarms, nonskid socks, and yellow fall-risk armbands. It mandates new procedures; for example, placing fall-risk signs outside patient rooms, instituting hourly rounding and no-pass zones, and establishing criteria for identifying patients at-risk for falls or for injury with a fall. We also began holding fall huddles at the change of every shift and using patient handoff signs.
We established new policies for how to respond should a fall take place. We require staff to call the nurse manager immediately after a patient fall to debrief him or her about the incident; hold post-fall meetings with patient, therapist, and nurse; make sure the outcome of a patient’s fall is documented in the electronic health record; discuss falls and lessons learned at all staff meetings; and hold mandatory yearly fall summits.
Double protection
The most significant and perhaps most effective decision was to use two self-releasing alarm belts* for patients who meet specified criteria for fall risk. Using two belts—one with a release on the right and one on the left—gives staff additional time to prevent a fall. When the first belt alarm sounds, staff members have the opportunity to reach the patient before the second belt is opened.
The alarm belts aren’t considered restraints; they are secured around the patient with Velcro fasteners, so they release easily. The belts are then secured to the chair with a hook and loop fastener. Before alarm belts are used, the patient must demonstrate the ability to release them without any assistance. We use data analysis to select who should receive selfreleasing alarm belts before patients enter our facility so we can have a chair with the belts waiting in the patient’s room on admission. If belt use is established from the start, the patient is less likely to perceive it as a punishment, compared to using belts for the first time after a fall has occurred.
The path forward
To avoid losing ground in our initiative to reduce falls from chairs, we monitor staff compliance, continue with data collection, and report data monthly. In addition, we share findings with other units and other hospitals and advocate for the use of self-releasing belts in acute-care settings.
Editor’s note: This is one in a series of recurring case studies describing success stories in preventing falls and injuries from falls. The series is brought to you by Posey. Watch for the next case study in the July issue of American Nurse Today.


















{kind=link}