Improving efficiency and nurse confidence
- Nurses can face challenges with peripheral I.V. insertion, particularly in patients with difficult I.V. access.
- Evidence-based practice recommendations emphasize a shift away from traditional visualization and palpation techniques toward the use of ultrasound guidance, which can improve efficiency, increase nurse confidence, and enhance overall clinical competence.
- Healthcare organizations to support this transition by investing in training and implementing clear, standardized guidelines.
Learning Objectives
- Describe DIVA challenges and ultrasound-guided PIV use.
- Identify core elements of ultrasound-guided PIV training.
- Apply evidence-based DIVA management practices.
Reflective Learning Question 1:
What clinical challenges make PIV insertion difficult in patients with DIVA, and how can ultrasound guidance help?
Reflective Learning Question 2:
Which components of an ultrasound-guided PIV training program would be most impactful in your practice setting?
No relevant financial relationships were identified for any individuals with the ability to control content of the activity.
Expiration: 7/1/29
1.5 ANCC contact hours
NURSES FREQUENTLY ENCOUNTER challenges with peripheral I.V. (PIV) insertion, especially among adult patients with difficult I.V. access (DIVA), resulting in multiple unsuccessful skin punctures. Bahl and colleagues define DIVA as two or more failed PIV access attempts using traditional techniques such as visualization and palpation. Most patients with DIVA are older, have chronic and complex health comorbidities, have high body mass index, are undergoing chemotherapy treatment, or have a history of I.V. drug use. According to Davis and colleagues, patients with DIVA have an increased risk of multiple failed PIV catheter insertion attempts and are likely to experience and report moderate-to-severe pain, vein depletion, complications, and increased length of stay.
Many nurses continue to apply the traditional visualization and extremity palpation technique to obtain vascular access. However, patients with DIVA require advanced techniques, such as ultrasound, to display good-quality vein images and facilitate successful PIV cannulation.
Tuomela and colleagues describe efficiency as service quality, productivity, performance, customer satisfaction, and workforce satisfaction. Schuster and colleagues identify confidence as one of the most important attributes for enabling nurses to make appropriate care decisions. The increasing number of patients with DIVA in our organization and nurses’ feedback concerning multiple failed PIV catheter insertion attempts illustrated an identified literature and practice gap specific to patients with DIVA. Improving the nurses’ PIV insertion skills efficiency and confidence could elevate not only performance standards, patients’ trust, and customer satisfaction but also workforce satisfaction.
An interprofessional team at our organization initiated a quality improvement (QI) project to decrease failed PIV insertion attempts, establish hospital practice guidelines, and improve nurses’ PIV skills efficiency and confidence. The project leader, a clinical education and professional development nurse, completed a gap analysis and identified that the community hospital’s existing PIV therapy and management policy lacked current evidence-based practice standards. The gap analysis also identified the lack of an ultrasound-guided PIV insertion training program. With acutely ill patients continuing to require prompt PIV access for care management, nurses require technology aids, such as ultrasound guidance, and clear evidence-based practice standards to improve their PIV insertion skills efficiency and confidence.
Literature review
The project team conducted a literature review using PubMed, CINAHL, Cochrane Database of Systematic Reviews, and Joanna Briggs Institute databases. Search terms included “peripheral intravenous catheter insertion or cannulation,” “nurses,” and “ultrasound.” Search parameters included full-text, peer-reviewed, English-language literature from 2019 to 2023.
Recent literature and guidelines recommend using ultrasound guidance to increase PIV insertion first-attempt success, noting that it reduces the number of failed attempts and time to successful PIV cannulation, especially among patients with DIVA.
Standard technique vs ultrasound-guided technique
In a scoping review, Burton and colleagues found that with relatively little ultrasound-guided PIV access training, nurses, paramedics, and emergency technicians appear to successfully anticipate PIV access difficulty. The authors noted that 16 studies yielded an overall insertion success rate ranging from 76% to 99% while increasing first-attempt success and decreasing the number of punctures.
A study by Hansel and colleagues compared participants in an intervention group who received ultrasound-guided PIV insertion and a control group who received traditional visualization and palpation technique insertion. The authors found a 90% first-puncture attempt success rate in the intervention group vs 36% in the control group. No patients in the intervention group required more than three punctures. Patients in the control group were rescued by the ultrasound technique with successful first attempts. This study showed that the ultrasound-guided technique will more likely work on the first try and takes less time.
