
Overcome stigma and misconceptions to ensure quality care.
Learning Objectives:
- Describe nursing care for patients on an acute medical unit who have comorbid mental illness.
- Discuss education and effective communication skills essential for nurses caring for patients on a medical unit who have comorbid mental illness.
- Define how holistic treatment of patients on a medical unit who have mental illness can help reduce symptoms and ensure quality, compassionate care.
- Discuss nursing interventions when caring for patients on a medical unit who have underlying mental illness.
The authors and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CNE credit. Expiration: 6/1/25
- Approximately 20% of U.S. adults experience some form of mental illness.
- Some chronic medical conditions (autoimmune disorders, diabetes) place patients at higher risk for mental illnesses, such as depression, and some mental illnesses increase the risk that a patient may develop a medical condition.
- Many people with psychiatric illnesses don’t seek healthcare out of fear that they won’t receive appropriate treatment.
- Improving care requires reducing stigma, providing nurse education, improving communication, enhancing the environment, and intervening appropriately
What do you think when you have a patient with pneumonia and a history of mental illness? Before even meeting the patient, do you assume you’ll face difficulty providing care? Several questions may come to mind: How much time will I need to dedicate to this patient? Will the patient take prescribed medication? What if the patient is aggressive? If the patient requires sedation, will that worsen their medical condition? These concerns and others may affect your nursing care.
Recognizing and treating dissociative disorders
Depression and chronic medical illness in adults
A recent article in The Hospitalist refers to patients with an acute medical condition and a comorbid psychiatric illness as a management problem. However, rather than viewing these patients as problems, treat them holistically to help reduce symptoms and ensure quality, compassionate care. Take time to learn more about mental illness and how you can address patients’ symptoms and concerns.
Understanding mental illness
Mental illnesses involve changes in emotions, thought processes, or behaviors associated with distress or impaired function in social, family, or work activities. The National Institute of Mental Health (NIMH) estimates that approximately 20% of U.S. adults experience some form of mental illness. The entertainment industry and social media frequently portray mental illness as leading to unstable and frightening behaviors, and some healthcare professionals may believe that hospitalized patients with mental illness are dangerous or unable to understand their medical care. However, not all mental illness results in psychosis or aggression. It includes diagnoses of depression, anxiety, bipolar disorder, substance use disorder, schizophrenia, schizoaffective disorder, and neurocognitive disorders. (See Mental illness stats.)
Mental illness stats
The World Health Organization reports that close to one billion people worldwide have some form of mental illness. According to the National Institute of Mental Health, 51.5 million of them are in the United States, and the American Hospital Association estimates over 36 million yearly hospital admissions. This means that many nurses who work on acute care units will care for patients with mental illness.
A multiyear study by Scott and colleagues found that 53% of hospitalized patients were diagnosed with a mental health disorder during hospitalization. The most common diagnoses included depression, neurocognitive disorders (primarily delirium), anxiety, substance use disorders, and schizophrenic spectrum disorders. Walker and colleagues found that rates of depression range from 5% to 34% in general hospitalized patients. These figures seem to indicate that mental illness among the 36 million hospitalized patients is common and should be part of a comprehensive nursing care plan.
Relationship between mental and physical illness
According to NIMH, patients with chronic medical conditions (such as autoimmune disorders, cardiac conditions, hypothyroidism, and diabetes) are at a higher risk of depression. Some patients may have depressive symptoms related to a newly diagnosed medical illness such as stroke or HIV. Alternatively, patients with depression may be at a higher risk of developing medical conditions such as cardiovascular conditions and diabetes, and some evidence points to patients with depression having a higher incidence of osteoporosis. A medical condition may be a direct result of depressive symptoms, which can hinder self-care (including keeping regular medical appointments, taking medications appropriately, healthy eating, and exercising).
Patients with severe mental illness may find that previously controlled symptoms (such as hallucinations, delusions, mania, anxiety, or depression) resurface during hospitalization. Changes in the patient’s environment and daily schedules may be the cause. Renewed symptoms also may be related to interrupted medication regimens. As much as possible, psychiatric medication should be continued during hospitalization.
Psychiatric symptoms, not care refusal
Nurses and other healthcare providers may misinterpret psychiatric symptoms as refusing care. Take the time to consider how a patient’s mental illness may disrupt their ability to follow treatment recommendations. For example, extreme anxiety may prevent a patient from having a procedure or an exam, or they may be afraid to learn the results of a diagnostic test. If a patient is depressed, they may refuse to eat, take prescribed medications, or participate in physical therapy. These patients aren’t being difficult, they have an illness that interferes with care.
