
Nurses can work with the organ donation team to meet patients’ wishes and optimize donation benefits.
Takeaways:
- Nurses and other healthcare disciplines must be knowledgeable about organ donation.
- Early identification of a potential organ donor by the nurse and collaboration with the transplant coordinator are vital for successful organ donation.
- The care of the transplant donor and recipient is complex and requires teamwork and collaboration with the transplant team.
One particular case that exemplifies the selflessness of some people and makes organ/tissue/eye donation so special to me was of a baby boy who was under 2 years of age. Sadly he died of head trauma. His mother told me that if she could help one other mother not go through the loss of a child that this would help her bring closure from the loss of her child. The young mother and her parents asked me to attend the funeral services and I did. The donation saved four people. They used the heart, liver, and kidneys. —R.S. Murphy
Transplant statistics demonstrate the continued need for patient advocacy, education, and support. Since 1988, 683,000 transplants have been performed (in 2016 alone, 33,600 patients received a transplant), but the demand for organs far outweighs the supply. Currently, 115,000 men, women, and children are waiting for a transplant, and every year 8,000 people die while waiting for a transplant. According to the United Network for Organ Sharing (UNOS), 2018 saw more transplants than ever, and the number of living donors was 6,900 (the highest since 2005).
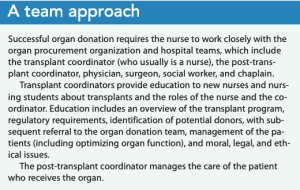
All nurses are critical to organ donation advocacy education. In the acute-care setting, nurses must be aware of the guidelines and procedures for organ donation so they can help identify potential donors and work with the organ donation team. (See A team approach.)
 About organ donation programs
About organ donation programs
 About organ donation programs
About organ donation programsLaws and regulations govern U.S. organ donation. In 1984, the National Organ Transplant Act (NOTA) established the Organ Procurement and Transplantation Network (OPTN) to manage a national organ-matching registry. NOTA requires OPTN to be operated by a private, nonprofit organization under contract with the federal government. In 1986, UNOS took on that role and is responsible for allocation policy data collection and analysis, organ matching, and education of the public and healthcare providers.
The Centers for Medicare and Medicaid Services (CMS) regulate hospital compliance with all aspects of the U.S. donor program, and The Joint Commission requires hospitals to have a written agreement with an organ procurement organization (OPO). Hospitals also are required to have policies and procedures for organ and tissue procurement and donation.
UNOS matches organ donors and recipients. Patients needing a transplant are ranked according to medical urgency, blood and tissue type, expected benefit, waiting time, and geography. Priority is given to pediatric patients and living organ donors, such as patients who donated a kidney and whose remaining kidney is failing.
Identifying the donor and obtaining consent
Timely identification and management of potential donors is crucial to successful organ donation. Potential organ donors—including those who are brain dead or have imminent brain death as a result of a fatal medical condition or traumatic event (such as severe head injury, cerebral bleed, or cardiac arrest)—typically are identified by the patient’s assigned nurse or provider. Criteria for brain death include loss of two or more brainstem reflexes (for example, cough, gag, or pain reaction). In the case of planned removal of a ventilator, a transplant coordinator should be asked to evaluate if the patient is a suitable candidate. (See Organ donation after brain or cardiac death.)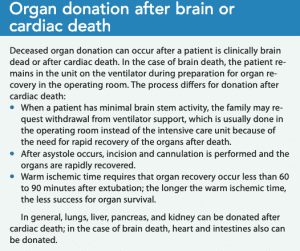
The nurse notifies the OPO transplant coordinator of the potential donor. The coordinator verifies that the donor meets guidelines for organ donation and checks if the patient is listed in the state’s donor registry. Patients who are registered as organ donors are considered to have given consent, and the family can’t reverse their wishes. In extenuating circumstances when the family doesn’t agree with the patient’s decision, the transplant coordinator may elect not to proceed with the donation, but for the most part, the patient’s registration is a legal and binding decision that will usually be followed.
If the patient is not a registered donor, the transplant coordinator obtains consent from the authorized party as defined by the Uniform Anatomical Gift Act. The Act, which was passed in 1968 and revised in 1987 and 2006, establishes the regulatory framework for the donation of organs, tissues, and other human body parts in the United States.
A myth of organ donation is that families aren’t given adequate time to come to terms with their loved one’s brain death. However, decoupling (allowing time after explaining the patient’s grave prognosis for the family members to understand and accept the impending loss) is always provided.
The transplant coordinator works with the nurse to manage the potential donor. The overall goal is to reverse or mitigate (using supportive and therapeutic measures) the physiologic changes (severe autonomic or inflammatory response) that occur after brain death. (See Organ donor management goals.) To ensure appropriate management and preparation for organ recovery, the average time from donor consent to the operating room is 48 to 72 hours. Throughout the process, the nurse collaborates with the transplant coordinator and advocates for the family.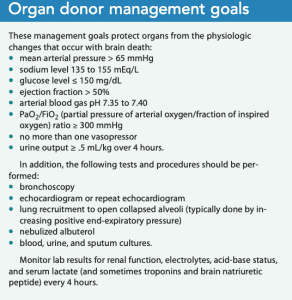
Clinical management
After the organ transplant, the post-transplant coordinator collaborates with the nurse to manage care of the recipient patient, including following organization policies and procedures for surgical site assessments and dressing changes and closely monitoring the patient’s hemodynamics, vital signs, and blood work for potential postoperative complications and organ rejection.