Similarly, a case-control and cross-sectional study conducted by Rodríguez-Herrera and colleagues, which compared standard and ultrasound-guided techniques, found a 76% first-attempt success rate with ultrasound compared to 16% using the standard technique.
Ultrasound-guidance training
In a systematic review of 35 articles, Hoskins and colleagues found that almost all training programs included mixed modalities (didactic online or in-person with simulation or hands-on sessions). Training duration ranged from 1.5 to 91.5 hours. Topics focused on principles of ultrasonography, identifying patients with DIVA, probe and image optimization, arm vascular anatomy, differentiating arteries from veins, principles of aseptic technique, Doppler color recognition, and machine operation. The mean reported insertion success rate was 83%, and the mean reported first-time insertion success rate was 76%. All studies indicated that the training correlated with improved procedural knowledge, confidence, and competence, which benefited providers and the health system.
Van Loon and colleagues noted the need for supervised hands-on live patient training. Their study found that first-attempt success rates significantly increased when participants gained competency, resulting in a lower failure rate per procedure. Consequently, the time needed to perform a PIV insertion decreased as nurses gained experience. It took an average of 34 procedures performed for nurses to become competent with ultrasound-guided PIV insertion.
Amick and colleagues conducted a simulation-based ultrasound-guided PIV training program to improve nurses’ insertion skills and confidence, especially when performing the procedure with hospitalized patients with DIVA. The researchers surveyed the nurses’ confidence and reported improved procedural skills and self-confidence post-training. In addition, the nurses achieved an overall insertion success rate of 90%.
Guidelines, standards,and evidence-based practices
According to the Infusion Nurses Society (INS) Infusion Therapy and Vascular Access Standards of Practice, vascular visualization technology, such as ultrasonography, minimizes the need for unnecessary and more invasive vascular devices, thereby reducing the risk of insertion-related and hospital-acquired complications. In addition to recommending an aseptic, non-touch technique to maintain asepsis for all invasive clinical procedures, the standards also call for escalating insertion to a more experienced colleague after two failed attempts. The standards recommend that healthcare organizations establish strategies for initiating PIV insertion in patients with DIVA.
A systematic review by Paterson and colleagues recommended the adoption of clinical practice guidelines and escalation pathways to improve clinical outcomes. According to Paterson and colleagues, guidance regarding the maximum number of attempts generally recommends escalation after two to three failed attempts, consistent with the INS standards.
Although most guidelines advocate using ultrasound guidance in patients with DIVA, limited standardization exists. Paterson and colleagues recommend establishing clinical practice guidelines and escalation pathways to improve clinical practice and patient care.
Our QI project
Our QI project took place in a large tertiary community medical center near Houston, Texas, between November 2023 and June 2024. The facility operates as a three-time Magnet®-recognized, Level II trauma, chest pain, and comprehensive stroke center. The project team included nurses from adult acute care and critical care, vascular nurses, central line-associated bloodstream infection (CLABSI) committee members, advanced practice providers, and professional development educators. Adult acute care nurses served as the target population for the project because they’re primarily responsible for accessing and inserting PIV lines.
The project aimed to answer the PICOT (Population, Intervention, Comparison, Outcome, Time) question: Among nurses in a tertiary community medical center (P), how do ultrasound-guided PIV catheter insertion training and establishment of practice guidelines for patients with DIVA (I), compared to current practice (C), affect nurses’ PIV catheter insertion skills efficiency and confidence (O), within 1 to 3 months (T)?
Design
The project’s primary goal was to decrease PIV insertion attempts among patients with DIVA. Interventions included training, developing clinical practice guidelines, and improving nurses’ PIV access skills and confidence. The project leader used pre- and post-implementation data to measure variables such as PIV insertion success rate, time of insertion, and nurse skills confidence.
CLABSI committee representatives, consisting of nurses from each acute care unit, met at least once a month to establish insertion guidelines. They reviewed the gap analysis information, INS standards, and evidence-based practice standards for PIV insertion. In addition, they worked to establish a consensus on recommended practice guidelines when caring for patients with DIVA.
The vascular nurse and the professional development educators used the INS guidelines to create content for the class and prepare didactic and hands-on skills training for nurses across all specialty areas. The hospital provided at least one to two training sessions per month, which allowed at least eight to 16 nurses to complete the training every month.
Pre-implementation
To measure variables such as the frequency of PIV attempts and time-to-I.V. access using visualization and palpation methods before implementing ultrasound-guided PIV catheter insertion training, the project leader collected quantitative data from adult acute care nurse participants using the Learning Self-Efficacy Scale (L-SES) before attending the training. No patient data were collected, and staff participation remained anonymous. (See Measurement instrument.)