A patient with a neurocognitive disorder, such as dementia, may have language challenges that prevent them from expressing themselves clearly or memory deficits that hinder their ability to remember treatment recommendations. These patients may require frequent redirection and reeducation. Patients with dementia are at a higher risk for developing delirium during a hospitalization. (See Dementia vs. delirium.)
Dementia vs. delirium

Delirium, which includes symptoms such as confusion, disorientation, memory impairment, hallucinations, and paranoid thinking, may be mistaken for a psychiatric disorder. If the acute care team doesn’t know the patient, they may have difficulty distinguishing between delirium and dementia.
Dementia, a progressive brain disorder, generally has a gradual onset and doesn’t respond rapidly to medical or pharmacologic treatment. Nurses must care for patients with compassion and patience.
Delirium, which usually has an acute onset, typically results from electrolyte imbalances, metabolic disturbances, infectious processes, medications, pain, or major organ issues. Delirium also can result from being in an unfamiliar environment such as an intensive care unit. As the patient’s medical condition improves, their delirium symptoms should dissipate.
Care on the acute medical unit
Many people with psychiatric illnesses, some of whom report that they feel medical health professionals dismiss their physical complaints as symptoms of their mental illness, don’t seek healthcare out of fear that they won’t receive appropriate treatment. According to Knaak and colleagues, a Canadian Psychiatric Association survey showed that 79% of healthcare professionals discriminated against a patient with a mental illness and 53% observed discrimination. To ensure holistic care, nurses, providers, and healthcare organizations must address the stigma associated with mental illness, implement mentoring and education programs to improve nursing skills and confidence, enhance patient and team communication, and alter settings as appropriate.
Reduce the stigma
Stigma (labeling, stereotyping, or discrimination) related to mental illness can create fear, marginalization of patients who frequently visit their provider or the emergency department, and ultimately poor health outcomes. Significant health issues may be overlooked because medical professionals dismiss physical complaints as a manifestation of a psychiatric disorder.
Start by acknowledging that negative attitudes toward patients with mental illness exist. Perform a self-appraisal and ask yourself these questions: Do I have negative thoughts about people with mental illness? Have I made jokes or disparaging comments about patients with mental illness? Have I refused to care for or complained about caring for patients with mental illness? Answering yes to any of these questions may mean that your feelings interfere with the care you provide.
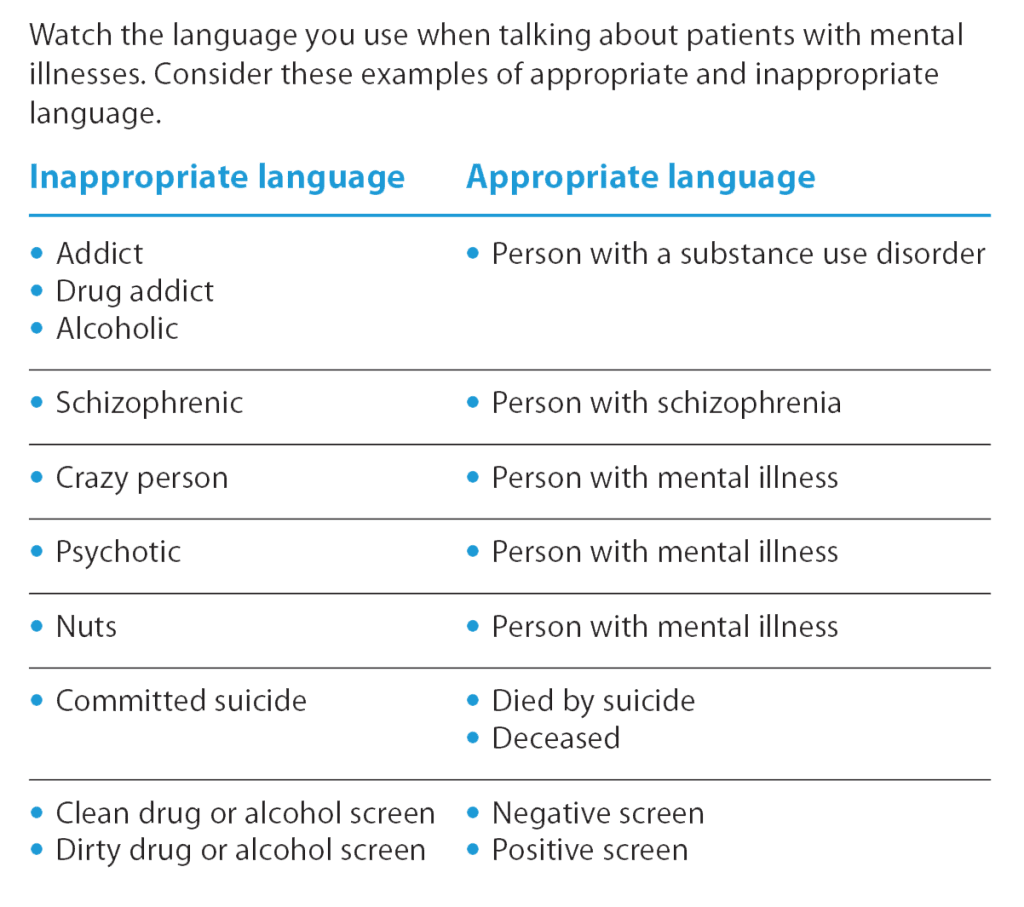
