
A collaborative initiative yields positive outcomes despite challenging circumstances.
Takeaways:
- Shared governance is a framework that empowers collaborative decision-making and positively impacts nursing practice.
- Transforming and strengthening nursing shared governance is essential for the future of nursing and healthcare organizations.
- Organizational support to encourage understanding and growth of shared governance knowledge and leadership skills can have an immense impact on the effectiveness of nursing councils.
A strong shared governance structure has been shown to enhance the effectiveness of healthcare organizations by improving patient outcomes, increasing nurse satisfaction, supporting nurse autonomy, and strengthening nursing practice. Despite the challenges faced throughout the COVID-19 pandemic, healthcare organizations must remain committed to a culture that values and supports shared governance.
In early 2020, UW Health, a large academic medical center with 595 beds and 45 clinics, sought to strengthen its shared governance structure. The process began with a current state assessment, which led to a 3-day workshop with an overall goal of transforming nursing practice through nurse empowerment.
Assessing the situation
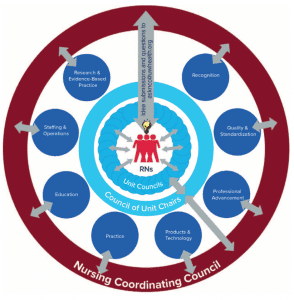
As a Magnet® organization, UW Health values and promotes nurse autonomy. It launched a formal nursing shared governance council structure in 2004, which by 2020 included eight system-level councils (practice, products and technology, professional advancement, recognition, quality and standardization, education, research and evidence-based practice, and staffing), a council of unit chairs, a nurse executive council, and unit councils. UW Health’s overarching nursing council, the nurse coordinating council (NCC), consists of the chairs and co-chairs of each of the eight system-level councils and council of unit chairs. (See Shared governance structure.)
The NCC completed a current state assessment of the system-level council structure, including all system-level councils, the NCC itself, and the council of unit chairs, to identify strengths and barriers of shared governance using a fishbone diagram (a visualization tool for identifying problems and understanding their root causes). The NCC then assessed the combined strengths and barriers of all the councils to pinpoint themes and subthemes to target for improvement. To objectively evaluate the operations within each individual shared governance council, members completed the Council Health survey tool. Results of the current state assessment revealed a need for leadership development of system-level council chairs and enhancement of shared governance council processes.
NCC health survey
As part of our assessment of the current state of UW Health’s shared governance structure, we conducted a nurse coordinating council (NCC) survey using the Council Health survey developed by Robert Hess (used with permission; to request permission, contact info@sharedgovernance.org).
Participants rated each item on a Likert scale (1 = strongly disagree; 2 = disagree; 3 = neutral; 4 = agree; 5 = strongly agree). After the workshop, survey results improved in 20 of 25 survey items.
| Survey items | Pre-workshop results (N=17) | Post-workshop results (N=13) | Percent change in mean |
| Our council has a process to assess each other’s participation in the council. | 2.94 | 3.38 | 15% |
| Our council has formal education or training for new council members/leaders. | 3.47 | 3.96 | 14% |
| Our council members make meaningful decisions. | 3.65 | 4.13 | 13% |
| Our council members use decisions to change practice. | 3.59 | 4.05 | 13% |
| Our council members have the necessary computer and project management skills to perform council activities. | 3.12 | 3.39 | 9% |
| Our council members participate in activities that improve our professional practice environment. | 3.88 | 4.22 | 9% |
| Our council members communicate decisions to all stakeholders. | 3.29 | 3.56 | 8% |
| Our council members participate in activities that improve the care of patients. | 3.59 | 3.89 | 8% |
| Our council has processes for selecting and deselecting council members. | 4.06 | 4.31 | 6% |
| Our council members use data and/or evidence-based practice in making decisions. | 3.71 | 3.9 | 5% |
| Our council members make decisions that are aligned with the organization’s strategic goals. | 3.82 | 3.99 | 4% |
| Our council has strategies to ensure members have dedicated time to complete council work. | 3.53 | 3.66 | 4% |
| Our council has established clear avenues for non-council members to contribute to council work. | 3.59 | 3.74 | 4% |
| Our council member use consensus to make decisions. | 4.18 | 4.32 | 3% |
| Our council has charter/bylaws that describe expectations of its council members. | 3.82 | 3.91 | 2% |
| Our council has charter/bylaws that define its membership. | 4.06 | 4.16 | 2% |
| Our council members have a management leadership team that is engaged in our council work. | 4 | 4.08 | 2% |
| Our council members regularly attend meetings as specified in the charter/bylaws. | 4.53 | 4.58 | 1% |
| Our council members complete assigned council work between meetings. | 3.71 | 3.75 | 1% |
| Our council members have council chairs and management leadership teams that collaborate on council work. | 3.94 | 3.99 | 1% |
| Our council has charter/bylaws that define its work. | 3.76 | 3.75 | 0% |
| Our council members are engaged during meetings. | 4.59 | 4.58 | 0% |
| Our council members use effective, direct, and respectful communication. | 4.65 | 4.67 | 0% |
| Our council members make decisions that reflect the values and preferences of those they represent. | 4.06 | 4 | –1% |
| Our council members manage conflict effectively and respectfully. | 4.47 | 4.34 | –3% |
Designing a workshop
With commitment and backing from the organization’s chief executive officer and interim chief nurse executive, the authors designed a 2-day workshop to provide the NCC with focused time to address identified barriers, which was approved for June 2020. Planning for the interactive workshop began immediately with support from key stakeholders, including Magnet and nursing excellence department staff (planning), nursing education and development department staff (contact hour guidance), nursing education council and nurse coordinating council chairs (direct-care nurse feedback and planning), and UW Health’s organizational improvement department (activity development). The workshop agenda was first shared with the NCC chair for initial review. Before finalizing the agenda, all NCC members reviewed and prioritized topics based on their identified needs. (See Workshop structure.)