Measurement instrument
To measure project outcomes and compare results before and after training implementation, the project team used the Learning Self-Efficacy Scale (L-SES). The 12-item Likert scale questionnaire was used with permission of Kang and colleagues, who developed the instrument.
The short well-developed, tested, and verified scale aids in understanding the relationship between students’ learning self-efficacy and clinical skills practice. Kang and colleagues define learning self-efficacy as the student’s confidence in their capability to learn specific subjects. The L-SES, which includes questions focusing on cognitive, affective, and psychomotor domains, can be applied to various clinical learning tasks by focusing questions on
targeted clinical skills. The project team used the following modified scale for the purposes of ultrasound-guided peripheral I.V. catheter insertion training assessment.
Implementation
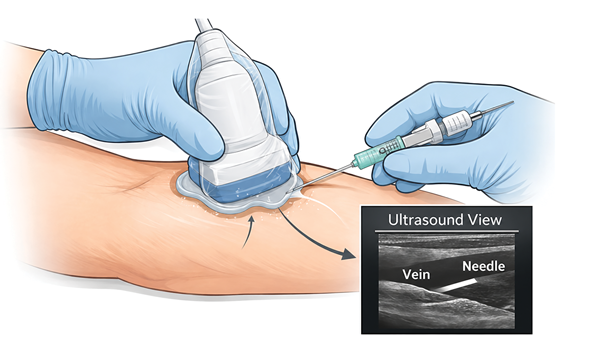
Nurses who completed the pre-intervention electronic survey attended the 4-hour ultrasound-guided PIV training program. A brief didactic lecture included discussion of ultrasound basics, identification of vascular structures, differentiation of arteries and veins, needle control, and probe guidance.
After the lecture, the trainer used arm manikins to demonstrate how to insert a PIV using ultrasound guidance. Nurses then performed a return demonstration. Participants received adequate time to practice hands-on skills. The trainer used a competency check-off form. The nurses completed at least three additional check-offs within 3 months on their units as witnessed by another ultrasound-trained nurse. After completion of all check-offs, the nurse submitted the competency form to the project leader for recording and tracking.
While the nurses participated in ultrasound-guided PIV insertion training, the project leader worked with the CLABSI committee and professional development team to create guidelines specifically for patients with DIVA. Evidence-based practice standards were adopted to develop the guidelines. Once guidelines were established, they were submitted to the hospital leadership for approval. After approval and publication of the guidelines, the professional development team provided organization-wide education.
Post-implementation
To gauge improvement in their PIV insertion efficiency, levels of confidence, and self-efficacy, nurses completed an electronic survey 1 to 3 months after finishing the training program.
The surveys measured the frequency of PIV attempts and time to successful I.V. access using ultrasonography. The project team evaluated the outcomes to assess improvement after establishing guidelines and providing training. (See Training outcomes: Pre- and post-assessment scores)
Training outcomes: Pre- and post-assessment scores
Descriptive statistics
Nurses who participated in the ultrasound-guided peripheral I.V. (PIV) insertion training completed pre- and post-implementation surveys to measure frequency of PIV attempts and time-to-I.V. access using visualization and palpation.
Pre-implementation descriptive statistics (n = 10)
hospital setting
Data collection
The QI project team measured pre- and post-intervention data quantitatively. For the nurses’ survey responses, the project leader used the paired t-test and p-values to measure, analyze, and compare the nurses’ level of confidence, frequency of attempts, and self-efficacy before and after training. The team stored data on a secure, HIPAA-compliant server accessible only to the project leader and used solely to evaluate project outcomes.
Results
Over the 3-month implementation period, 56 nurses enrolled in the ultrasound-guided PIV insertion training and agreed to complete the pre-survey. The project leader collected a total of 50 pre-implementation responses, 25 post-implementation responses with five duplicates, and 10 matched and valid responses.
The 10 matched and validated nurses’ demographics showed a range of ages and years of experience in the acute-care setting. The participants’ birth years ranged from 1977 to 1999, and their nursing experience ranged from 1 month to more than 16 years. Of the participants, eight out of ten stated that they hadn’t previously attended ultrasound-guided PIV insertion training.
Data analysis showed that the 10 nurses’ average confidence scores increased from 3.50 to 3.90 post-training and that the average number of attempts decreased from 1.60 to 1.30. Time for PIV insertion was measured in minutes and recorded from the beginning of vein assessment until the nurse left the patient’s room. Interestingly, the results showed an increase in the average insertion time from 9.50 to 12.75 minutes.