NIMH recommends talking about mental illness openly to help normalize it. According to Nyblade and colleagues, one of the most effective ways of reducing stigma among healthcare professionals is to provide education about specific disease states and the effects of stigma on outcomes. Education can include structured activities that allow healthcare professionals to develop skills for working with patients with mental illness. For example, members of the stigmatized group can meet with healthcare professionals to discuss concerns, including appropriate and inappropriate language. (See Choose your words wisely.)
Choose your words wisely
In addition, organizations should develop policies aimed at eliminating discrimination. Leadership must set the example of respect for all employees to follow.
Education and mentoring
Several studies indicate that some nurses believe they don’t have the skills to assess or communicate effectively with patients with mental illness. According to Avery and colleagues, nurses who feel unprepared report that caring for patients with comorbid mental illness is stressful, difficult, and unrewarding. Mentoring (including emotional support, guidance, modeling, and evidence-based knowledge) from experienced nurses can help increase confidence and improve care.
Education (including nursing school, continuing education outside of the hospital setting, and in-house programs) also can improve nurse confidence. Several private companies offer formal curriculum related to topics such as de-escalating aggressive patient behavior and effective communication. Organizations should consider offering this education during all new employee orientation and at annual updates.
Effective communication
Quality care requires effective communication with patients and colleagues. When communicating with patients, develop a therapeutic rapport and maintain a professional demeanor, regardless of the patient’s behavior. Don’t argue with patients, demean them, or use offensive language. Training in communication techniques, such as motivational interviewing, can help improve your ability to relate to and address patient concerns.
Nurses spend the most time with patients, which means they can provide critical information to the entire treatment team. To address patient and family concerns and improve care, share what you learn during patient interactions. For example, if a patient expresses distrust in a specific staff member, ask if someone else can care for the patient. If a patient doesn’t want to take medications three times a day, discuss dose adjustment options with the provider. If a patient doesn’t like the taste of a medication, determine if it can be taken mixed with food. To address confusion, remind all staff to orient the patient by reintroducing themselves each time they enter the room. Ask for assistance if a patient becomes aggressive or agitated or if you need a break. Discuss the possibility of consulting psychiatric services and consider having a staff member or a sitter stay with the patient to ensure safety. (See Improve patient communication.)
