This dual diagnosis poses challenges for patients—and their nurses.
Takeaways:
- Adults with chronic medical illness have a high prevalence of co-morbid depression.
- Depression often goes undiagnosed, leading to worsening health outcomes.
- Nurses are in key positions to advocate for screening and implementing evidence-based interventions for depression in patients with co-morbid medical illnesses.
MAJOR depressive disorder (MDD) affects more than 16 million adults in the United States each year and is a leading cause of disability for individuals ages 15 to 44. (See Facts and figures.) In middle-aged and older adults, depression becomes less prevalent, but a greater likelihood exists that it will become a chronic condition accompanied by other chronic health issues. Depression can negatively impact patients’ medical comorbidities and reduce quality and length of life. Although patients with chronic medical conditions are three times more likely to suffer from depression than those without other chronic health issues, depression assessment frequently is overlooked.
When nurses and healthcare providers understand depression’s etiology, symptoms, treatment options, and relationship with other chronic diseases and conditions, they’re better positioned to proactively help patients with this dual diagnosis.
Facts and Figures
Did you know…
- depression can develop at any age, but the median age at onset is around 32 years.
- depression is more prevalent in women (8.5%) than in men (4.8%).
- many individuals with major depressive disorder have poor health, a low socioeconomic status, impaired social relationships, and diminished functioning at work and home.
- approximately 35% of adults with depression aren’t being treated.
- untreated depression increases the lifetime risk for suicide—estimates range from 2.2% to 15%.
Sources: Chow et al, 2019; National Institute of Mental Health, 2019
Etiology
 Depression can be attributed to multiple mechanisms—monoamine deficiency, inflammation, hypothalamicpituitary-adrenal (HPA) axis, and genetics—but it’s still poorly understood.
Depression can be attributed to multiple mechanisms—monoamine deficiency, inflammation, hypothalamicpituitary-adrenal (HPA) axis, and genetics—but it’s still poorly understood.
Monoamine deficiency
Discoveries in the 1950s suggested that depression may be caused by monoamine deficiency. Patients taking the antihypertensive medication reserpine (which prevents neuron receptors from taking up mono a mines such as serotonin, norepinephrine, dopamine, and histamine) were becoming severely depressed. Around the same time, researchers found that depressed patients treated with isoniazid for tuberculosis experienced a reduction in depressive symptoms. Isoniazid inhibits the enzyme mono amine oxidase that breaks down monoamine neurotransmitters. These findings led to developing pharmacologic depression treatments focused on increasing monoamine levels.
However, further research suggests that patients with depression may not have a monoamine deficiency because not all patients with depression respond to antidepressants that increase monoamines. Continued exploration has led to the rejection of the simple monoamine hypothesis in favor of complex interrelationships between neurotransmitter systems that lead to depression.
Inflammation
More recent evidence suggests that patients with MDD have high levels of pro-inflammatory cytokines and receptors, in addition to high levels of acute-phase reactants and chemokines. This theory is supported by research demonstrating that 30% to 50% of patients with hepatitis C who were being treated with inflammatory cytokines (interferon alpha) developed depression. However, because not all patients with depression have elevated levels of pro-inflammatory cytokines and not all patients with an inflammatory response experience relief from their depressive symptoms with anti-inflammatory agents, researchers suggest that a subgroup of patients may develop depression due to inflammation.
HPA activity
Depression also has been attributed to alterations in the regulation of hormones through the HPA axis. Early trauma and chronic stress lead to increased HPA activity, resulting in elevated cortisol levels that have been associated with depression. Research suggests that up to half of individuals experiencing a major life stressor develop depression.