The project results based on the 10 matched and valid responses indicated that the nurses’ average self-efficacy domains improved, their level of confidence increased, the number of insertion attempts decreased; however, the insertion time increased. These results prompted the community hospital to continue implementing the newly established guidelines and the ultrasound training program.
Despite the slight increase in insertion time, the project allowed application of the aseptic non-touch technique to help prevent infection. Acute care nurses have become accustomed to the practice of attempting insertions only once and to call for an ultrasound-trained nurse after one failed attempt.
Implications for practice
The implementation of ultrasound-guided PIV catheter insertion training and the establishment of practice guidelines improved nurses’ confidence and efficiency in performing PIV insertions. Of the 10 nurses, eight stated that the use of ultrasound guidance increased the efficiency of peripheral I.V. insertion. Overall, the project outcomes aligned to enhance nurses’ skills and reduced the number of insertion attempts, which supported previous literature that highlighted the benefits of ultrasound guidance for patients with DIVA.
The project also promoted the application of newly established hospital guidelines, which limits the number of PIV insertion attempts, thus decreasing patients’ experiences of pain and discomfort. The increase in average insertion time may reflect nurses’ meticulous and strict adherence to the new aseptic non-touch technique rather than a loss of efficiency. This result showed consistency with a systematic review finding by Tada and colleagues that ultrasound guidance increases procedure time. The project leader predicts that as the nurses become more efficient and confident with ultrasound-guided PIV insertion, procedure time will decrease.
The training intervention, along with the established practice guidelines, proved effective in achieving its learning objectives within the 4-hour didactic and hands-on training timeframe. However, educators who provided the training should consider increasing the number of required hands-on check-offs and extending the number of hours to complete the training based on previous studies. According to Burton and colleagues and Hoskins and colleagues, ultrasound-guided PIV catheter insertion training ranged from 90 minutes to 91.5 hours. The required number of hands-on competency check-offs also ranged from 10 to 34. According to Van Loon and colleagues, nurses became competent with ultrasound-guided PIV insertion after performing an average of 34 procedures.
Implications for practice include maintaining the 4-hour didactic and hands-on training timeframe but increasing the number of competency hands-on check-offs to improve the nurses’ overall learning, self-efficacy, confidence, and PIV catheter insertion skill efficiency as well as to decrease PIV insertion procedure time. Unit leaders can continue to advocate for the availability of working ultrasound equipment at the bedside, and experienced nurses can serve as unit-based ultrasound champions, supporting their peers and supervising PIV insertion practice opportunities. In addition, leaders can encourage nurses to honestly assess their own PIV insertion skill competency and seek assistance from more experienced nurses as needed.
Improved efficiency and confidence
PIV catheter insertion in patients with DIVA may remain challenging, but this QI project showed a successful translation of evidence into practice through the provision of leadership support, interprofessional collaboration, education, skill development, and the creation of policies and guidelines in alignment with current standards of care. The project also supported the nurses’ mission to provide compassionate, ethical care and decrease patient pain, discomfort, and frustration resulting from multiple failed PIV insertion attempts. Ultimately, the project’s use of ultrasound guidance helped improve nurses’ PIV insertion skill efficiency and confidence—both vital attributes and components of healthcare service quality, productivity, performance, and customer and workforce satisfaction.
Anne Genevieve Papa-Torres is the professional development lead in clinical education and professional development at Memorial Hermann The Woodlands Medical Center in Shenandoah, Texas. Kimberly Parker is a clinical assistant professor at the University of Alabama in Tuscaloosa. Amy D. Lee is senior associate dean of academic affairs and a clinical professor at the University of Alabama Capstone College of Nursing. Heidi Gilroy is director of professional development, Magnet, and research at Memorial Hermann The Woodlands Medical Center.
