
Suffering—it’s a powerful word that evokes a visceral response. Actually, patient means “one who suffers” in Latin. To reduce patient suffering, we need to consider the experience of nurses and other caregivers, because patient experience and nurse engagement are inextricably tied. Measuring the met and unmet needs of both patients and caregivers is critical for addressing those needs and driving improvement and value in healthcare.
The patient experience
Medical advances, cutting-edge technology, and regulatory requirements arguably have led to better care. But they’ve also resulted in a highly task-driven, checklist-oriented healthcare environment that decreases our acknowledgement of the patient’s true experience—clinical, operational, cultural, and behavioral.
Patient suffering has multiple layers, which we can better understand in terms of the sources of suffering.
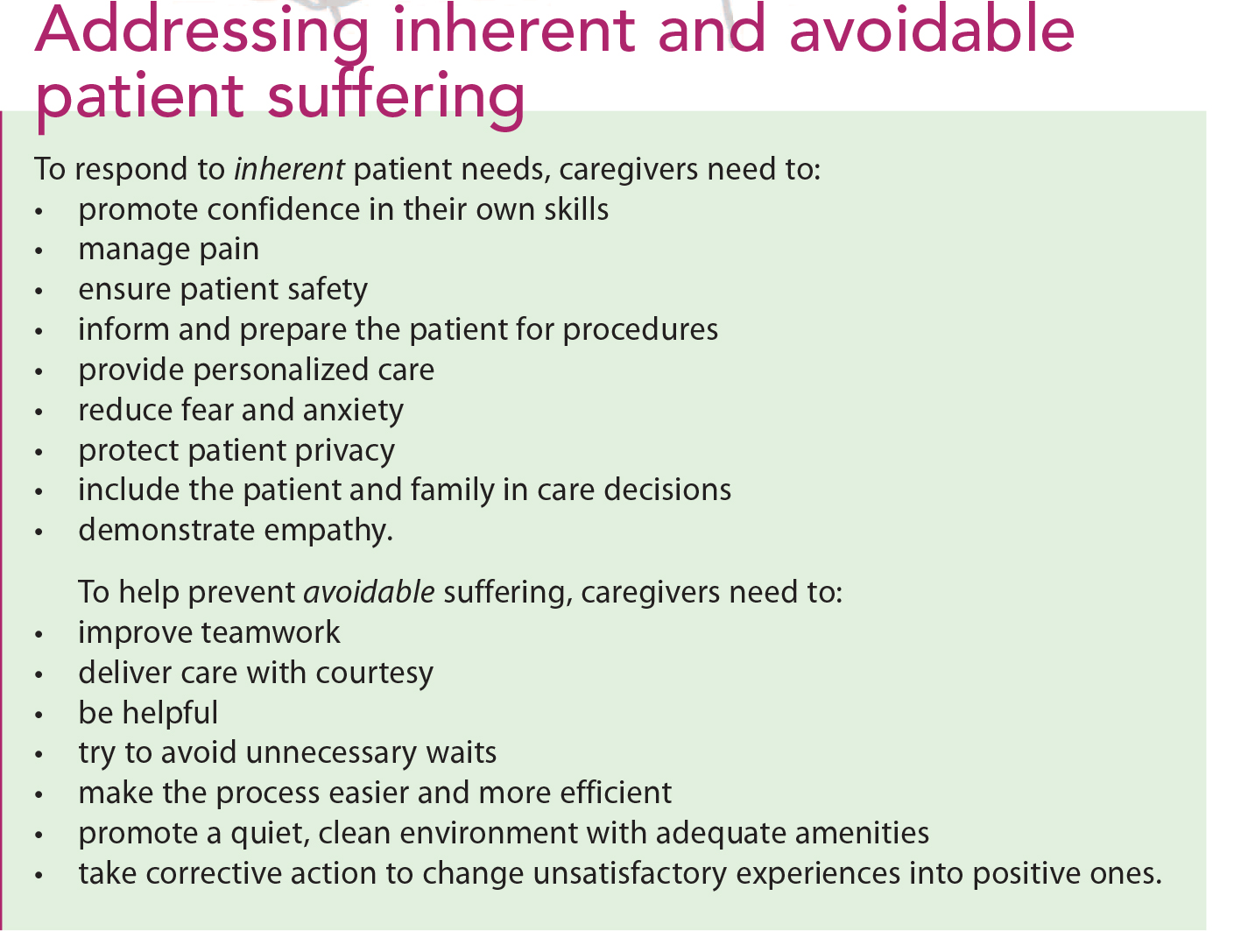
• Inherent suffering arises directly from a medical diagnosis or the treatment the diagnosis requires. For example, a patient with cancer may experience pain, appetite loss, skin problems, and emotional distress due to the cancer diagnosis. Inherent suffering also can stem from treatment; surgery, for instance, can be painful and frightening and may necessitate rehabilitation. So even if health care were perfect, patients inevitably would suffer. As caregivers, we may be able to mitigate suffering but we can’t eliminate it altogether.
