
A gap analysis at the project site (which offers surgical services, including procedures requiring overnight admission and postoperative pain management with narcotic and non-narcotic pain medication) using retrospective chart reviews showed ineffective pain management based on patient self-reported pain scores. The improvement initiative was guided by this PICOT (patient, intervention, comparison, outcome, time) question: For nursing staff caring for adult surgical procedure patients admitted to a medical or surgical floor post-procedure (P), how does implementing targeted music listening therapy with patient education using teach back (I) versus current practice focusing on pharmacologic pain treatment (C) affect postprocedure pain management (O) over 12 weeks (T)?
The baseline data showed an opportunity to offer patients more resources to help manage their postprocedure pain and reduce the gap between current pain levels and acceptable pain levels. Patient perception is subjective, as is pain experienced after a surgical procedure. This quality improvement initiative enabled a nurse-driven, evidence-based process offering patients an alternative, complementary approach to addressing pain outside of traditional oral pain medication, which, according to Önal Alkan, can have a synergistic effect. Patients’ overall satisfaction with their care experience is tied to reimbursement for many facilities, and facility rankings are often posted online for public viewing.
Literature support
A review of available research across multiple databases yielded information organized into themes as part of the project’s literature synthesis. The four main themes noted in the articles, synthesized and used to support foundational concepts of intervention implementation, included music therapy with patient input, music therapy without patient input, surgical procedure-related pain, and surgical procedure-related pain-related anxiety. Many of the articles in the literature synthesis, including by Suarez and colleagues, discussed nurse-driven initiatives that used nonpharmacological pain management in conjunction with other treatment modalities to produce a complementary effect, thereby modifying patients’ perception of acute pain postprocedure.
The final group of scholarly journal articles were synthesized into a cohesive group to support the project, creating a framework for an evidence-based, nursing-driven, literature-supported implementation plan.
Quality improvement initiative
This quality improvement initiative followed a continuous cycle of process improvement, using the plan-do-study-act (PDSA) format. After training, the pre-op clinic nurse educator added an insert to the pre-op clinic patient instructions to reinforce listening to music therapy at home between the pre-op visit and surgery day.
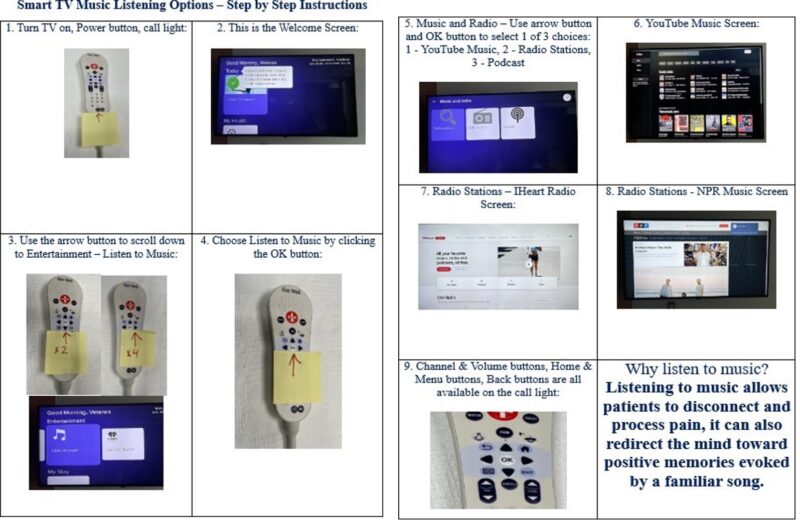
For scheduled surgeries requiring a minimum 24-hour post-procedure stay and “floor status” patients, the primary nurse admitted the patient and documented per facility policy. A unit staff nurse then provided a handout on accessing streaming music services on Smart TVs in patient rooms as part of the admission process.
Frontline nursing staff completed a patient pain assessment every 12 hours per facility standards, which are part of the electronic health record (EHR). Postdischarge, a project team member collected data from the EHR for all patients who received the nurse-driven intervention. Over 7 weeks, pre- and postintervention data were compiled and compared once the sample size matched the baseline.
Outcome
The pain scores were extracted from the patient’s EHR and the nursing shift assessment standard national health system note. The project leader recorded pain score data extracted from the patient’s chart on a password-protected Excel spreadsheet, with the two pain score categories averaged over 48 hours postprocedure. The leader then compared the two groups: patients with a current pain score average at or below their average acceptable pain score, and those with an average current pain score greater than their average acceptable pain score. The project team completed this process for 70 patients before intervention implementation and for 73 patients after.
Stakeholders and leadership interpreted the improved patient experience reflected in the data as a clinically significant change. Baseline data showed that of the 70 patients, 84% (59 out of 70) had average current pain scores greater than their average acceptable pain score, with a project goal to reduce this to 25% or less postintervention implementation over the planned period. The final data showed a change to 56% (41 out of 73), which wasn’t as low as the project target but still reflects a shift toward improved patient experiences. The clinical significance of the results relates to patient experience, which improved as the patient-reported pain score (when averaged) showed that more patients’ acute pain scores were at or below their acceptable pain scores.
Note: Pre-Implementation Cohort: 70 patients, Post-Implementation Cohort: 73 patients
Return on investment
One of the advantages of this kind of project is the ability to harness existing technology resources, which means minimal financial impact on any facility attempting to reproduce results when similar technology is already available in-house. The patient interaction with the preop nurse educator and the staff nurse upon admission would have occurred regardless of the intervention, and the added time to each role’s workflow was 5 to 10 minutes per patient per shift.
The streaming music services were already available on the Smart TV in each patient room but were cumbersome to navigate and traditionally underused. By providing the patient with written instructions for the Smart TV streaming music service and reinforcing them with nursing staff, it became an accessible resource that improved the patient experience.

Potential challenges
The patient’s perception of postprocedure pain is subjective and self-reported, which can potentially make it challenging to move this metric. This project had the advantage of an existing requirement that nurses assess and document patients’ self-reported current and acceptable pain score every 12 hours. This allowed the project team to use the pain scores charted in the nursing assessment as a metric without changing nursing workflow or documentation. Implementing the intervention would have been more challenging if it had required a significant change to nursing workflow or charting.
The project leader already had a collaborative relationship with the surgical unit staff and the preop nurse educator, which allowed for dissemination of information along existing communication channels. The preop nurse educator (who meets with patients 1:1) had the advantage of unvarnished patient responses, which were then communicated to the project leader. These responses showed excitement and engagement when patients were given the option to choose parts of their postprocedure care plan.
Connecting to patient experience
This project provided a great opportunity to harness existing technology in a way that requires minimal cost to the facility and maximum impact on the patient experience, as reported by the patients themselves. Patients asked whether they could bring their own musical instruments to play after surgery, recorded their worship services before surgery, and even made playlists they shared on streaming music services. The available literature on complementary pain management can be used by nursing staff at any facility to harness existing technology to enhance the patient experience.
Sarah Wright DNP, RN, is a Nurse Manager at Harry S Truman Veterans Memorial Hospital in Columbia, MO.
References
Önal Alkan A, Uslu Y, Karabacak U, Adigüzel Akbaba M. Effect of music therapy on dressing pain in intensive care patients with pressure injury. Adv Skin Wound Care. 2025;38(8):419-25. doi:10.1097/asw.0000000000000336
Suarez A, Delgado Y, Servais A, et al. Effects of combining music therapy, light therapy, and chromotherapy in the treatment of chronic pain patients: A pilot study. Evid Based Complement Alternat Med.2024:3006352. doi:10.1155/2024/3006352

















