Takeaways:
- Pain assessment in older adults is best guided by a systematic framework, such as the Hierarchy of Pain Assessment.
- Nonpharmacologic treatment strategies are equally as important as analgesic medication in a comprehensive pain management plan.
- Nonpharmacologic strategies can enhance pain relief but also can reduce potential side effects and adverse effects that frequently accompany pain medications.
CNE
1.75 contact Hours
Learning Objectives
- Identify strategies for overcoming challenges related to pain assessment in older adults.
- Discuss five steps for assessing pain in older adults.
- Describe nonpharmacologic options for pain management in older adults.
The authors and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit.
Expiration: 12/1/23
Accurately assessing and detecting acute or chronic pain in older adults (65 years and older) is challenging, especially if they have difficulty recognizing, interpreting, and communicating their pain experience. Assessment using best practices is the critical first step in developing and implementing an effective treatment plan in any care setting.
The American Society for Pain Management Nursing recommends taking a step-by-step hierarchical assessment approach and identifying and advocating for the safest management approaches with the fewest side effects. Many nonpharmacologic strategies are accessible, inexpensive, easy to use, and reduce the need for high-risk medications, such as opioids and nonsteroidal anti-inflammatory drugs (NSAIDs).
This article provides practical guidance for addressing common challenges in pain assessment, reviews the hierarchy of pain assessment, and integrates nonpharmacologic strategies into a comprehensive treatment plan.
Pain assessment challenges and strategies
Practical strategies are available to mitigate three common challenges associated with pain assessment in older adults—pain source identification, time limitations, and communication barriers—and facilitate the process.
Challenge 1: Pain source identification
One of the first challenges is identifying the source of pain, particularly in the presence of multimorbidity, and developing a treatment plan that addresses different types of pain. Multiple diagnoses and pain conditions may increase the experience of pain, worsen severity and intensity, and affect normal function.
Strategy: Knowing a patient’s chronic health diagnoses will facilitate early recognition of the possible pain source. The source of pain also may help determine the best nonpharmacologic treatment option. For example, patients with longstanding diabetes are prone to developing painful diabetic neuropathy.
Challenge 2: Time limitations
Pain assessment is a priority similar to vital signs and diagnostic tests because pain can deter the healing process. Nurses should conduct a focused pain assessment per their organization’s policy and patient’s need. However, time constraints can pose challenges, especially during public health emergencies, such as the COVID-19 pandemic.
Strategy: Different settings provide opportunities for nurses to contribute to pain assessment and treatment decision-making despite time limitations. For example, patients or the family caregiver can complete some elements of the assessment before the healthcare visit. These elements are then communicated to the provider and discussed during the visit as appropriate to the care setting and available resources. In a primary care setting, older adults can complete pain intensity and function tools in the waiting room with the nurse or by using a tablet with direct data entry options.
Challenge 3: Communication barriers
Communication barriers can impede transparency, timely nurse assessment, and patient pain reports. Several factors (including language, cognitive, sensory, and physical impairments) influence patient communication, and every effort should be made to maximize patient-nurse communication. (See How to maximize patient communication.)
How to maximize patient communication
Communication is a significant pain assessment challenge. Consider these strategies to overcome it.
- Develop rapport and trust with patients.
- Determine the patient’s beliefs related to talking about pain. For example, ask patients if they feel comfortable discussing pain. If not, explore their reasons and discuss why it’s important to share their pain experience.
- Assess pain during your initial interaction with the patient, then collaboratively establish a method for pain assessment, including how often and when pain is assessed while maintaining organization policies.
- Ascertain pain terminology typically used by the patient and use these lay descriptors throughout your pain assessment and management.
- Use open-ended questions to ask about pain directly. For example, ask, “How would you describe your pain right now?” Don’t use general questions, such as “How are you doing,” for pain assessment.
- Ensure the patient understands that reporting pain isn’t considered “complaining” or “griping.”
- If the patient has a documented pain diagnosis, such as osteoarthritis, but seems reluctant to answer a general pain question, ask about specific locations of pain.
- Ensure patient privacy during pain assessments, but also ask which family members or caregivers can be involved in the process and what pain information can be shared with them.