• Avoidable suffering occurs because health care isn’t perfect. During the course of a patient’s diagnosis and treatment, if we make the patient wait, fail to work well together as a team, or don’t provide an environment conducive to healing, we’re imposing suffering on the very person who has come to us for care. Simply mitigating this avoidable suffering isn’t enough; we must prevent it.
We can measure the extent to which we reduce patient suffering by understanding the degree to which we meet our patients’ needs. Attributes of the patient experience can be organized around the patient needs they reflect. These needs can be organized further based on the type of suffering they predominantly reflect. (See Addressing inherent and avoidable patient suffering.)
Framework for compassionate care
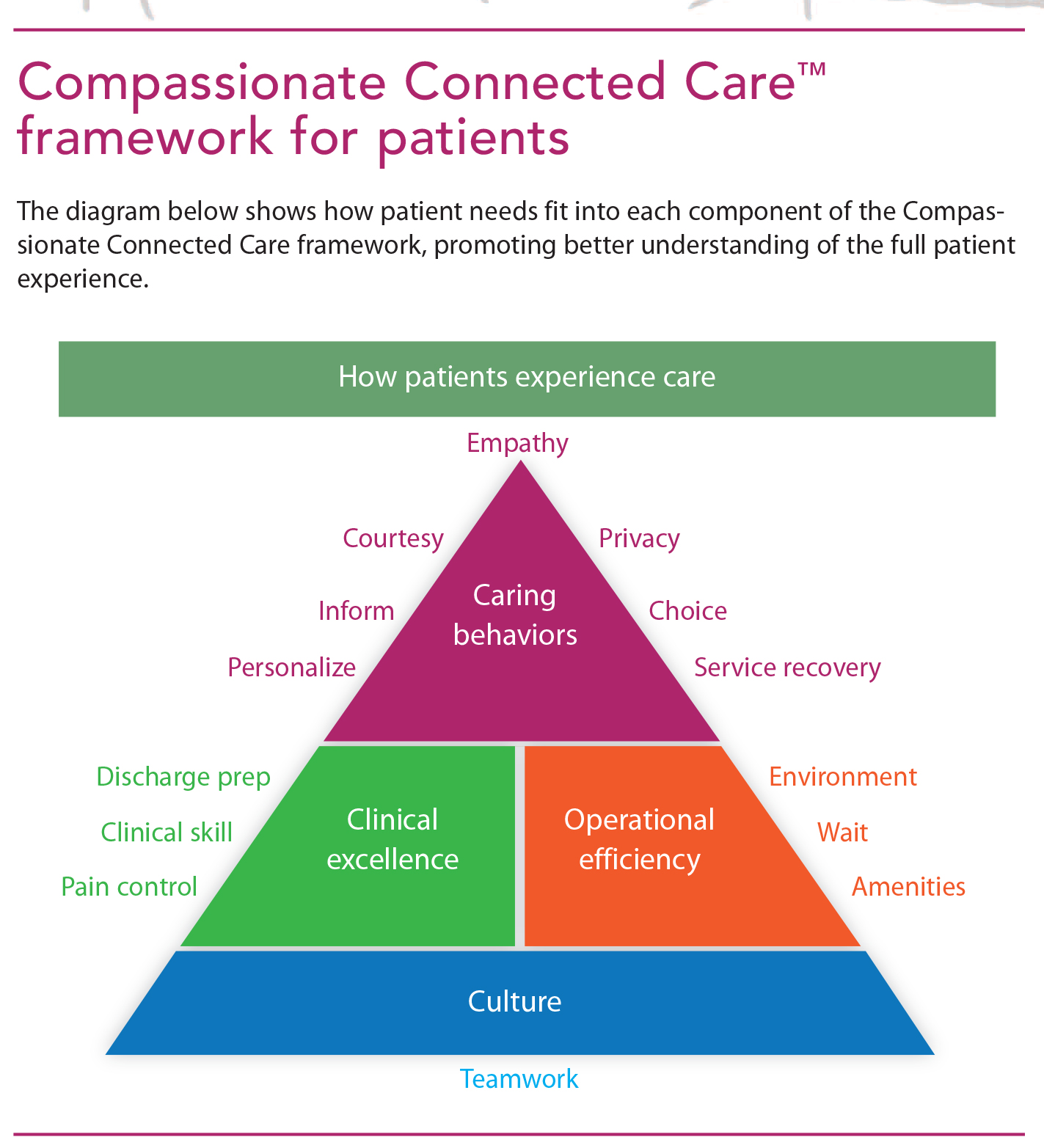
Understanding that patients suffer and measuring their suffering is just the beginning. To address suffering, we must embrace the totality of the patient experience. The Compassionate Connected Care™ framework addresses the challenges of reducing suffering by integrating clinical, operational, cultural, and behavioral aspects of care to provide the best possible patient experience in any setting. This framework identifies specific action items that help nurses and other caregivers achieve the greatest impact in reducing suffering.