Improve patient communication
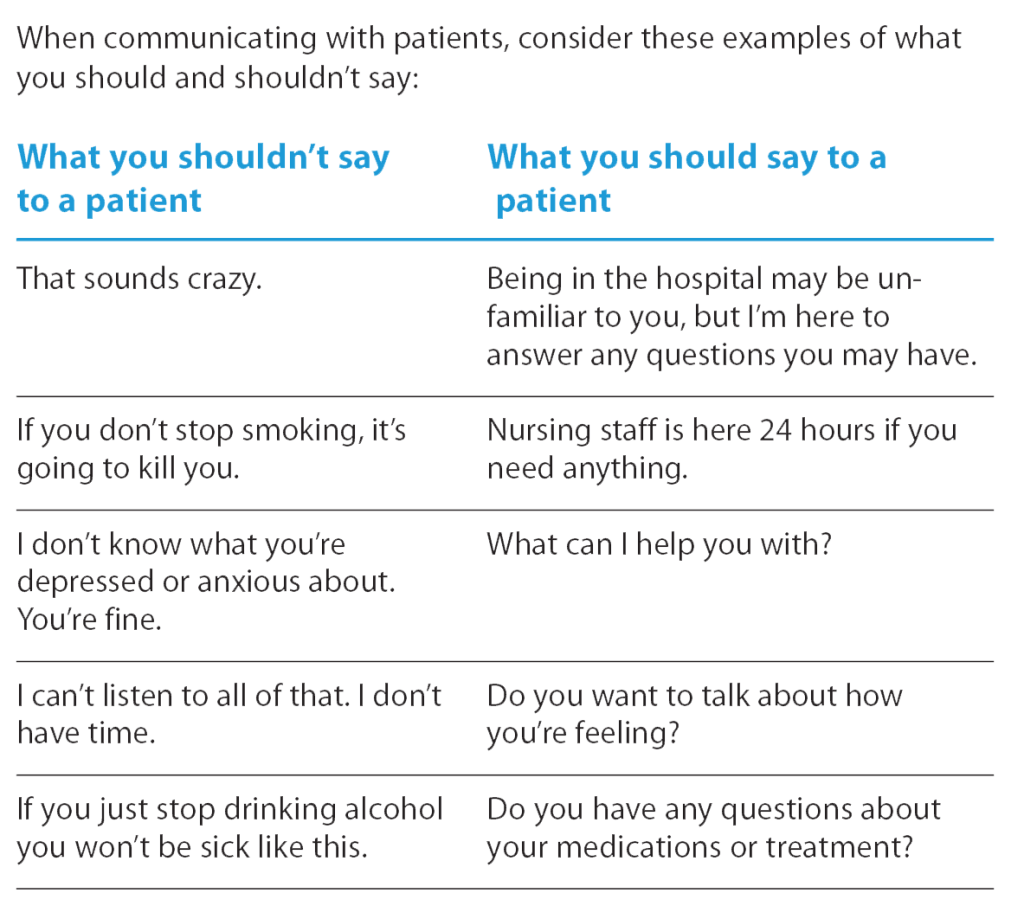
In addition, encourage patients to talk about their feelings, concerns, and fears.
- In an unfamiliar hospital environment, patients may be too anxious to ask questions. Take time to ask the patient how they’re feeling about an upcoming surgery, a recent diagnosis, going home alone, being in the hospital, or any other aspect of their medical condition.
- Ask the patient how you can help.
- Listen to the patient.
- Paraphrase what you hear to ensure you’ve accurately understood their concerns.
- Tell the patient you appreciate that they shared their feelings so they know someone is paying attention.
Improve the environment
You may not be able to physically change the hospital environment, but you can take steps to reduce anxiety and confusion. For example, when the patient arrives, familiarize them with the room and describe the purpose of each piece of equipment. Explain that alarms may sound but that the nursing staff will address them. To keep the patient oriented to time and place, update an orientation board daily and open the window blinds during the day and close them at night. Explain nighttime disturbances and try to time care for when the patient isn’t resting. If the room door must stay open, explain why. To reduce depressive symptoms or anxiety, inform the patient of visitation policies and encourage them to bring familiar and comforting items, such as blankets or pillows.
Interventions
To enhance care, perform appropriate assessments and take steps to alleviate mental health symptoms.
Depression.
Assess patients for thoughts of death or suicidality by asking direct questions, such as “Are you having thoughts of suicide?” Actively initiate conversations and share any concerns based on your observations (“I see that you haven’t been eating any of your meals. Has your appetite decreased?” “I noticed that you were tearful when talking about the surgery. Are you depressed or anxious?”). If necessary, help patients with activities of daily living, such as bathing, oral care, or hair grooming. Talk to the patient about how depressive symptoms can interfere with managing their physical illness.
Anxiety.
To help relieve a patient’s anxiety, use grounding techniques such as touch (with permission), being fully present with the patient, deep breathing, and guided imagery. Some patients may be defensive, but don’t argue or debate. If possible, reduce sensory stimuli and provide a calm environment. For example, play soothing music and dim the lights. If possible, keep “threatening equipment” out of sight and lower alarm volume. If the patient is in a room near a high-activity area, see if they can be moved. Take time to listen to the patient express their feelings about anxiety. If the anxiety is a rational response, normalize their feelings. If it’s an irrational response, comfort the patient. In addition, when explaining tests and procedures, speak calmly and slowly and use nonmedical terms.
Dementia/delirium.
Assess all patients for delirium, especially those at high risk, and discuss any concerns with the attending provider. To promote patient safety, remove potentially dangerous objects from the room. Always stay calm and reassuring and provide a soothing environment when possible. Encourage family visits, reassure the patient that they’re safe, provide accurate information on the orientation board, and place familiar personal belongings in the room. If the patient uses glasses or hearing aids, ensure they’re nearby. Use nonmedical terms when explaining the patient’s condition and care steps. To avoid cultivating false ideas, talk to the patient about real people and real events. Some patients with dementia/delirium may need assistance with activities of daily living, and fall prevention protocols may be required. If necessary, discuss assigning a 24-hour staff member for the patient and alert all staff to the patient’s mental health condition.