- Educate patients about pain and medical terminology.
Strategy: A patient-centered approach emphasizes patient autonomy, integrates patient preferences into the pain assessment process, and respects sociocultural practices. For example, provide pain intensity scale options for older patients to choose from, and ensure they all address communication barriers and demonstrate reliability in self-reporting pain. If your organization’s pain assessment policy doesn’t include pain scale options that are reliable and valid in older adults (including those with cognitive impairment), advocate for policy changes. Maximizing communication also requires attention to nonverbal cues, such as facial expressions, body movements, and navigation of environmental and personal space (such as holding on to objects when walking).
Assessment best practices
If best practices don’t drive pain assessment and treatment in older adults, care may be inadequate, resulting in suffering; loss of function and independence; and the psychological triad of depression, anxiety, and sleep disturbances. The Hierarchy of Pain Assessment Techniques is a five-step framework to guide pain assessment in older adults who can’t self-report.
To ensure a clinically useful and aligned assessment, we’ve modified these techniques for use in cognitively intact older adults by combining steps two through five of the hierarchy with the Clinically Aligned Pain Assessment (CAPA). The CAPA tool assesses five key areas: comfort (pain tolerability), pain change, pain control, function, and sleep. The role of this modified hierarchy is to expand the completeness of evidence-based pain assessment beyond simplistic ratings to identify key information that older adults may not report but are important in determining the presence and impact of pain and developing a treatment plan. (See Hierarchy of pain assessment in cognitively intact older adults.)
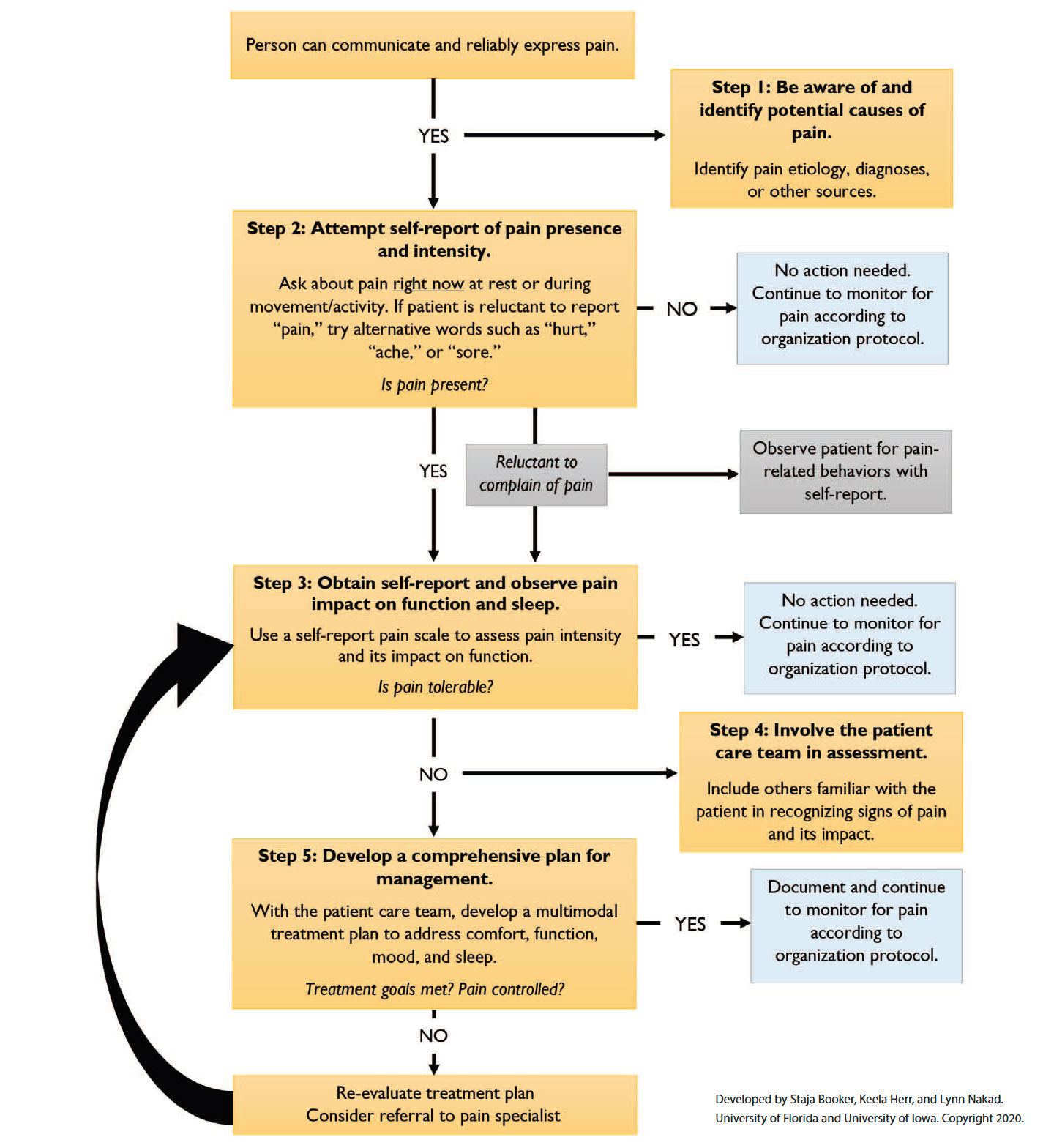
Hierarchy of pain management in cognitively intact older adults