The four Compassionate Connected Care domains link clinical excellence with outcomes, operational efficiency with quality, caring behaviors with action, and the organization’s mission, vision, and values with engagement. This construct addresses the causes of suffering with specific preventive measures in each category to improve the patient experience, confronting potential areas of dysfunction with tangible actions. (See Compassionate Connected Care framework for patients.)
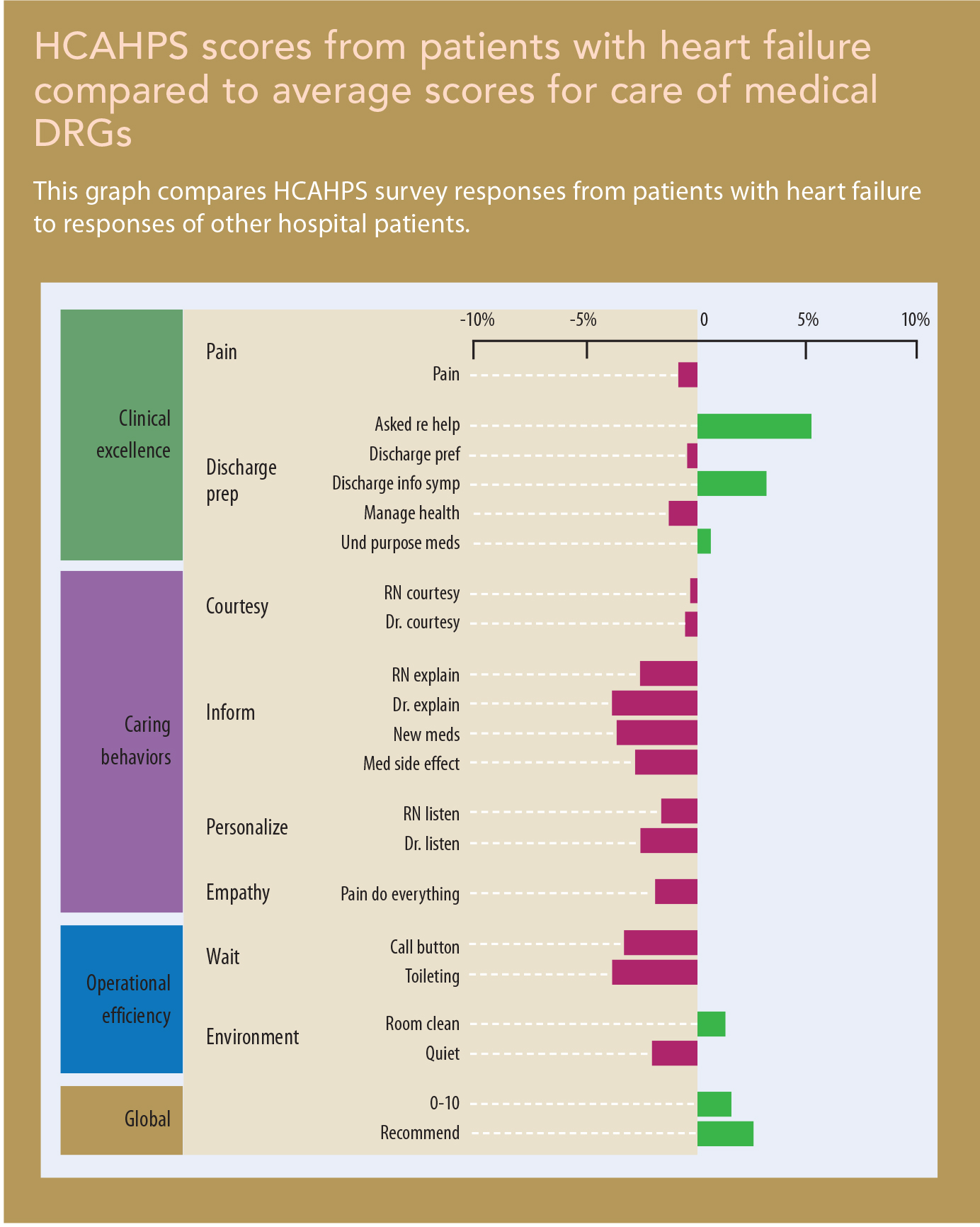
Responding to patient needs may warrant redesigning elements of care rather than simply layering service behaviors atop clinical processes. Data show patient needs vary by disease state or medical condition; the way care is provided must address these unique differences. For example, patients with heart failure perceive care differently than does the more global cohort of all medically treated patients. This may seem intuitive, but data paint a picture that helps focus improvement efforts on what matters to a specific patient population.