Genetics
The relationship between genetics and depression is widely accepted. Twin studies and other research related to heritability have demonstrated that if one parent has a mood disorder the child has a 10% to 25% risk of developing one. This risk increases to 50% if both parents have a mood disorder. Additionally, research supports the hypo thesis that changes in genes due to environmental influences such as adverse childhood events and other environmental stress
Symptoms
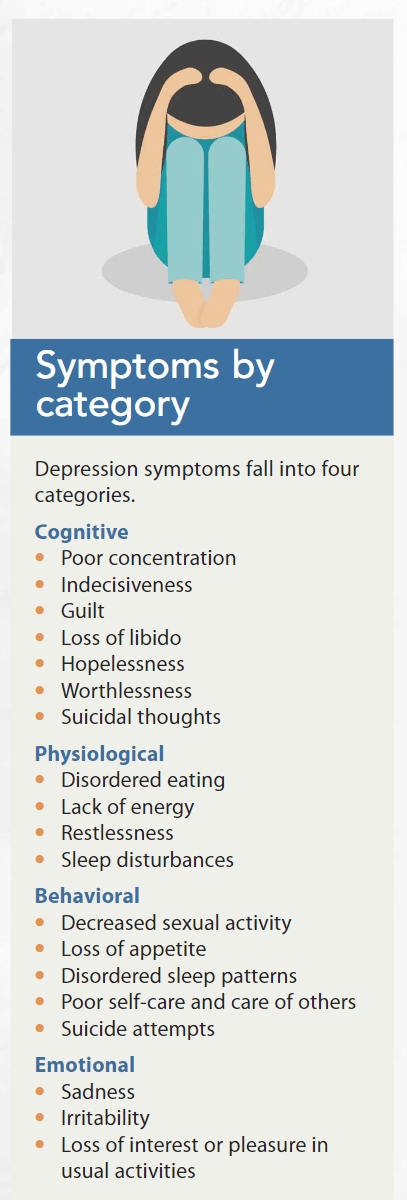
Symptoms of depression vary among individuals. (See Symptoms by category.) For example, one patient may overeat while another may eat very little or one patient may experience insomnia while another sleeps most of the day. In addition, some patients may appear depressed based on facial expression while some severely depressed patients present a cheerful front. Determining the likelihood of depression without conducting formal screening and assessment can lead to underdiagnosis.
Screening and diagnosis
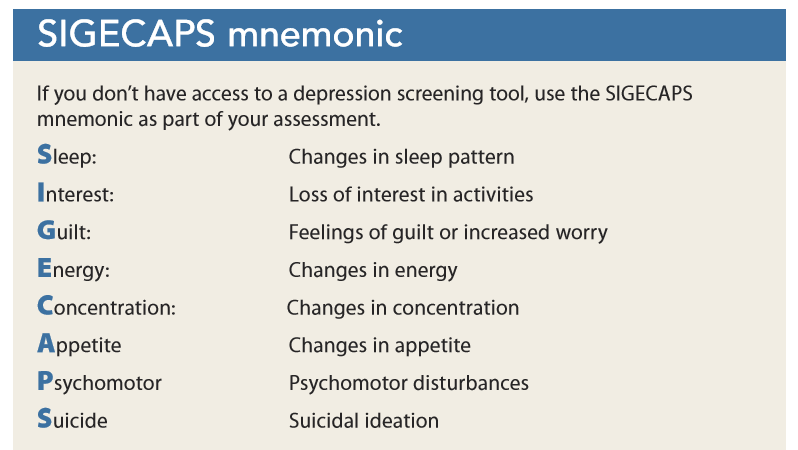
The U.S. Preventive Services Task Force (USPSTF) recommends screening for depression in all adults, including pregnant and postpartum women. This often starts with a self-report screening tool such as the Patient Health Questionnaire-2 (PHQ-2) or Patient Health Questionnaire-9 (PHQ-9). The benefit of the PHQ-2 is that it’s fast, but the PHQ-9 is highly sensitive and specific in detecting symptom severity. For example, a positive response to item nine “Thoughts that you would be better off dead, or of hurting yourself in some way” is associated with an increased risk of suicide. Further evaluation is needed for any positive screen and particularly for patients who report thoughts of death or self-harm. If you don’t have access to a screening tool, use the SIGECAPS mnemonic. (See SIGECAPS mnemonic.)