This pain assessment hierarchy combines a hierarchy for nonverbal and cognitively impaired older adults (65 years and older) with the Clinically Aligned Pain Assessment to help overcome challenges nurses may encounter when evaluating pain in cognitively intact older adults.
Step 1: Be aware of/identify potential causes of pain
Older adults may deny pain or hesitate to report its characteristics because of fear, stoicism, or a belief that pain is normal as we age and so not a priority. Be vigilant for diagnoses and conditions known to be painful. A patient’s medical history, physical examination, diagnostic tests, laboratory values, and medication history may provide evidence of potential or current pain etiology. Older adults with multimorbidity may have several sources or locations of pain.
Musculoskeletal disorders, such as arthritis, osteoporosis, and fractures, are common sources of pain for older adults. Other causes include inflammation, infections (urinary tract infections, pneumonia), bladder distention, kidney stones, skin breakdown, gout, peripheral vascular disease, and constipation. If the patient can point to the pain location, examine for signs of infection or injury, including redness, heat, and swelling or other deformity. In older adults, physiological indicators (sweating, elevated vital signs) may be blunted even in acute pain and are not good indicators of acute or chronic pain.
Pain management is improved when the cause is known, but in some cases the etiology may not be identified, even in the presence of acute pain. This is consistent with the new definition of pain from the International Association for the Study of Pain: “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.” Chronic pain may not be associated with a recognizable disease process, so providers shouldn’t delay treatment until a diagnosis is made. They should, however, attempt to determine whether pain symptoms are nociceptive, neuropathic, or mixed/nociplastic to develop a comprehensive management plan. (See Pain types.)