HCAHPS scores from patients with heart failure compared to average scores for care of medical DRGs shows that patients with heart failure are more likely (green bars) to rate elements of their hospital stay with a “top-box” (most positive) evaluation on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. Specifically, they’re more likely to give the hospital a 9 or 10 rating and to recommend it to others. They also have more favorable opinions on certain elements of discharge planning. However, this graph shows these patients need more information about their medications and care at home than do others, as well as more help in toileting and greater responsiveness when they press their call lights. Understanding data related to specific patient segments allows us to both acknowledge and address their unique needs.
Six themes
The Compassionate Connected Care framework uses six themes that help focus effort and understanding on what’s important to patients and to guide improvement. These themes were developed by using an affinity diagram process representing the responses of 117 clinicians, nonclinicians, and patients. Participants were asked to describe what compassionate and connected care meant to them. Responses were distilled into the following themes:
- Acknowledge suffering. We should acknowledge our patients are suffering and show them we understand.
- Body language matters. Nonverbal communication skills are as important as the words we use.
- Anxiety is suffering. Anxiety and uncertainty are negative outcomes that must be addressed.
- Coordinate care. We should show patients that their care is coordinated and continuous and that we are always there for them.
- Caring transcends diagnosis. Real caring goes beyond delivering interventions.
- Autonomy reduces suffering. It helps preserve patient dignity.
Caregiver experience
While nurses may not suffer the same way patients do, we experience pain, frustration, lack of resources, and many other forms of suffering when delivering care to patients and their families. In our highly regulated healthcare environment, administrators commonly view nursing as the highest cost center instead of a revenue generator. Typically, nursing is factored into room and board on the patient’s bill.
However, nurses arguably have the biggest impact on the patient experience because we’re more accessible to patients than other clinicians during hospitalization. Yet 15 of every 100 nurses are disengaged, defined as an engagement level at least one standard deviation below the mean on the Press Ganey employee engagement database. Conservative estimates suggest each disengaged nurse costs an organization $22,200 in revenue related to lost productivity. For a hospital with 100 nurses, this equates to $333,000 yearly. For a large system with, say, 15,000 nurses, potential loss skyrockets to $50 million.
Declining nurse engagement over time
Lack of engagement ultimately influences nurse retention. In 2014, the average turnover rate for nurses was 16.4%, according to the 2015 National Healthcare Retention & RN Staffing Report. The survey found the cost of turnover for a bedside registered nurse (RN) averaged $36,900 to $57,300, leading to a loss of $4.9 to $7.6 million for the average hospital. Overall, nursing turnover costs U.S. hospitals billions of dollars each year.
On average, RN engagement is relatively high—4.11 on a 5-point scale in the Press Ganey database. But data also show the most engaged nurses have been with the organization less than 6 months. This may reflect the “honeymoon effect” widely cited in employee research, or it may reflect more significant issues of employee empowerment, work design, or leadership. Whatever the cause, nurses’ dwindling engagement over time affects retention at the 2- to 5-year mark and leads to churn in the nursing workforce. Generational differences also account for more mobility and thus more volatility in the structure and stability of the nursing department in healthcare facilities.
What’s more, engagement data suggest that the further the nurse works from the bedside, the more engaged she or he is. Thus, nurses providing direct patient care ar among the least engaged. Considering the emphasis on patient-centered care and the known relationship between patient experience and engagement, this finding is troubling.
