
Take fear out of the conversation.
- Black community members have low rates of advance directive completion
- The support of a church leader or pastor can help encourage advance care planning conversations.
- Nurses can make an impact through discussions in the community setting.
Advance care planning (ACP), a routine aspect of healthcare regardless of age or health concerns, helps individuals make decisions about future care by reviewing their values, goals, and wishes. It should involve the patient, their family and loved ones, and their healthcare provider. This ongoing process can change throughout a person’s lifespan and begin when they’re healthy. However, most of these conversations occur with elderly patients or those with serious illnesses. According to a Conversation Project survey, 92% of participants believe it’s important to discuss end-of-life care wishes, but only 32% have talked with their loved ones.
Nurses serve as educators when providing care for patients and families. Developing a rapport builds trust and understanding, which helps to strengthen nurse–patient relationships. Person-centered care requires a learning environment that extends beyond the hospital and into the community setting. Communicating effectively involves meeting patients and families where they live, gather, and worship. When nurses make provisions for a comfortable environment, we can discuss uncomfortable topics such as ACP with less anxiety.
Nouri and colleagues noted that many people from diverse communities feel reluctant to discuss end-of-life care wishes because of past experiences, cultural or spiritual beliefs, fear, and an overall distrust of the healthcare system. Black community members are even less likely to complete ACP documents or participate in these conversations because of these barriers and a lack of understanding of end-of-life care documents. Bazargan and colleagues compared data from a California study and found Black Americans less likely to complete advance directives compared to White Americans and other ethnic groups.
Advance directives defined
Completing advance directive documents can help decrease complications related to grief, such as depression, anxiety, and guilt among bereaved family members; however, limited research exists related to financial cost savings. Most ACP conversations occur in hospitals, provider offices, or before outpatient procedures. ACP documents can prove confusing to healthcare clinicians as well as patients or community members. The confusion results from lack of knowledge and understanding.
Ultimately, advance directives serve as a guide for clinicians regarding a person’s desired care at the end of life. Although efforts and studies aim to alleviate the confusion of advance care planning documents for patients and to understand why completion rates for Black patients remain lower than for other populations, little progress has been made.
Advance directives, which are legal documents, include healthcare powers of attorney and living wills. The healthcare power of attorney names a person to speak for someone when that person can’t speak for themselves. A living will allows a person to make decisions about life-sustaining treatments in certain situations. Advance directive documents differ from state to state, but all have the same goal of making wishes known to families and healthcare providers.
The literature
McDonnell and colleagues found that programs involving a pastor and built upon existing ministries within a congregation support ACP and end-of-life conversation education among members. McDonnell’s study of Blacks in southeast North Carolina found that parishioners were more likely to discuss ACP in a church-led program than in any other setting. Nouri, Campbell, and others support moving ACP away from the healthcare setting to community organizations like churches to engage Black Americans and provide information from familiar sources.
Fink and colleagues found that community-based education models about ACP in ethnic and underserved populations can increase awareness and buy-in. Research conducted by Ohr and associates showed that patients and families felt supported when discussing end-of-life care with nurses due to their knowledge and professional advice. A similar study by Whitehead and colleagues reviewed nurse-led ACP education models and found that nurses proved essential in improving patient–provider communication.
Rezaei and colleagues explained that the theory of planned behavior successfully predicts health behaviors and the use of health services. According to this model, an individual’s intention to engage in a specific behavior is primarily influenced by their attitude toward that behavior. Changing attitudes around ACP in a Black church community by alleviating the knowledge deficit to modify behavior aligns with this theory.
Evidence-based intervention
Historically, Black American churches not only serve as places to receive spiritual guidance but also as sanctuaries for parishioners to obtain trusted and valuable information. Effective ACP conversations must consider spirituality and religion. As noted by Johnson and colleagues, Black American churches serve as suitable environments to train laypeople how to educate parishioners in ACP and goals-of-care conversations. Listening, Identifying, Guiding, Helping, Translating (LIGHT), a church-based curriculum, provides instruction in effective communication and ACP conversations.
Our study, approved by the University of Alabama Institutional Review Board, provided an evidence-based education intervention within a Black American church with the goal of increasing member ACP knowledge and their readiness to complete advance directive documents.
The educational intervention used the Respecting Choices Group Facilitation Program presentation, which is designed for community settings and engages participants on a personal level about ACP and conversations about end-of-life decision-making. According to Ejem and colleagues, the Respecting Choices program has been implemented worldwide and shown to improve prevalence of advance directives, treatment preferences aligned with patient wishes, and consistency in patient–healthcare agent (healthcare proxy) medical decisions and to reduce use of unwanted care.