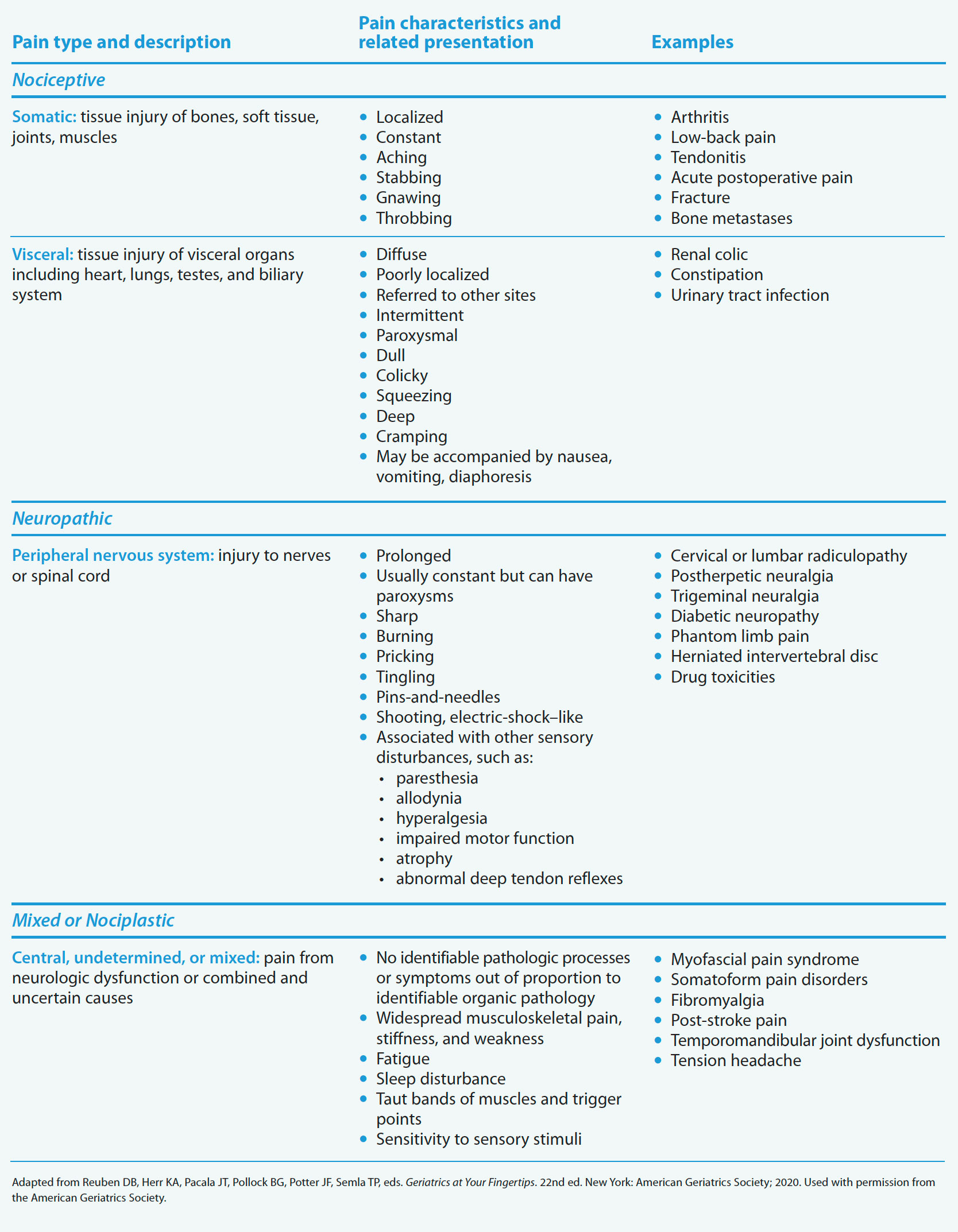
Pain types
Understanding the type of pain (nociceptive, neuropathic, mixed or nociplastic) a patient is experiencing will help determine the best treatment plan.
Use these strategies to identify causes and potential sources of pain:
- Review relevant medical records to identify any procedure, disease process (physical or emotional), acute issues, indwelling medical device (for example, urinary catheter, chest tube), or trauma that may be triggering pain.
- Be aware of atypical presentations of acute pain conditions. For example, older adults experiencing a myocardial infarction may report abdominal pain; chest pain as “pressure”; or exhibit restlessness, confusion, and fatigue.
- Ask the patient to point to the pain location on a human figure drawing or on themselves.
- Observe the patient’s response during routine care activities (such as repositioning and dressing), which may indicate the presence and location of pain.
Step 2: Attempt self-report of pain presence and intensity
Pain, as defined by Margo McCaffery, MS, RN-BC, FAAN, is a subjective experience that’s best identified via a patient’s self-report. However, because many older patients, regardless of cognitive status, under-report pain, self-reports may be limited or compromised (in terms of reliability). In patients who are under sedation or who have cognitive impairment, advanced dementia, delirium, intellectual disability, or stroke, self-reports may be unobtainable. The issue isn’t only if an older patient can complete a self-report measure, but also if their self-report is reliable and accurate.