American Nurse Journal. 2026; 21(7). Doi: 10.51256/ANJ072606
References
Abe-Doi M, Murayama R, Komiyama C, Tateishi R, Sanada H. Effectiveness of ultrasonography for peripheral catheter insertion and catheter failure prevention in visible and palpable veins. J Vasc Access. 2023;24(1):14-21. doi:10.1177/11297298211022078
Amick AE, Feinsmith SE, Davis EM, et al. Simulation-based mastery learning improves ultrasound-guided peripheral intravenous catheter insertion skills of practicing nurses. Simul Healthc. 2022;17(1):7-14. doi:10.1097/SIH.0000000000000545
Amick AE, Feinsmith SE, Sell J, et al. Ultrasound-guided peripheral intravenous catheter insertion training reduces use of midline catheters in hospitalized patients with difficult intravenous access. J Patient Saf. 2022;18(3):e697-703. doi:10.1097/PTS.0000000000000910
Bahl A, Johnson S, Alsbrooks K, Mares A, Gala S, Hoerauf K. Defining difficult intravenous access (DIVA): A systematic review. J Vasc Access. 2021;24(5):904-10. doi:10.1177/11297298211059648
Berlanga-Macías C, Díez-Fernández A, Martínez-Hortelano JA, et al. Ultrasound-guided versus traditional method for peripheral venous access: An umbrella review. BMC Nurs. 2022;21(1):307. doi:10.1186/s12912-022-01077-9
Burton SO, Donovan JK, Jones SL, Meadley BN. Can non-physician providers use ultrasound to aid in establishing peripheral IV access in patients who are difficult to cannulate? A scoping review. Prehosp Disaster Med. 2022;37(4):535-46. doi:10.1017/S1049023X22000796
Davis EM, Feinsmith S, Amick AE, et al. Difficult intravenous access in the emergency department: Performance and impact of ultrasound-guided IV insertion performed by nurses. Am J Emerg Med. 2020;46:539-44. doi:10.1016/j.ajem.2020.11.013
Hansel LA, Junges M, Santos MS, et al. UltraSound-guided PEripheral catheterization increases first-atTempt success RAte in hospitalized patients when compared with conventional technique: SPECTRA—Randomized clinical trial. J Vasc Access. 2024;25(5):1450-9. doi:10.1177/11297298231162132
Hoskins MJ, Nolan BC, Evans KL, Phillips B. Educating health professionals in ultrasound-guided peripheral intravenous cannulation: A systematic review of teaching methods, competence assessment, and patient outcomes. Medicine. 2023;102(16):e33624. doi:10.1097/MD.0000000000033624
Kang YN, Chang CH, Kao CC, Chen CY, Wu CC. Development of a short and universal learning self-efficacy scale for clinical skills. PLoS One. 2019;14(1):e0209155. doi:10.1371/journal.pone.0209155
Nickel B, Gorski L, Kleidon T, et al. Infusion therapy standards of practice, 9th edition. J Infus Nurs. 2024;47(1S suppl 1):S1-285. doi:10.1097/NAN.0000000000000532
Paterson RS, Schults JA, Slaughter E, et al. Peripheral intravenous catheter insertion in adult patients with difficult intravenous access: A systematic review of assessment instruments, clinical practice guidelines and escalation pathways. Emerg Med Australas. 2022;34(6):862-70. doi:10.1111/1742-6723.14069
Rodríguez-Herrera Á, Solaz-García Á, Mollá-Olmos E, et al. Use of the ultrasound technique as compared to the standard technique for the improvement of venous cannulation in patients with difficult access. Healthcare. 2022;10(2):261. doi:10.3390/healthcare10020261
Schuster C, Stahl B, Murray C, Glover K. Development and testing of an instrument to measure short peripheral catheter insertion confidence. J Infus Nurs. 2016;39(3):159-65. doi:10.1097/NAN.0000000000000166
Tada M, Yamada N, Matsumoto T, Takeda C, Furukawa TA, Watanabe N. Ultrasound guidance versus landmark method for peripheral venous cannulation in adults. Cochrane Database Syst Rev. 2022;12(12):CD013434. doi:10.1002/14651858.CD013434.pub2
Tran QK, Flanagan K, Fairchild M, Yardi I, Pourmand A. Nurses and efficacy of ultrasound-guided versus traditional venous access: A systematic review and meta-analysis. J Emerg Nurs. 2022;48(2):145-58. doi:10.1016/j.jen.2021.12.003
Tuomela K, Abiye Agbeh, Anibaba F, et al. The rounds efficiency index: A novel physics-based construct for patient- and family-centered rounds. Hosp Pediatr. 2024;14(7):584-91. doi:10.1542/hpeds.2022-006971
Van Loon FH, Scholten HJ, Korsten HH, Dierick-van Daele AT, Bouwman AR. The learning curve for ultrasound-guided peripheral intravenous cannulation in adults: A multicenter study. Med Ultrason. 2022;24(2):188-05. doi:10.11152/mu-3322
Key words: peripheral intravenous catheter insertion, cannulation, ultrasound