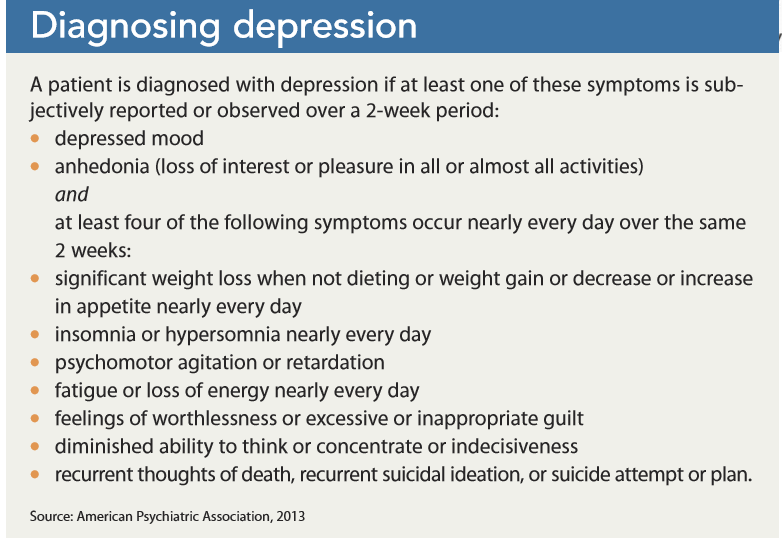
A diagnosis of MDD is established based on the patient meeting criteria identified in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). MDD also is referred to as “clinical depression” and is a separate diagnosis from other mood disorders such as disruptive mood dysregulation disorder, premenstrual dysphoric dis order, dysthymia, and depression due to substance or medication use. (See Diagnosing depression.)
Chronic illnesses and depression
Chronic illnesses and conditions— such as cardiovascular disease, diabetes, and chronic pain—are the leading cause of death and disability in the United States. The number of adults with two or more chronic conditions is rising and accounts for 87% of hospitalizations for patients 65 years and older.
Cardiovascular disease
The correlation between heart disease and depression is well-documented. It’s been attributed to the dysregulation of the autonomic system, abnormalities in serotonin metabolism, and HPA axis stimulation. Adults with depression have a 64% greater risk of developing cardiovascular disease and 59% have an increased likelihood of having a cardiac event. For patients without a history of depression, the presence of cardiovascular disease raises their risk for depression 20% to 30%. Clinical trials are underway to investigate the impact of depression treatment on cardiovascular disease prevention. Evidence of the link between depression and cardiovascular disease is so strong that the American Heart Association has called for early intervention in treating adolescents with mood disorders to prevent cardiovascular disease.
Diabetes
Studies suggest a bidirectional relationship between depression and diabetes. Data indicate that patients with type 2 diabetes have twice the risk for depression compared to the general population; those with type 1 diabetes have a three times greater risk. HPA axis theories for depression support this relationship as do factors such as socioeconomic status, lack of exercise, and poor diet. Individuals with type 1 diabetes, which typically develops in childhood, have significant disruptions to their daily life to manage their illness, increasing the risk for depression. In turn, individuals with depression have an increased risk for developing type 2 diabetes because of reduced physical activity, poor dietary habits, and side effects of some depression medications.
Chronic pain
Chronic illnesses such as rheumatoid arthritis, osteoarthritis, degenerative disc disease, multiple sclerosis, and spinal cord injuries cause pain and limit mobility. This affects a patient’s ability to perform activities of daily living and participate in social activities, important factors in reducing depression risk. Chronic pain can cause insufficient sleep, leading to daytime somnolence, fatigue, and further withdrawal from pleasurable activities. Depression can affect a patient’s motivation and energy to engage in health-promoting activities, which a vicious downward spiral. Approximately 85% of patients with chronic pain experience severe depression. In addition, a patient’s awareness that his or her condition won’t improve can lead to hopelessness, a major risk factor for suicide.
Treating depression
Evidence-based guidelines for treating MDD recommend collaborative care. For mild to moderate MDD, patients should be offered either psychotherapy or pharmacotherapy based on patient preference and individual factors. For moderate to severe MDD, a combination of pharmacotherapy and psychotherapy is superior to monotherapy.
Lack of access to qualified psychotherapists, especially in rural and underserved areas, can be a barrier to treatment. Sufficient evidence exists to recommend computer-based cognitive behavioral therapy (CBT), which can be offered as adjunctive or first-line treatment.
For severe MDD, electroconvulsive therapy has strong evidence to support its use. Little evidence supports repetitive transcranial magnetic stimulation, vagus nerve stimulation, or deep brain stimulation.
Psychotherapy
 Many types of evidence-based psychotherapy are available to treat depression, including CBT, problem-solving therapy (PST), and interpersonal psychotherapy (IPT).
Many types of evidence-based psychotherapy are available to treat depression, including CBT, problem-solving therapy (PST), and interpersonal psychotherapy (IPT).
CBT. This collaborative, problemsolving approach, which typically is offered in six to 14 sessions, is one of the most widely used therapies for treating depression. According to the cognitive-behavioral model, one’s thoughts about a situation can affect emotional and behavioral responses to it. When a patient is depressed, his or her thoughts about a situation are distorted, resulting in unpleasant emotions and maladaptive behaviors. By using CBT techniques, such as a thought record, the patient learns to change thought patterns commonly found in depression.