Self-report is more than pain intensity; a comprehensive pain assessment should consider the elements of pain (intensity, location, duration, quality), as well as related factors—how does pain affect function, what makes pain better or worse, current and past treatments, and what works well to relieve pain. Emerging evidence suggests that pain intensity tools alone (which have never been a recommended nursing best practice) are inadequate at capturing the pain experience or guiding analgesic treatment. Current practice recommends establishing a dynamic approach as standard of care, including assessing pain during movement (turning, dressing, walking, standing) and evaluating the impact of pain on function and activity.
Nurses must be consistent (and sometimes persistent) and use evidence-based techniques to identify the presence of pain in older adults. First, ask the simple question: “Are you hurting anywhere?” Or ask a more specific question when a documented health condition is associated with pain: “Do you have pain in your knees right now?” Then use a brief validated assessment tool (such as the Functional Pain Scale; the Pain intensity, Engagement, and General Activity Scale; or the Defense and Veterans Pain Rating Scale) to quantify pain intensity and impact. Recommended pain intensity scales (such as a numeric rating scale or the Iowa Pain Thermometer-Revised) should be used in combination with a measure of pain impact or interference with function and activities. Consistently use the same validated tools to score, document, and monitor changes in pain, tolerability, and functional improvement over time. (See Choosing the right self-report pain tool.)
Choosing the right self-report pain tool
Use these tips when selecting a self-report pain tool to assess older adult patients.
- Adopt validated pain intensity tools with different formats to accommodate the needs of diverse patients. The tools should
- be congruent with the patient’s culture of pain expression, use accurate language, and be available in different languages (or easily translated)
- accommodate a patient’s developmental, intellectual, and cognitive level (easily understood and reliable)
- accommodate a patient’s sensory impairments (available in Braille, audio, or large and dark print)
- Involve the patient in choosing a self-report tool. Document any preference and use that tool consistently.
In addition, find tools that
- are scientifically valid, reliable, and practical
- are easy to print or reproduce electronically
- are easily disinfected if laminated or disposable after each patient use
- are easily and quickly explained to the patient or observer
- are easy to use, score, and record consistently
- are appropriate for an interdisciplinary healthcare team
- can be linked to a patient’s comfort, function, and mood goals
- meet organization and regulatory body standards
- can be used to obtain data for quality-improvement and evidence-based practice projects.
In addition to selecting appropriate pain assessment tools, practical strategies to optimize obtaining an accurate self-report include the following:
- Keep instructions simple and clear, and repeat them if necessary.
- Give the patient adequate time to assimilate pain questions and answer, and don’t interrupt.
- Reduce any overstimulating and extraneous noises to help the patient focus, process, and answer questions.
- Provide examples of pain intensity (for example, a splinter may be rated 3/10, a broken hip could be rated 7/10) only if the patient is having difficulty perceiving and communicating pain or asks for clarification and examples.
- Obtain pain self-reports when the older adult is most alert and lucid.
- Older adults may have poor recall memory, so ask about pain in the present tense, using phrases such as “right now,” “current pain,” or “at this moment.”
Step 3: Self-report and observation of pain impact on function and sleep
In addition to a patient’s self-report of function and interference with activities, use observation to determine baseline ability and the effect of pain on engagement in physical activities and sleep. The original Hierarchy of Pain Assessment Techniques focused observations on pain behaviors in cognitively impaired individuals. However, identifying and understanding behaviors even in those who can self-report may support a more comprehensive assessment and act as another metric to assess pain increases and decreases.
Because impaired sleep significantly impacts the pain experience and quality of life, sleep should be assessed routinely, using options such as “awake with pain most of the night,” “awake with occasional pain,” or “normal sleep.” Research shows that people who experience sleep disturbances (trouble falling and staying asleep) and low-quality sleep report more chronic pain. Work with patients to determine the best timing for pain assessments and interventions to use before sleep.
Step 4: Involve the patient care team in assessment
Care team members—including the patient, selected family and significant others, caregivers, and other healthcare providers (physical therapist, nursing assistant/patient care technician, social worker, physician)—are familiar with the patient’s normal behavior and activity level, so can help identify subtle changes that may otherwise go unnoticed or overt changes that may indicate pain.