Compassionate Connected Care for the caregiver
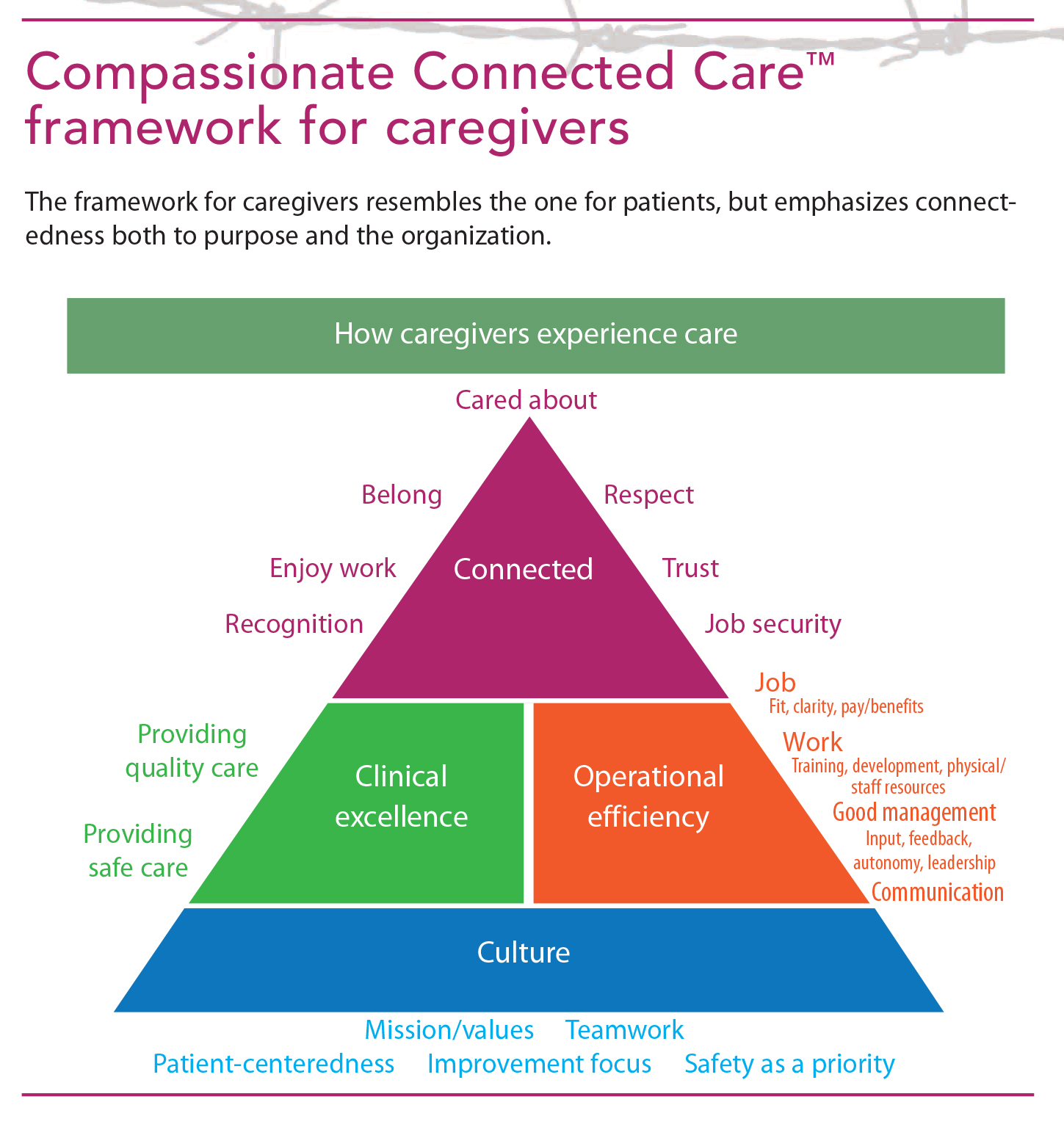
Like patients, caregivers also have measurable met and unmet needs. Like the Compassionate Connected Care framework for patients, the framework for the caregiver describes the caregiver experience as multidimensional. This model contains several parallel structures to the patient model in terms of clinical excellence, operational excellence, and emphasis on culture. (See Compassionate Connected Care framework for caregivers.) Specifically measuring each of these components and comparing them to the average performance across all measures in the model provides a view of the data that helps organizations focus their efforts in areas that matter to caregivers.
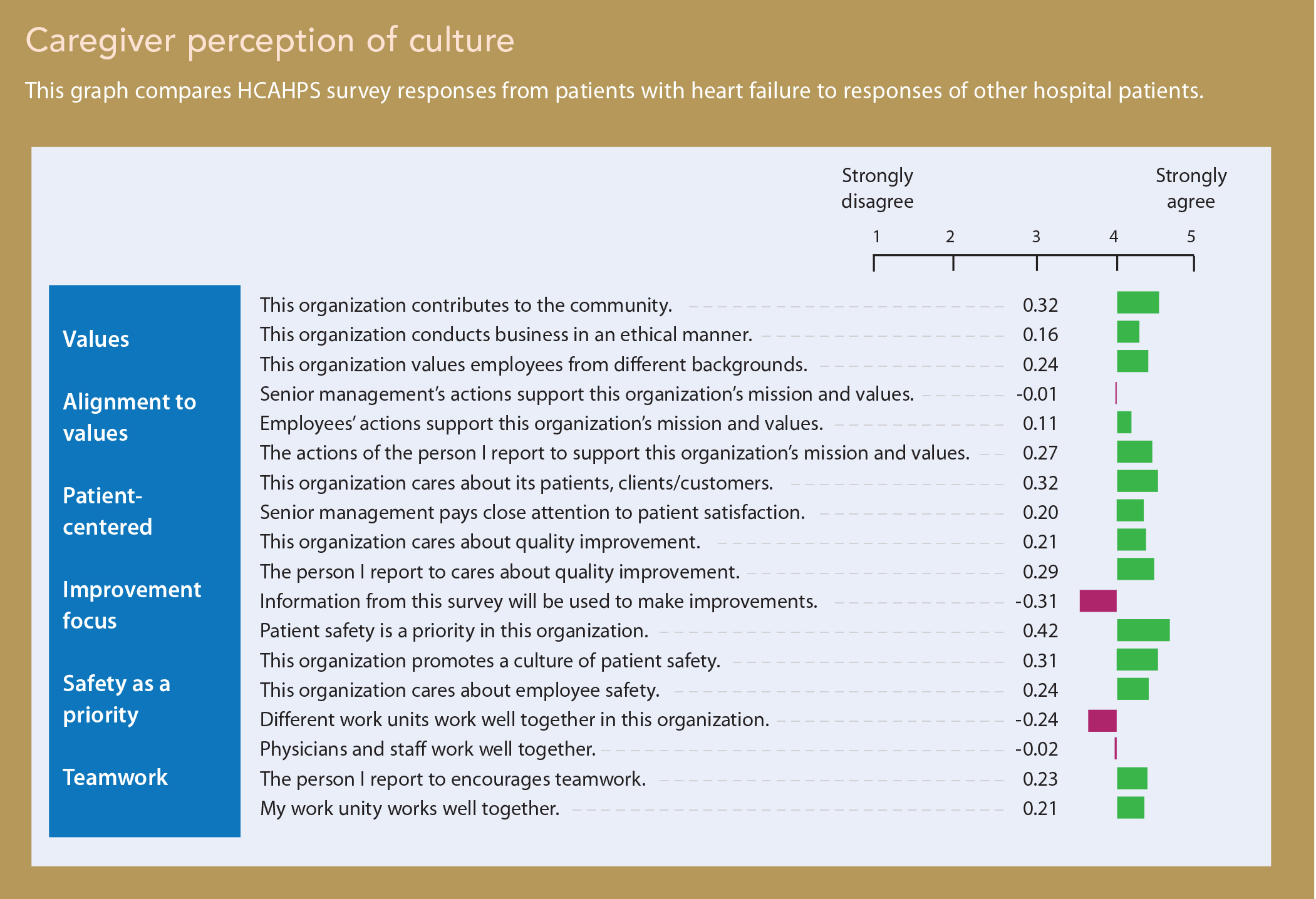
The data in Caregiver perception of culture show that caregivers evaluate cultural measures more positively than the average across all engagement measures. But several opportunities are apparent where elements of culture fall below the all-measures average, including teamwork across units and between physicians and nursing staff.
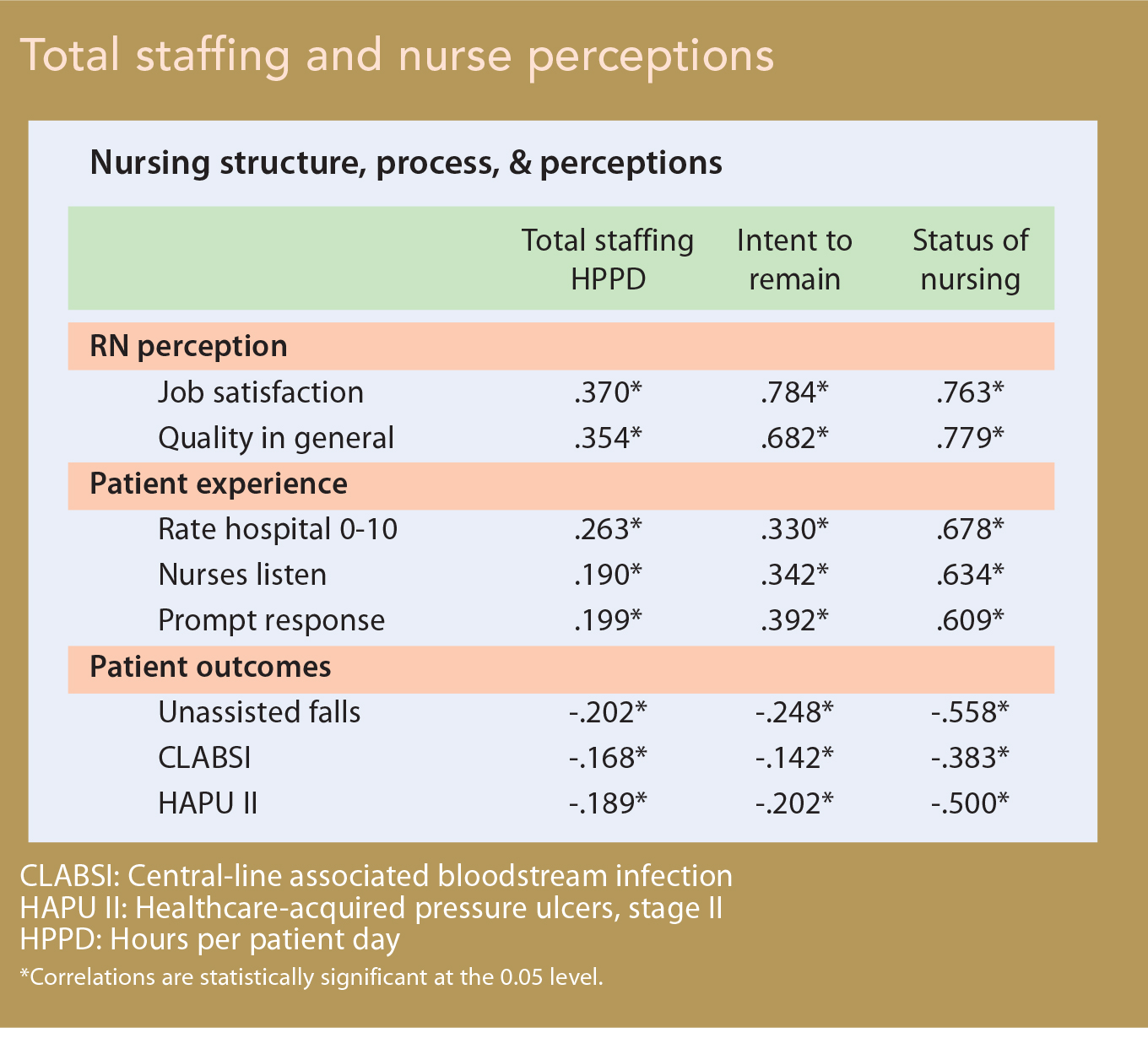
Understanding nurses’ perceptions goes beyond just measuring their attitudes and beliefs regarding their work environment. Clear relationships exist between how nurses perceive their work and critical outcomes. Total staffing and nurse perceptions shows the relationship between total staffing (hours per patient day) and measures related to nurses’ overall perception of their work, patients’ perceptions of their hospital stay, and patient outcomes related to falls, infections, and pressure ulcers. Staffing correlates significantly with each of these measures, with higher staffing associated with more positive nurse perceptions and patient experience and fewer negative patient outcomes.