In a thought record, the patient records details of a distressing event or situation and identifies associated automatic thoughts and emotions related to the event along with his or her actions. An individual may be unaware of an automatic thought (such as “It’s my fault”) but very aware of the emotion associated with it. Automatic thoughts stem from the patient’s rigid self-perceptions (such as being unlovable, worthless, and helpless). In weekly CBT sessions, the patient learns to develop more balanced thinking patterns and to view situations more realistically. With daily practice, the patient’s mood and response to situations improve as he or she develops positive thoughts and behaviors. Homework between sessions promotes practice of newly learned skills. CBT tools and worksheets, found in the public domain, can be used for homework and reviewed in each session. In addition, CBT applications for mobile devices offer options for recording thoughts and activities and monitoring mood.
Behavioral activation (BA) is a specific CBT skill. Patients with depression tend to withdraw from hobbies, activities, and social engagements they previously enjoyed. With BA, patients become regularly engaged in activities that give them the greatest level of pleasure and mastery. Patients identify goals and values and schedule enjoyable and meaningful activities throughout the week. As they engage in these activities, they rate their level of pleasure and mastery along with their depression level. As mastery and pleasure increase, mood improves, new behavior is reinforced, and activity participation increases.
PST. PST is a form of CBT that focuses on improving the patient’s ability to cope with stressful life events. The premise of PST is that depressive symptoms are the consequences of ineffective coping. Patients learn new problem-solving skills over four to 12 sessions to help them better manage future stressful events without experiencing the negative consequences caused by maladaptive coping.
IPT. The goal of IPT is to improve interpersonal relationships and social functioning. This structured therapy occurs over 12 to 16 weeks and starts with an assessment of the patient’s relationship patterns, capacity for intimacy, and current relationships. Therapy sessions then focus on issues with current relationships.
Psychopharmacology
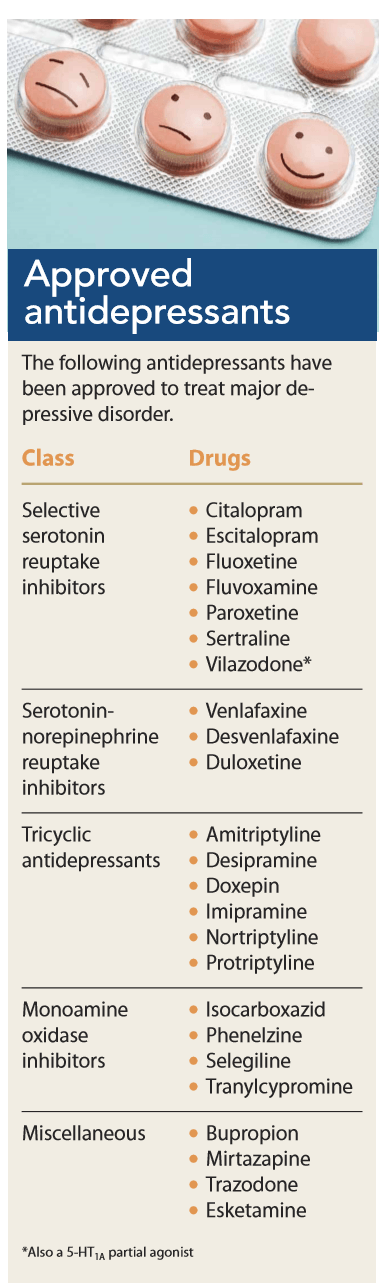
Antidepressants are in the top three medication classes prescribed in the United States. They include selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), and monoamine oxidase inhibitors (MAOIs). Other available antidepressants include trazodone, mirtazapine, bupropion, and esketamine. (See Approved antidepressants.)
In addition to treating depression, these medications are used to treat anxiety and as an augmented strategy for treating chronic pain. The specific antidepressant class and drug are selected based on patient characteristics, co-occurring conditions, patient preference, and cost.
Treating depression in individuals with chronic medical illnesses poses treatment challenges because of drug-drug and drug-disease interactions as well as renal and hepatic impairment. Also, medications prescribed to treat the various comorbidities (such as beta-blockers, corticosteroids, benzodiazepines, and hormones) may contribute to depressive symptoms.