Unlicensed personnel, such as nursing assistants and patient care technicians, may have a limited role in evaluating pain, but they can provide useful information about when pain most often occurs, which activities are more painful for the patient, and changes in activity or mood that may be due to suspected or reported pain. Unlicensed personnel may require training to screen for pain or use pain scales, with follow-up assessments by nurses or providers.
Family and personal caregivers can provide information about a patient’s pain behaviors, mood disposition, communication patterns, and functional status. They also can provide information about how the patient typically manages pain, which may help when developing an individualized treatment plan, especially for rehabilitation therapy. Suggest that patients and caregivers keep a pain diary to record pain characteristics (intensity, location and duration of pain, time of day pain is noted, pain at rest or during movement). This may require teaching caregivers key observations—such as patient behavior, function, and mood—to note if they suspect the patient is experiencing pain.
Step 5: Develop a comprehensive plan for management
In the original Hierarchy of Pain Assessment Techniques, the fifth step uses an analgesic trial to validate pain in cognitively impaired older adults and confirm questions about their behaviors. However, in cognitively intact older adults who are able to report their pain, validating pain presence with an analgesic isn’t needed and developing a comprehensive management plan can proceed.
A comprehensive plan is guided by a patient’s goals and preferences for care, considers pharmacologic and nonpharmacologic approaches based on the patient’s unique needs, and weighs risks and benefits of treatment options. When pain is identified, work with the patient and provider to establish attainable goals for continued comfort, function, and sleep (or other patient-preferred outcomes such as mood). Evaluate changes in pain and pain control according to CAPA: Is the pain getting worse, about the same, or is it getting better? How effective is pain control? Is pain control inadequate, partially effective, effective (just about right), or fully effective (would like to reduce medication or use nonpharmacologic interventions)?
New best practice reports recommend nonpharmacologic strategies as a primary intervention that should be considered first and early given the low risk of adverse effects and the evidence of risks associated with opioids, NSAIDs, and adjuvants. Other resources provide guidance on analgesic interventions for older adults; this article focuses on nonpharmacologic strategies.
Pain management using nonpharmacologic interventions
Managing pain has always been a complex task but is even more challenging as healthcare providers attempt to mitigate opioid misuse. Biological, social, and psychological factors contribute to chronic pain, so treatment should be integrative and individualized to improve pain control, function, activities of daily living, and quality of life. The benefits of many nonpharmacologic strategies include accessibility, low cost, ease of use, and few side effects. Evaluate patients for contraindications to select nonpharmacologic interventions; for example, avoid or limit the use of heat/cold therapies in older adults with neuropathy, pressure injuries, or venous or arterial ulcers.
According to a recent U.S. Department of Health and Human Services report, pain management best practices are broadly categorized as medications, interventional (minimally invasive or invasive) procedures, restorative therapies, behavioral health approaches, and complementary and integrative health (CIH). (See Hierarchy of multi-modal pain management.) This article describes restorative, behavioral health, and CIH approaches; however, they may not be readily available for every patient, particularly behavioral and CIH therapies.
Hierarchy of multimodal pain management
Consider this multimodal approach to pain assessment and treatment in older adults.