We conducted our study at Wilson Heights First Church of God, a Black church situated in an underserved community on the west side of Charlotte, North Carolina. Currently, the church offers healthy living programs, such as diabetes education and a community garden. Participants included 35 church members and staff.
The nurse leader conducted two education sessions, one after a Sunday worship service and one during an evening Bible study later that week. The lead pastor prefaced the Sunday session with a message focused on taking care of your affairs in the present to bless your family later. This opening provided a perfect segue to the educational intervention. In addition, beginning the study with a trusted church figure established the importance of these conversations and helped to reduce apprehension related to ACP.
After the pastor’s message, the lead nurse offered an overview of the education session and then administered a pre-intervention survey to all participants. After collecting and securing all surveys, we delivered a 45-minute presentation, followed by a 15-minute question-and-answer session. After addressing all questions and concerns, we administered and collected the post-intervention survey. The nurse leader offered an opportunity for participants to complete advance directive documents after both sessions and provided future opportunities for another workshop at the pastor’s discretion. All church members had access to both sessions, but those under age 18 and those viewing the session via live stream didn’t participate in the intervention surveys.
Intervention outcomes
The results of this educational intervention showed significant improvement in participants’ willingness to take action regarding end-of-life decisions. The most improvement occurred in their plans to make changes within the next 30 days. Participants reported a 35% change in readiness to name a person to make decisions for them and a 38% change in readiness to talk about the type of care desired. Talking to a doctor about medical decisions increased by 41% after the intervention. The highest increase occurred in readiness to sign official papers about medical care and wishes (44% increase from pre- to post-intervention survey). (See Readiness outcomes.)
Readiness outcomes
Participants in the advance care planning educational sessions completed pre- and post-intervention surveys to gauge their readiness to have conversations with their providers and complete documentation related to end-of-life care.
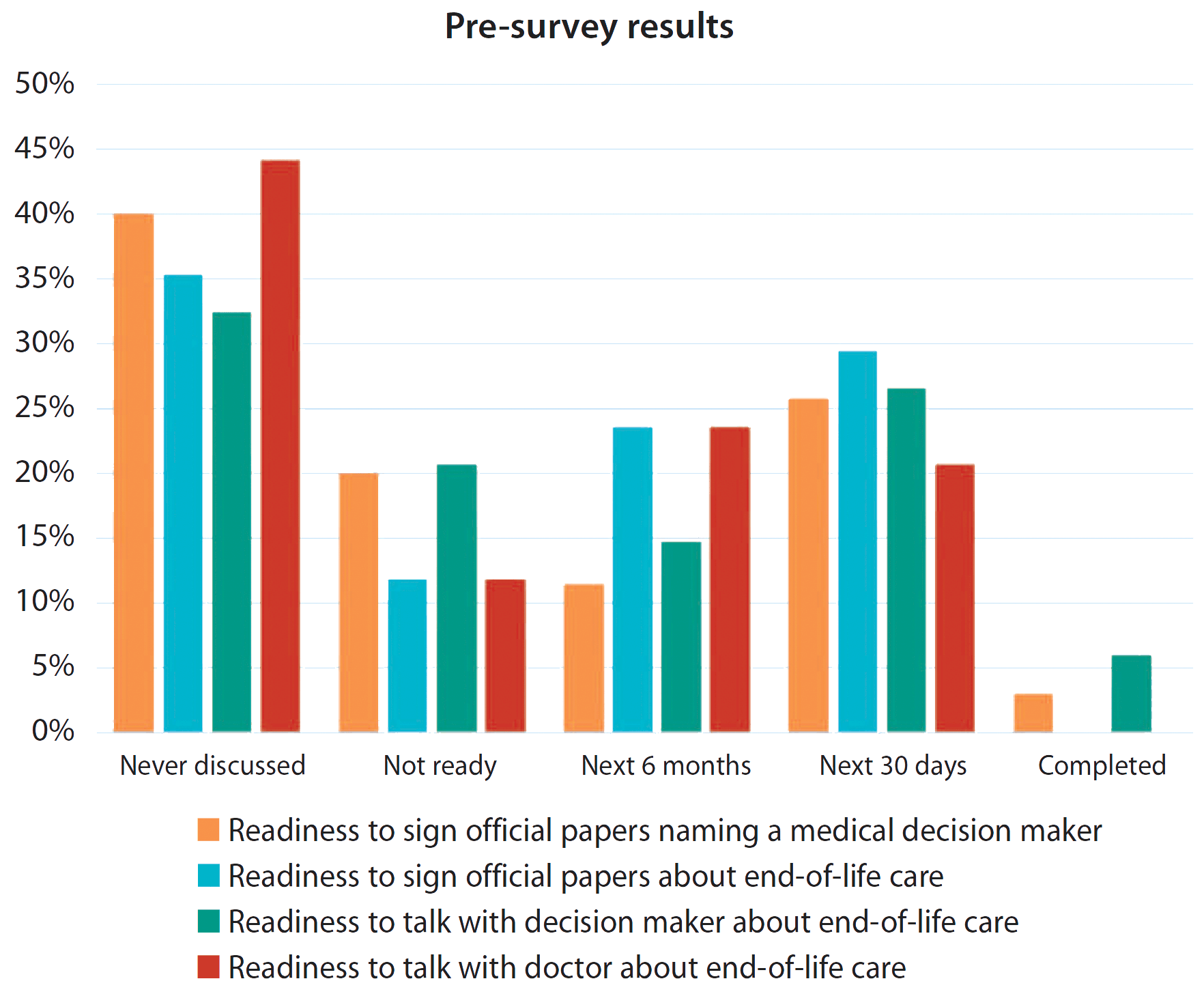
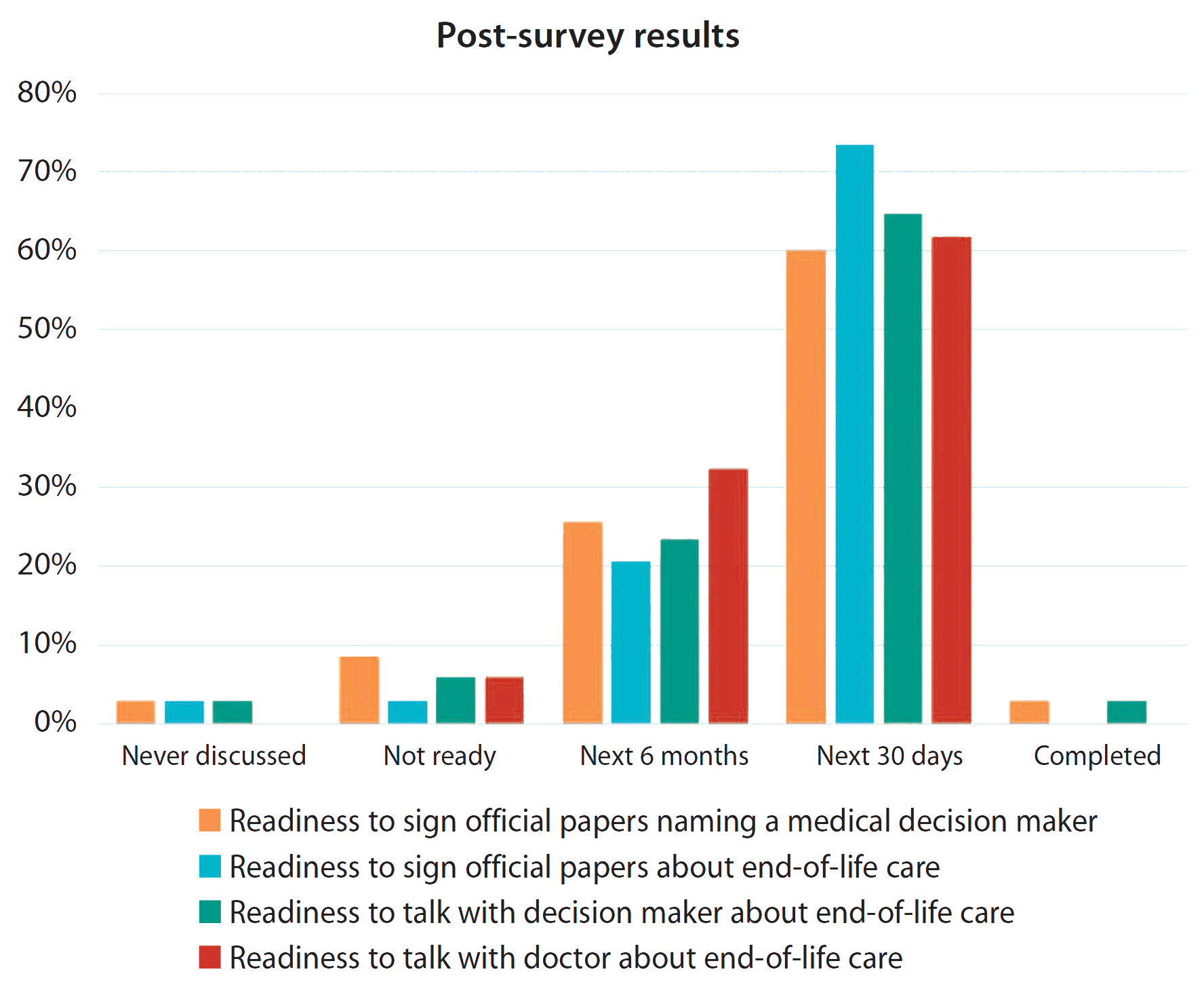
All the changes represent an increase in readiness to discuss and make decisions about ACP, which reinforces the Theory of Planned Behavior (changing behaviors by changing attitudes). Alleviating fear of ACP conversations encouraged the participants to plan discussions and actions toward completing advance directives soon.