However, nurses’ reported intention to stay with the organization and their beliefs about the status of the nursing department within their organization correlate more strongly to nurse perception, patient experience, and patient outcomes than staffing levels. These findings indicate that while staffing is important in all three areas, the strongest relationships occur in how RNs perceive the status of nursing on their unit. In other words, staffing is important, but work environment is even more important.
Caregiver themes
Compassionate Connected Care for caregiver themes derive from a qualitative study that asked thousands of clinicians to identify strategies that demonstrate compassion, connectedness, and caring for people who provide care at the bedside (nurses, physicians, transporters, and anyone else who interacts with patients). The following themes emerged:
- We should acknowledge the complexity and gravity of the work caregivers provide.
- Leadership needs to provide support in the form of material, human, and emotional resources.
- Empathy and trust must be fostered and modeled.
- Teamwork is vital to success.
- Caregivers’ perception of a positive work-life balance reduces compassion fatigue.
- Communication at all levels is foundational.
Acknowledgment of the work
Just as we must acknowledge that our patients suffer and respond accordingly, we must acknowledge that caregivers’ work is complex, important, and hard. This acknowledgment needn’t necessarily take the form of monetary or other tangible rewards. In fact, clinicians’ feedback on how they view recognition and appreciation of their role didn’t focus on compensation at all. Instead, they indicated that simply having their efforts acknowledged and receiving praise for good patient outcomes and behavior are meaningful when provided in a genuine, unscripted way. The essence to such acknowledgement is the perception that leaders “understand what I went through today.”
Acknowledgment can focus on an individual’s performance and can reinforce the role of the team and its accomplishments. When something goes wrong, root-cause analyses may be done to help avoid similar incidents in the future. By the same token, when things go well, leaders should pull the team together to deconstruct why this happened and use that learning to create more good days and good outcomes.
Leadership support
Cross-domain analytics illustrate staffing is important but work environment is even more important. Leaders create the work environment; in a positive environment, employees feel valued and supported.
• Leaders must ensure appropriate staffing based on patient acuity, complexity, and skill mix—not just volume.
• Staffing must be transparent so caregivers understand the complexity and reality of budgetary and regulatory constraints and can help solve related issues.
• Material resources needed for care must be available and in good working order. Having to constantly search for equipment or use equipment that’s not fully functional is inefficient, dangerous, and frustrating. Preventive maintenance and a proactive approach to capital management produces a much better return on investment than lost productivity and potential turnover costs associated with frustration and disengagement from lack of resources.