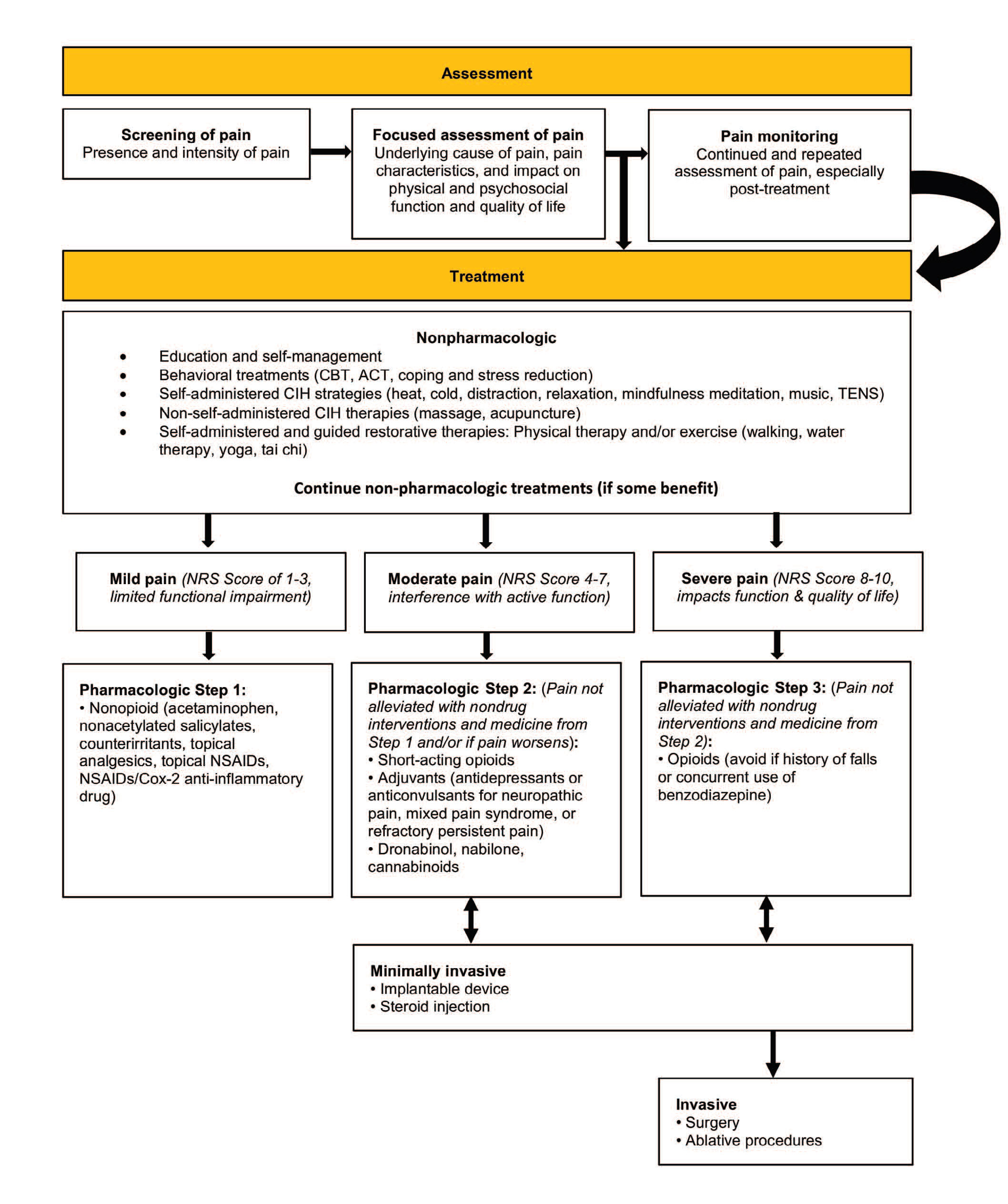
Restorative therapies include therapeutic exercise, transcutaneous electric nerve stimulation, massage therapy, traction, cold and heat, therapeutic ultrasound, and bracing. Behavioral health interventions include behavioral therapy, cognitive behavioral therapy (CBT), acceptance and commitment therapy, mindfulness-based stress reduction (MBSR), emotional awareness and expression therapy, and self-regulatory or psychophysiological approaches (biofeedback, relaxation training, hypnotherapy). CIH approaches include acupuncture, manipulative therapies, MBSR, yoga, tai chi, and spirituality.
Evidence on noninvasive, nonpharmacologic therapies for chronic pain (including low back pain, neck pain, osteoarthritis, and tension headaches) commonly seen in older patients is variable. Interventions with the strongest support for consistently improving function and reducing pain include regular exercise (walking, tai chi, yoga), multidisciplinary rehabilitation, acupuncture, massage, heat, music, and mind-body practices (CBT, imagery with progressive muscle relaxation, mindfulness practices). Some interventions haven’t had extensive testing with older adults, but that doesn’t mean they’re not effective. More research is needed.