Challenges and concerns
The church site broadcasts its Sunday morning worship via live social media platforms. Although this option helped provide educational intervention to remote parishioners, we excluded them from participating in the readiness survey. In addition, during the Sunday session, the nurse leader couldn’t show the PowerPoint presentation to in-person participants; instead, they followed along via printed handouts.
Nursing implications
Conducting educational sessions in churches helps nurses reduce barriers to providing person-centered care. Participants in this intervention had opportunities to complete advance directives; four (11%) did so. North Carolina advance directives require notarization and signatures from two unrelated witnesses, which can present challenges for some individuals. North Carolina nurses continue to advocate to change these laws.
Build trust, provide vital education
ACP conversations can prove difficult for patients and families, especially among Black Americans who may distrust how and when the documents will be used. This intervention took the discussion out of the hospital and into the community. Providing education in a comfortable environment, such as a church, helps to build trust and alleviate fear associated with advance directives.
Black Americans complete advance directives at a much lower rate than their White counterparts, highlighting the need for education on the importance of advance care planning in the community. Results of this intervention support the Black American community’s need for ACP education and nurses’ integral role in providing this valuable information.
Michelle Kirby is director of business operations at Atrium Health, a part of Advocate Health, in Concord, North Carolina. Kim Parker is a clinical assistant professor at the University of Alabama Capstone College of Nursing in Tuscaloosa.
American Nurse Journal. 2025; 20(5). Doi: 10.51256/ANJ052528
References
Baker EF, Marco CA. Advance directives in the emergency department. JACEP Open. 2020;1(3):270-5. doi:10.1002/emp2.12021
Bazargan M, Cobb S, Assari S. Completion of advance directives among African Americans and white adults. Patient Educ Couns. 2021;104(11):2763-71. doi:10.1016/j.pec.2021.03.031
Campbell CL, Williams IC, Campbell LC. Church matters: Education about advance care planning and end-of-life care in Black churches. Fam Community Health. 2023; 46(3):176-80. doi:10.1097/fch.0000000000000365
CaringInfo. Advance directives. caringinfo.org/planning/advance-directives
The Conversation Project. Institute for Healthcare Improvement. theconversationproject.org/about
Ejem DB, Barrett N, Rhodes RL, et al. Reducing disparities in the quality of palliative care for older African Americans through improved advance care planning: Study design and protocol. J Palliat Med. 2019;22(S1):90-100. doi:10.1089/jpm.2019.0146
Fink RM, Kline DM, Bailey FA, et al. Community-based conversations about advance care planning for underserved populations using lay patient navigators. J Palliat Med. 2020;23(7):907-14. doi:10.1089/jpm.2019.0470
Johnson J, Hayden T, Taylor L. Evaluation of the LIGHT curriculum: An African American church-based curriculum for training lay health workers to support advance care planning, end-of-life decision making, and care. J Palliat Med. 2022;25(3):413-20. doi:10.1089/jpm.2021.0235
Rezaei MA, Zahiri A, Kianian T, et al. Factors related to patients’ readiness for advance care planning: A systematic review. BMC Public Health. 2025;25(1):78. doi:10.1186/s12889-024-21209-x
McDonnell J, Idler E. Promoting advance care planning in African American faith communities: Literature review and assessment of church-based programs. Palliat Care Soc Pract. 2020;14:263235242097578. doi:10.1177/2632352420975780
Nouri S, Quinn M, Doyle BN, et al. “We’ve got to bring information to where people are comfortable”: Community-based advance care planning with the Black community. J Gen Intern Med. 2023;38(11):2478-85. doi:10.1007/s11606-023-08134-2
Ohr SO, Cleasby P, Jeong S, Barrett T. Nurse-led normalised advance care planning service in hospital and community health settings: A qualitative study. BMC Palliat Care. 2021;20(1):139. doi:10.1186/s12904-021-00835-x
Whitehead P, Frechman E, Johnstone-Petty M, et al. A scoping review of nurse-led advance care planning. Nurs Outlook. 2022;70(1):96-118. doi:10.1016/j.outlook.2021.08.002
Key words: advance care planning, African Americans, faith communities


