Workshop structure
The overall goal of the workshop was to achieve three main outcomes:
• Prepare nurses to become council leaders.
• Address identified barriers to the organization’s shared governance council structure.
• Revise the organization’s nursing philosophy, mission, and vision.
Topics for the first day included the following:
• shared governance structures at UW Health
• meeting facilitation
• virtual meeting and communication skills
• quality improvement
• evidence-based practice
• research
• department leader presentations (finance, marketing, human resources, quality)
• strategic planning preparation.
Work conducted on the second day included the following:
• developing a new nursing philosophy, mission, and vision
• creating a marketing and communication plan for nursing shared governance
• designing a plan for the upcoming fiscal year
Safety and technology
In addition to planning the content of the workshop, extensive logistical preparation ensured all Centers for Disease Control and Prevention and organizational COVID-19 guidelines were followed. To support contact tracing recommendations, each workshop attendee was assigned to one of three meeting rooms, which remained consistent throughout each day and session.
The workshop was offered in a hybrid format of in-person and virtual sessions, but it could have been exclusively virtual. The workshop was held in an administrative building with low occupancy during the pandemic. Attendance included 30 incoming and outgoing NCC members. When attendees arrived, they were directed to their assigned rooms. The three rooms allowed for adequate physical distancing, and attendees wore masks at all times.
The rooms were connected via teleconferencing technology with screen sharing and video capabilities. Overhead microphones permitted attendees to control when audio connections between rooms were active, providing opportunity for individual room collaboration or larger group interaction. Presenters rotated among rooms, which guaranteed that each workshop participant would receive equal in-person presentation time. To ensure participants had everything they needed, one facilitator was present in each room to guide group discussions and manage technology.
Day 1: Setting the stage
On the first day of the workshop, participants discussed a variety of topics, including meeting facilitation, communication skills, and evidence-based practice. The outcomes from those discussions were evaluated and incorporated into activities for the second day. This structure encouraged participants to build on their learnings and implement new concepts during collaborative group work.
Day 2: Mission and vision
Day 2 began by developing a new nursing philosophy, mission, and vision. Using the teleconferencing technology, all participants updated the organization’s existing nursing philosophy, then each individual room broke into two separate groups to develop mission and vision statements. They wrote their statements on easels that were displayed in a shared hallway. Each group viewed the statements, and then each participant used a sticker dot to vote on their preference. Mission and vision statements with the most votes were reviewed with the entire group, and edits made before finalizing each.
The finalized nursing mission statement consists of the following: “To innovate and advance healthcare without compromise through service, scholarship, science, and social responsibility while providing remarkable patient-, family-, and community-centered care across the continuum of health and wellbeing.” The finalized nursing vision statement reads as such: “To serve as remarkable and trusted national leaders in nursing. Every day.”
Day 2: Communication plan
The organization’s chief marketing officer and nursing corporate communication strategist provided education to help participants create a communication plan aimed at promoting nursing shared governance. The participants then split up into four separate groups. Three of the groups worked on developing an overall communication strategy, including an algorithm for triaging nursing questions, comments, and suggestions to the appropriate resource; a process for requests made to the NCC; and a plan for communication between councils. The fourth workgroup refined membership attendance expectations, a council process that required updating. Each group then shared a summary of their work.