Before selecting a nonpharmacologic regimen, providers should consider the patient’s underlying co-morbidities, physical ability, cognitive status, preferences, access (for example, tai chi classes may be limited in a rural community), and evidence of effectiveness. An intervention may need to be tailored to the individual older adult. For example, select cognitive-based therapies (guided imagery, reminiscence) carefully; older adults with any level of cognitive or intellectual disability may not be able to use them because of issues related to attention/focus, memory, and understanding.
Work with patients to shape their expectations for treatment and provide education about available strategies. Other strategies include the following:
- Target the nonpharmacologic treatment based on its mechanism of action and the pain problem.
- Assess pain immediately before and again after administering nonpharmacologic interventions, when the intervention is expected to have an effect.
- Determine what nonpharmacologic treatments are used at home to manage pain.
- Use a pain bundle, or offer the patient a comfort menu. Pain bundles typically include CIH strategies, structured pain rounds, pharmacologic treatments, pain assessment tools, and education.
- Engage patients and caregivers in education and intervention use.
Take a multimodal approach
A multimodal assessment and treatment approach provides the best pain management for older adults. Follow current practice to standardize pain management, meet regulatory requirements for quality care, maintain a strong skill set, and use good clinical judgment to help relieve patients’ pain. (See Resources.) More research and quality improvement projects can further refine best practices to meet older adults’ needs. AN
Resources
Tap into these resources to learn more about pain management in older adults and to ensure you’re following best practices.
| Guidelines | Assessment
Management—Pharmacology
Management—Disease specific
|
| Reports |
|
| Websites |
|
Staja Q. Booker is an assistant professor at the University of Florida College of Nursing in Gainesville. Lynn Nakad is a research assistant and PhD student at the University of Iowa College of Nursing in Iowa City. Keela A. Herr is the Kelting Professor in Nursing and co-director of the Csomay Center for Gerontological Excellence at the University of Iowa College of Nursing.
References
American Geriatrics Society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674-94.
Arnstein P, Gentile D, Wilson M. Validating the functional pain scale for hospitalized adults. Pain Manag Nurs. 2019;20(5):418-24.
Arnstein P, Herr K. Shifting focus: From the opioid crisis to quality pain management. J Gerontol Nurs. 2019;45(6):3-5.
Booker SQ, Haedtke C. Assessing pain in verbal older adults. Nursing. 2016;46(2):65-8.
Booker SQ, Herr KA. Assessment and measurement of pain in adults in later life. Clin Geriatr Med. 2016;32(4):677-92.
Bruckenthal P, Marino MA, Snelling L. Complementary and integrative therapies for persistent pain management in older adults: A review. J Gerontol Nurs. 2016;42(12):40-8.
Herr K, Coyne PJ, Ely E, Gélinas C, Manworren, RCB. Pain assessment in the patient unable to self-report: Clinical practice recommendations in support of the ASPMN 2019 position statement. Pain Manag Nurs. 2019;20(5):404-17.
Miaskowski C, Blyth F, Nicosia F, et al. A biopsychosocial model of chronic pain for older adults. Pain Med. 2020;21(9):1793-1805.
Nakad L, Booker S, Gilbertson-White S, Shaw CA, Chi N-C, Herr K. Pain and multimorbidity in late life. Curr Epidemiol Rep. 2020;7:1-8.
Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain. 2020. Online ahead of print.
Schofield P. The assessment of pain in older people: UK national guidelines. Age Ageing. 2018;47(suppl 1):i1-22.
Skelly AC, Chou R, Dettori JR, et al. Noninvasive Non-pharmacological Treatment for Chronic Pain: A Systematic Review Update. Comparative Effectiveness Review No. 227. Agency for Healthcare Research and Quality. April 2020. effectivehealthcare.ahrq.gov/sites/default/
files/pdf/noninvasive-nonpharm-pain-update.pdf
Topham D, Drew D. Quality improvement project:
Replacing the numeric rating scale with a Clinically Aligned Pain Assessment (CAPA) tool. Pain Manag Nurs. 2017;18(6):363-71.
U.S. Department of Health and Human Services. Pain Management Best Practices Inter-Agency Task Force Report: Updates, Gaps, Inconsistencies, and Recommendations. May 9, 2019. hhs.gov/sites/default/files/pmtf-final-report-2019-05-23.pdf