A challenge with all patients is promoting drug adherence. Patients may not take their medications as prescribed for a variety of reasons, including concern about potential side effects, cost, perceived benefits, and complex treatment regimens. Patients who are depressed are less likely to take their medications (because of lack of motivation, fatigue, trouble concentrating, and a sense of worthlessness), creating treatment challenges for both their depression and comorbid medical conditions.
SSRIs. Before SSRIs, only patients with severe MDD were treated with antidepressants because of intolerable side effects such as somnolence, hyper- and hypotension, arrhythmia, weight gain, and sexual dysfunction. The safety and low side effect profile of SSRIs and SNRIs made treating depression in primary care practices possible.

Serotonin is an important neurotransmitter that aids in regulating mood and social behavior, appetite and digestion, sleep, memory, and sexual desire and function. SSRIs increase the level of serotonin at the synaptic cleft. (See How SSRIs regulate serotonin.)
Side effects vary within this class, but the most common are GI upset, sexual dysfunction, emotional blunting, and changes in energy level. Caution is advised in elderly patients because SSRIs can cause hyponatremia and GI bleeding; citalopram causes QTc prolongation.
SNRIs. These first-line medications for treating depression are recommended for patients with fatigue or pain. SNRIs inhibit the reuptake of serotonin and norepinephrine. Side effects are similar to SSRIs except for venlafaxine and desvenlafaxine, which can cause hypertension.
TCAs. This class of antidepressants (among the earliest used) increases norepinephrine and serotonin levels by inhibiting reuptake. However, TCAs affect other neurotransmitters neurotransmitters, which can cause sedation, postural hypotension, blurred vision, weight gain, dry mouth, and constipation. TCAs are lethal if more than the prescribed dose is taken, so extreme caution should be used when prescribing them to patients with depression. They’re most often used in the primary care setting to treat neuropathic pain.
MAOIs. This was the first class of antidepressants. These drugs increase levels of norepinephrine, serotonin, and dopamine by inhibiting the enzyme monoamine oxidase to effect changes in cells and circuits that have been impacted by depression. Multiple side effects and drugdrug interactions plus drug-food interactions limit these drugs to use in patients with refractory depression.
Patients taking MAOIs should avoid foods that are high in tyramine, such as aged cheese, beer, red wine, and cured or smoked meats. Patients taking MAOIs not only should be aware of the potential for drug-drug interactions with prescription drugs but also should avoid over-the-counter products that contain ephedrine.
Other antidepressants. Three other antidepressants frequently used because of their ability to treat depression and other health issues are trazodone, mirtazapine, and bupropion.
Trazodone, a serotonin antagonist and reuptake inhibitor, has sedating properties and has replaced benzodiazepines as a sleep aid because of its lack of addictive potential. At high doses, trazodone exerts an antidepressant effect, but low doses typically are prescribed for use at bedtime to promote sleep.
Mirtazapine is used as an augmenting agent because it doesn’t impact monoamine reuptake and can work synergistically with SSRIs or SNRIs. At low doses, mirtazapine causes sedation and increases appetite, so it’s frequently prescribed for elderly patients with sleep disturbances and anorexia.
Bupropion is a norepinephrine dopamine reuptake inhibitor approved for depression and smoking cessation. The benefit of bupropion is that it causes fewer sexual side effects compared to other antidepressants, it isn’t sedating, and it’s considered a weight-neutral drug. Bupropion lowers the seizure threshold, so it shouldn’t be prescribed to patients with a seizure disorder or those at risk for seizures.
In 2019, esketamine, a noncompetitive N-methyl D-aspartate receptor antagonist, was approved to treat severe treatment-resistant depression. Esketamine is delivered via nasal spray. Because of potential side effects of sedation, nausea, and dissociation, the medication must be taken within the clinical setting and can be prescribed only by providers who have received additional training in its use.
Nurses at the forefront
When depression is undetected and untreated, mental and physical health can deteriorate. However, nurses have many opportunities to address mental health in inpatient and outpatient settings. For example, if the electronic health record doesn’t have a screening tool for depression as part of the standard admission process, advocate through shared governance structures to include it.
Nurses also have an opportunity to reduce the stigma around mental healthcare. Screening for depression, providing evidence-based education, and making referrals to mental health specialists and community resources should be routine components of your nursing care. When stigma around mental health is reduced, patients may be more likely to seek help, which can improve health outcomes and quality of life.