All patients who receive a solid organ transplant are prescribed immunosuppressive therapy to prevent organ rejection. Induction therapy begins at the time of the transplant and typically includes high-dose glucocorticoids and biologic antibodies (such as basiliximab). In addition, patients will receive long-term maintenance immunosuppressive therapy, which is selected based on individual patient need, side effects, and efficacy. Common medications include glucocorticoids, antimetabolites (such as azathioprine), calcineurin inhibitors (such as cyclosporine), mammalian target inhibitors (such as everolimus), or selective T-cell costimulation blockers (such as belatacept) to inhibit T-cell activation. Potential side effects of immunosuppressive therapies include malignancy, infections, cardiovascular disease, and post-transplant diabetes.
Patient education should focus on self-care and management and include information about medications, wound care, complications, diet and exercise recommendations, and the importance of follow-up appointments. It also should include information about possible immunotherapy-related malignances and signs of rejection specific to organ type.
Organ-specific care
Patient monitoring continues after hospital discharge and is based on the transplanted organ.
Kidney
Patients who’ve received a kidney transplant should:
- be monitored by the transplant team for 6 months and then by the nephrologist
- maintain a healthy lifestyle by keeping their body mass index within normal ranges, not smoking, eating a healthy diet, exercising, avoiding alcohol in the early transplant phase (discuss time frame with provider) and then consuming it only in moderation (consuming 10 to 30 g of alcohol per day has been associated with post-transplant diabetes and metabolic syndrome)
- take immunosuppressant or antirejection medications as prescribed
- avoid live vaccines, traveling to other countries (until cleared by their providers), and infections.
Heart
The International Society for Heart and Lung Transplantation recommends that patients who’ve received a heart transplant should:
- be monitored for cardiovascular risk factors (hypertension, diabetes, hyperlipidemia, smoking, and obesity)
- receive statin therapy
- have annual or biannual coronary angiography tests
- have coronary angiography every 6 to 12 months to evaluate for cardiac allograft vasculopathy
- have coronary angiography 6 months after percutaneous coronary intervention.
Liver
Patients who’ve received a liver transplant should avoid alcohol and be monitored for complications and signs of graft dysfunction, including elevated liver enzymes, acute chronic cellular rejection, biliary obstruction, and hepatic artery thrombosis/stenosis.
Other metabolic complications and possible manifestations that can occur in liver and other types of transplants include hypertension, new-onset diabetes, and chronic kidney disease.
Lungs
Lung transplant recipients may experience multiple complications, including graft rejection, infection, reperfusion injury, and anastomotic breakdown. Early respiratory distress identification and ventilator management are key to preventing complications.
Organ donation advocacy
Identifying and managing transplant donors and recipients is complex and requires collaboration between the transplant coordinator, nurses, and physicians. Although these patients are cared for in critical-care settings, all nurses should have a full understanding of the donor process so they can advocate for organ donation with their patients and in the community.
Deborah Hunt is associate dean and professor of nursing at Mercy College in New Rochelle, New York. R. Scott Murphy is the donor evaluation coordinator at LiveOnNY in New York, New York.
References
Bhat M, Al-Busafi S, Deschênes M, Ghali P. Care of the liver transplant patient. Can J Gastroenterol Hepatol. 2014;28(4):213-9.
Centers for Medicare & Medicaid Services. Transplant. May 5, 2020. cms.gov/Medicare/Provider-Enrollment-and-Certification/CertificationandComplianc/Transplant.html
Chandraker A, Yeung MY. Kidney transplantation in adults: Overview of care of the adult kidney transplant recipient. UpToDate.com.
Costanzo MR, Dipchand A, Starling R, et al. The International Society of Heart and Lung Transplantation guidelines for the care of heart transplant recipients. J Heart Lung Transplant. 2010;29(8):914-56.
Danovitch GM. Handbook of Kidney Transplantation. 6th ed. Philadelphia: Wolters Kluwer; 2017.
Donate Life America. Organ, eye and tissue donation statistics. donatelife.net/statistics
Duarte RT, Linch GF, Caregnato RCA. The immediate post-operative period following lung transplantation: Mapping of nursing interventions. Rev Lat Am Enfermagem. 2014;22(5):778-84.
Gift of Life Institute. Hospital development. www.giftoflifeinstitute.org/category/hospital-development
HCPro. Joint Commission clarifies organ procurement requirements. May 6, 2014. hcpro.com/ACC-304209-4634/Joint-Commission-clarifies-organ-procurement-requirements.html
Jawoniyi OO, Gormley K. How critical care nurses’ roles and education affect organ donation. Br J Nurs. 2015;24(13):698-700.
National Kidney Foundation. Care after kidney transplant. 2015. kidney.org/atoz/content/immunosuppression
Organ Procurement and Transplantation Network. About transplantation: History. optn.transplant.hrsa.gov/learn/about-transplantation/history
Organ Procurement and Transplantation Network. Organ transplants in United States set sixth consecutive record in 2018. January 7, 2019. optn.transplant.hrsa.gov/news/organ-transplants-in-united-states-set-sixth-consecutive-record-in-2018
Potestio C, Jordan D, Kachulis, B. Acute postoperative management after lung transplantation. Best Pract Res Clin Anaesthesiol. 2017;31(2):273-84.
Turner K, Burns T, Tranter S. An evaluation of the nursing care of renal transplant recipients: A qualitative study. Renal Soc Australasia J. 2018;14(1):21-5.
United Network for Organ Sharing. History. unos.org/transplantation/history
Wallace B. CPTC Exam Review and Handbook for the Organ Procurement Coordinator: A Comprehensive Study Guide for the Certified Procurement Transplant Coordinator Exam. 2nd ed. Scottsdale, AZ: Nurse Brooke CPTC; 2019.


















3 Comments.
awesome information about organ donation all content are useful
Dear Rick,
Thank you so much! It is a topic near and dear to our hearts.
Best,
Deb and Scott
Very impressive, informative and relevant writing and topic. Thanks for highlighting the need and upside of organ and tissue donation.