Empathy and trust
Empathy and trust built on accountability, integrity, and fidelity at all levels of the organization are critical to a positive work environment. The consistency and empowerment so basic to shared governance help instill trust in leadership and colleagues. For caregivers, empathy means treating each other with respect and anticipating and responding to each other’s needs. For this empathy and trust to be tangible in patient care, empathy and trust for each other and the organization mustbe embedded within the culture. Just as connecting with patients on a level beyond the reason for their hospitalization is important, leaders must connect with staff on a level beyond the reason they work there.
Teamwork
Health care is a team endeavor. No one person or discipline can do it alone. An interprofessional team of experts and support persons provides the best care for the patient in the best place for his or her care. The team must coordinate around the patient’s needs and diagnosis, not the caregivers’ or organization’s convenience. Teams that work together consistently and with the same patient populations show higher engagement with the organization and achieve better outcomes.
Work-life balance
As millennials begin to dominate the workplace, a positive work-life balance is more important than ever. Caregivers must believe the work they do is meaningful and purposeful. Yet much of what we do in health care is task oriented. Caregivers need to be reminded frequently that what they do affects the lives of their patients and their families in ways they may never know.
After each shift, caregivers want to leave work a “good” tired; even if they’re tired from a long day, they want to know they gave their patients excellent care and feel good about that care. When nurses or other caregivers begin to experience burnout or compassion fatigue, leaders must intervene quickly and appropriately so they can receive help rather than “infecting” colleagues.
Communication
For caregivers to demonstrate empathy and trust, good communication and transparency are required. Listening is a key component of communication—one that leaders don’t always demonstrate with employees (or caregivers with patients and families). Data transparency and opportunities to discuss and improve the data allow bedside caregivers to determine improvement strategies and drive accountability and ownership for improvement efforts. The patient’s care and outcome may hinge on clear, direct, timely communication of clinical impressions and plans among all team members to align focus and messaging to the patient.
Reducing patient suffering motivates caregivers
The patient and caregiver experiences are much more than a percentile rank or a line item on a report. Patients and caregivers suffer in unique ways. Some elements of suffering are inherent and require support to mitigate the effects. But much avoidable suffering for both patients and caregivers occurs— and must be eliminated. For caregivers, reducing patient suffering is the why that motivates and engages them.
The first step toward reducing suffering for patients and caregivers is to understand how the data show opportunities for improvement, the impact, and the effort required; this is the what. Strategies within the Compassionate Connected Care framework provide the how . Reducing suffering through compassionate and connected care for both patients and caregivers is the purpose on which we can all agree.
Christy Dempsey is a senior vice president and chief nursing officer at Press Ganey Associates, Inc. Deirdre Mylod is a senior vice president of Analytics/ Solutions and executive director of the Press Ganey Institute.
Selected references
Bakker D, Keithley JK. Implementing a centralized nurse-sensitive indicator management initiative in a community hospital. J Nurs Care Qual. 2013;28(3):241-9.
Bamford M, Wong CA, Laschinger H. The influence of authentic leadership and areas of worklife on work engagement of registered nurses. J Nurs Manag. 2013;21(3):529-40.
Choi J, Bergquist-Beringer S, Staggs VS. Linking RN workgroup satisfaction to pressure ulcers among older adults on acute care hospital units. Res Nurs Health. 2013;36(2):181-90.
Choi J, Boyle DK. RN workgroup job satisfaction and patient falls in acute care hospital units. J Nurs Adm. 2013;43(11):586-91.
Jobe LL. Generational differences in work ethic among 3 generations of registered nurses. J Nurs Adm. 2014;44(5):303-8.
Kelly D, Kutney-Lee A, Lake ET, Aiken LH. The critical care work environment and nurse-reported health care-associated infections. Am J Crit Care. 2013;22(6):482-8.
McAlearney AS, Robbins J. Using high-performance work practices in health care organizations: a perspective for nursing. J Nurs Care Quality. 2014;29(2):E11-20.
Meyer JP. The science–practice gap and employee engagement: it’s a matter of principle. Can Psychol. 2013;54(4):235-45.
Pavlish C, Hunt R. An exploratory study about meaningful work in acute care nursing. Nurs Forum. 2012;47(2):113-22.
Piper LE. Generation Y in healthcare: leading millennials in an era of reform. Front Health Serv Manage. 2012;29(1):16-28.
Sawatzky JA, Enns CL. Exploring the key predictors of retention in emergency nurses. J Nurs Manag. 2012;20(5):696-707.
Schaufenbuel K. Powering your bottom line through employee engagement. UNC Kenan-Flagler Business School; 2013.
Stimpfel AW, Aiken LH. Hospital staff nurses’ shift length associated with safety and quality of care. J Nurs Care Qual. 2013;28(2), 122-9.

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}