Day 2: Implementation plan
At the end of the day, the entire group discussed an implementation plan that included activities identified during the workshop that needed further work and provided momentum and direction for all shared governance councils for the coming year. The implementation plan comprised 26 items, including creating an NCC charter, producing resources for conducting virtual meetings, and enhancing a council membership model representative of all care areas.
Outcomes
After the workshop, all participants were asked to complete an evaluation form. Feedback was overwhelmingly positive, with participants saying that an annual workshop would be beneficial because NCC members change each year.
Anticipated outcomes for the workshop were met, including preparing nurses for their roles as council leaders, addressing barriers to the organization’s shared governance council structure, and creating new nursing mission, vision, and philosophy statements. In addition, the workshop allowed for nurse-to-nurse and interdisciplinary engagement during the pandemic, firsthand experience with virtual meeting skills and strategies, opportunities to lead small and large group work, and improved confidence in leadership abilities and communication. Leadership presence throughout the workshop allowed council chairs to interact, engage, and feel supported by nursing leaders.
Obstacles encountered during the workshop included having only 4 weeks to prepare, complying with COVID19 guidelines to ensure staff safety, and working through technology glitches. Despite these few challenges, the workshop successfully enhanced and strengthened the organization’s shared governance structure.
Long-term effects and benefits of the workshop were seen throughout the following year. Because in-person meetings weren’t possible for most of the year, the virtual meeting skills obtained during the workshop were invaluable to participants during council activities.
Technology has transformed the way all employees within the organization work, and the skills gained during the workshop aided nursing shared governance progress. In addition, workshop outcomes have cascaded to members of each of the system-level and area councils, allowing all nurses involved in shared governance to benefit. (See Outcomes by the numbers.)
Outcomes by the numbers
Six months after the workshop, the nurse coordinating council re-evaluated its operations by repeating the Council Health Survey measurement tool.
• Of the 23 NCC members, 17 (73.9%) completed the preassessment, and 13 of 21 (61.9%) completed the postassessment.
• Results showed positive improvements in 20 of 25 measures, with more than 5% improvement to the following measures:
• have the necessary computer and project management skills to perform council activities: 9%
• make meaningful decisions: 13%
• use decisions to change practice: 13%
• communicate decisions to all stakeholders: 8%
• participate in activities that improve the care of patients: 8%
• participate in activities that improve the professional practice environment: 9%
• provide formal education or training for new council members/leaders: 14%
• establish a process for selecting and deselecting council members: 6%
• establish a process to assess each other’s participation in the council: 15%.
These results support the effectiveness of the knowledge and skills gained from the workshop in strengthening the NCC’s shared governance operations. Further evaluation to assess the impact of the workshop on the organization’s other councils is in progress.
Transformation for the future
Transforming and strengthening nursing shared governance is essential for the future of healthcare organizations. Organizational support to encourage the understanding and growth of shared governance knowledge and leadership skills can have an immense impact on the effectiveness of nursing councils. UW Health found success creating and implementing the workshop, despite challenges posed by the pandemic. This work resulted in many benefits and can be easily replicated by other organizations.
The authors work at UW Health in Madison, Wisconsin. Dani Edwards is a nursing program specialist for Magnet and Nursing Excellence. Sarah Brzozowski is director of Magnet and Nursing Excellence. Susan Rees is in-patient regional vice president and chief nursing officer. Meghan Reisman is care team leader of emergency services. Mandy Jo Mlsna is an in-patient staff nurse. Rebecca Rankin is director of nursing informatics. The authors thank the nurse coordinating council members for their dedication to advancing shared governance and the nursing profession.
References
American Nurses Credentialing Center. 2019 Magnet® Application Manual. American Nurses Credentialing Center; 2019.
Boswell C, Opton L, Owen DC. Exploring shared governance for an academic nursing setting. J Nurs Educ. 2017;56(4):197-203. doi: 10.3928/01484834-20170323-02
Hess Jr RG, Bonamer JI, Swihart D, Brull S. Measuring council health to transform shared governance processes and practice. J Nurs Adm. 2020;50(2):104-8. doi: 10.1097/NNA.0000000000000849
Hess Jr RG, Weaver SH, Speroni KG. Shared governance during a pandemic. Nurse Lead. 2020;18(5):497-9. doi: 10.1016/j.mnl.2020.05.008
Joseph ML, Bogue RJ. A theory-based approach to nursing shared governance. Nurs Outlook. 2016;64(4):339-51. doi: 10.1016/j.outlook.2016.01.004
Porter-O’Grady T. Is shared governance still relevant? J Nurs Adm. 2001;31(10):468-73. doi: 10.1097/00005110-200110000-00010.

















