Triage assessment results in prompt attention.
- Spontaneous pneumothorax occurs in the absence of an obvious etiology.
- It’s most common in tall, thin males with a history of tobacco or cannabis use.
- Tension pneumothorax, a rare, potentially life-threating complication, requires timely identification, diagnosis, and definitive treatment.
COLBY ROGERS*, a 19-year-old man with no significant medical history, develops sudden, sharp, left-sided chest pain while playing basketball. After 8 hours, his pain doesn’t improve with over-the-counter acetaminophen, prompting a visit to the ED.
History and assessment
Lauren, the triage nurse, assesses Colby, who says that his pain worsens with inspiration. He denies trauma but reports mild dyspnea with exertion. His vital signs are temperature 36.5°C (97.7°F), HR 113 bpm, RR 24 breaths per minute, BP 104/60 mmHg, and O2 saturation 95% on room air. Colby is 6’7” tall and weighs 151 lbs (68.6 kg). Auscultation of Colby’s lungs reveals diminished breath sounds on the left. Concerned about a spontaneous pneumothorax, Lauren escorts Colby to the treatment area and notifies the ED physician.
Taking action
Lauren places Colby on a cardiac monitor with continuous pulse oximetry monitoring. The advanced practitioner notes tachycardia and left-sided decreased breath sounds and hyperresonance. She orders 15 L of oxygen via non-rebreather mask. A two-view chest x-ray reveals a left-sided pneumothorax measuring 13% of the hemithorax. Given Colby’s clinical stability and the small size of the pneumothorax, chest tube insertion isn’t indicated. Cardiothoracic surgery recommends overnight observation with continued cardiopulmonary monitoring and 100% oxygen via non-rebreather mask.
Outcome
In the observation unit, Colby receives 975 mg of acetaminophen every 8 hours as needed for mild pain and 50 mg of tramadol every 8 hours as needed for severe pain. The next morning, his RR and HR have normalized and he’s weaned from oxygen. He doesn’t experience dyspnea on exertion or exhibit hypoxia. A repeat x-ray shows improvement of the pneumothorax. He’s discharged home with close primary care follow-up and an order for a repeat chest x-ray in 24 hours.
Education and follow-up
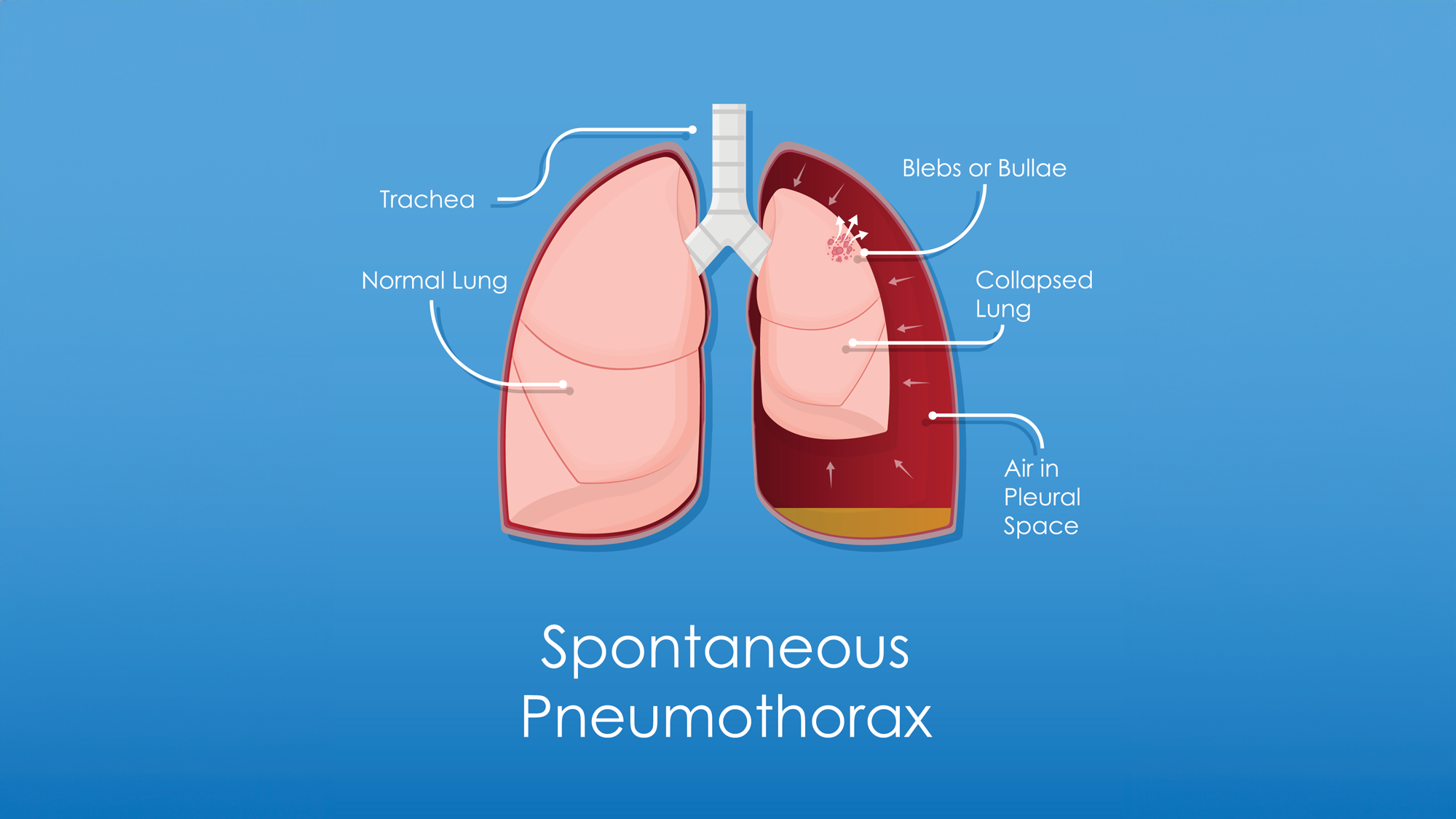
Pneumothorax occurs when gas collects in the pleural space between the lungs and chest wall. Spontaneous pneumothorax (no obvious etiology), classified as primary (no underlying pulmonary disease) or secondary (with underlying pulmonary disease such as COPD), occurs more frequently in males than females. Risk factors include tall, thin body and a history of tobacco or cannabis use. (See Spontaneous pneumothorax: Symptoms)
Spontaneous pneumothorax: Symptoms