The authors work at Texas Tech University Health Science Center in Lubbock. Susan J. Calloway is a professor, Rosalinda Jimenez is an assistant professor, and Dianne Lavin is an associate professor.
Selected references
American Association of Suicidology. Depression and Suicide Risk. 2014. suicidology.org/portals/14/docs/resources/factsheets/2011/depressionsuicide2014.pdf
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. Washington, DC: American Psychiatric Association; 2013.
B descu SV, T taru C, Kobylinska L, et al. The association between diabetes mellitus and depression. J Med Life. 2016;9(2):120-5.
Chow W, Doane MJ, Sheehan J, Alphs L, Le H. Economic burden among patients with major depressive disorder: An analysis of healthcare resource use, work productivity, and direct and indirect costs by depression severity. Am J Manag Care. February 14, 2019. ajmc.com/journals/supplement/2019/economic-burden-mdd-analysis-healthcare/economic-burden-mdd
Department of Veterans Affairs, Department of Defense. VA/DoD Clinical Practice Guideline for the Management of Major Depressive Disorder. 2016. www.healthquality.va.gov/guidelines/MH/mdd/VADoDMDDCPGFINAL82916.pdf
Goldstein BI, Carnethon MR, Matthews KA, et al. Major depressive disorder and bipolar disorder predispose youth to accelerated atherosclerosis and early cardiovascular disease: A scientific statement from the American Heart Association. Circulation. 2015; 132(10):965-86.
Herman JP, McKlveen JM, Ghosal S, et al. Regulation of the hypothalamic-pituitaryadrenocortical stress response. Compr Physiol. 2016:6(2):603-21.
Katon WJ. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin Neurosci. 2011;13(1):7-23.
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-13.
Liu B, Liu J, Wang M, Zhang Y, Li L. From serotonin to neuroplasticity: Evolvement of theories for major depressive disorder. Front Cell Neurosci. 2017;11:305.
Miller AH, Raison CL. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat Rev Immunol. 2016;16(1), 22-34.
National Institute of Mental Health. Major depression. February 2019. nimh.nih.gov/health/statistics/major-depression.shtml
Pratt LA, Brody DJ, Gu Q. Antidepressant Use in Persons Aged 12 and Over: United States, 2005–2008: NCHS Data Brief, no. 76. Hyattsville, MD: National Center for Health Statistics; 2011. cdc.gov/nchs/data/databriefs/db76.pdf
Rathbone AL, Clarry L, Prescott J. Assessing the efficacy of mobile health apps using the basic principles of cognitive behavioral therapy: Systematic review. J Med Internet Res. 2017;19(11):e399.
Shadrina M, Bondarenko EA, Slominsky PA. Genetics factors in major depression disease. Front Psychiatry. 2018;9:334.
Siu AL, US Preventive Services Task Force (USPSTF), et al. Screening for depression in adults: US Preventive Services Task Force Recommendation Statement. JAMA 2016; 315(4):380-7.
Sheng J, Liu S, Wang Y, Cui R, Zhang X. The link between depression and chronic pain: Neural mechanisms in the brain. Neural Plast. 2017:9724371.
Stahl SM. Prescriber’s Guide: Stahl’s Essential Psychopharmacology. 6th ed. New York: Cambridge University Press; 2017.
Steiner CA, Barrett ML, Weiss AJ, Andrews RM. Trends and Projections in Hospital Stays for Adults with Multiple Chronic Conditions, 2003–2014: Statistical Brief #183. Rockville, MD: Agency for Healthcare Research and Quality; November 2014. ncbi.nlm.nih.gov/books/NBK264314
Stewart JC, Rollman BL. Optimizing approaches to addressing depression in cardiac patients: A comment on O’Neil et al. Ann Behav Med. 2014;48(2):142-4.
Wenzel A, Dobson KS, Hays PA. Cognitive Behavioral Therapy Techniques and Strategies. Washington, DC: American Psychological Association; 2016.

















2 Comments.
Although medication can relieve the symptoms of depression, it is not usually suitable for long-term use. Other treatments, including exercise and therapy, can be just as effective as medication, often even more so, but don’t come with unwanted side effects. If you do decide to try medication, remember that medication works best when you make healthy lifestyle changes as well.
Depression treatment is a way to find a solution for someone you love. Although major depressive disorders are treatable by medication, sometimes it is not enough.