Patients with spontaneous pneumothorax commonly report a sudden onset of sharp, ipsilateral, pleuritic chest pain at rest. Dyspnea on exertion and tachycardia also may occur, particularly with secondary spontaneous pneumothorax. Patients with large pneumothoraces may experience ipsilateral decreased or absent breath sounds, pulsus paradoxus, or jugular venous distention. Tension pneumothorax, a rare, potentially life-threatening complication, presents in patients as hypoxia, tracheal deviation, and hypotension.
Diagnosis of spontaneous pneumothorax relies on physical examination, present illness, and chest radiography. Initial treatment for all patients includes 100% oxygen via a non-rebreather mask and cardiopulmonary monitoring. High-flow oxygen enhances the rate of gas absorption in the pleural space.
Clinically stable patients, such as Colby, can be managed conservatively with supplemental oxygen, monitoring, and repeat chest x-ray before discharge with close follow-up. Large pneumothoraces require chest tube insertion, whereas recurrent pneumothoraces may require video-assisted thoracoscopy surgery or chemical pleurodesis.
Patient education should include recommendations to delay air travel and strenuous activity for 1 week after pneumothorax resolution and information about symptoms (worsening dyspnea, chest pain) that require emergency care.
Spontaneous pneumothorax and associated complications, including tension pneumothorax with airway compromise, can prove fatal. Timely identification, diagnosis, and definitive treatment are critical. In Colby’s case, Lauren’s triage assessment facilitated immediate implementation of an evidence-based treatment plan.
*Names are fictitious
Aaron Sebach is a dean and professor at Wilmington University in Wilmington, Delaware. Bradley Helmuth is a cardiology nurse practitioner at TidalHealth in Salisbury, Maryland.
American Nurse Journal. 2026; 21(1). Doi: 10.51256/ANJ012656
References
American Thoracic Society. Patient education information series: What is a spontaneous pneumothorax? Am J Respir Crit Care Med. 2020;202:33-4. thoracic.org/patients/patient-resources/resources/spontaneous-pneumothorax.pdf
Costumbrado J, Ghassemzadeh S. Spontaneous pneumothorax. StatPearls. July 22, 2025. ncbi.nlm.nih.gov/books/NBK459302
Lee GYC. Treatment of primary spontaneous pneumothorax in adults. UpToDate. uptodate.com/contents/treatment-of-primary-spontaneous-pneumothorax-in-adults
Mendogni P, Vannucci J, Ghisalberti M, et al. Epidemiology and management of primary spontaneous pneumothorax: A systematic review. Interact Cardioasc Thorac Surg. 2020;30(3):337-45. doi:10.1093/icvts/ivz290
Shorthose M, Barton E, Walker S. The contemporary management of spontaneous pneumothorax in adults. Breathe. 2024;19(4):230135. doi:10.1183/20734735.0135-2023
Key words: spontaneous pneumothorax, respiratory assessment


