Substance use.
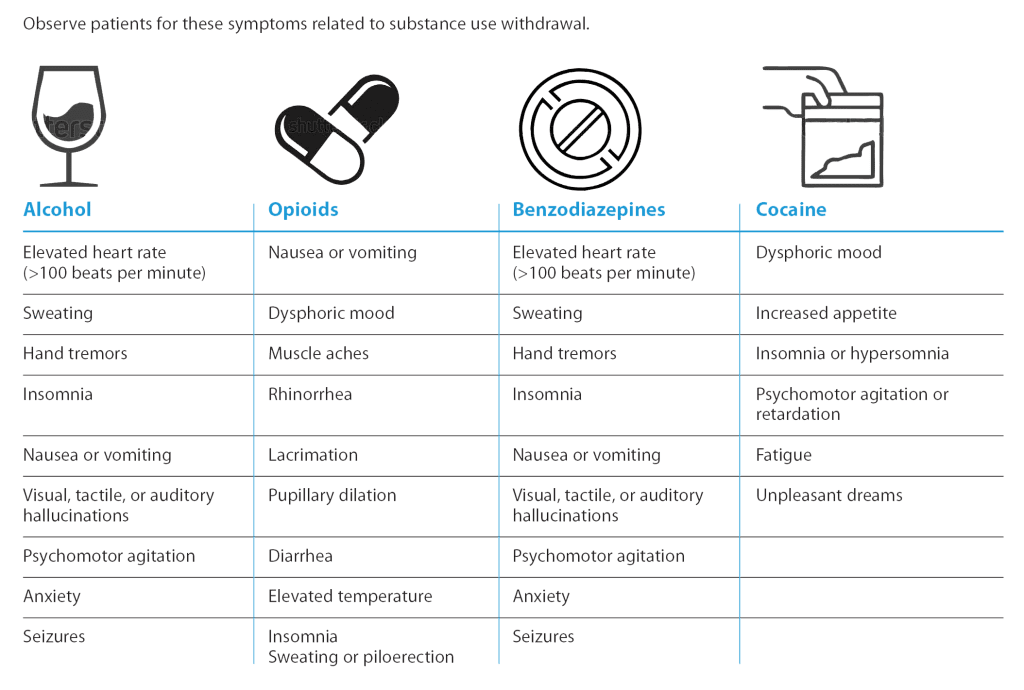
Assess all patients for substance use, but keep in mind that they may not be forthcoming. Some patients may not report that they drink alcohol daily, or their medical condition may prevent them from providing an accurate medical history. Patients may not view prescribed medications as having the potential for misuse and those who use illicit drugs may fear legal consequences. For these reasons, monitor for signs and symptoms of withdrawal. Some patients may be fearful that they’ll experience withdrawal during hospitalization, so explain how symptoms can be treated. After the patient’s medical condition has stabilized, provide them with information about substance use treatment. (See Withdrawal symptoms.)
Withdrawal symptoms
Schizophrenia or psychotic disorders.
Patients with schizophrenia or psychotic disorders may require orientation to reality and reassurance that they’re safe in the hospital. If the patient exhibits psychotic symptoms, alert the attending provider. Patients with these conditions may require a 24-hour staff member.
Agitation.
When caring for patients who may become agitated, assess them frequently and ask coworkers for help in resolving situations before agitation occurs. Remove any potentially harmful objects from the patient room, and reduce external stimuli. If a patient does become agitated, use verbal redirection and de-escalation techniques (speak clearly and in a low voice, respect personal space, maintain eye contact, set clear limits that the patient understands, explain what’s going to happen next, and offer alternative options). As ordered, administer medications that may help calm the patient. If symptoms are noticed early, oral medications are effective. If possible, avoid using physical restraints, which can potentially harm the patient and may place staff in harm’s way while trying to apply them. The Centers for Medicare and Medicaid Services guidelines state that physical restraints can’t be used when a patient refuses care or as punishment.
Prepared to care
Nurses must be prepared and confident to care for patients with comorbid psychiatric illness in the acute care setting. Preparation begins by acknowledging your concerns and possible biases, reducing the stigma associated with mental illness, obtaining mentoring and education, implementing effective patient and staff communication, and ensuring a safe and comfortable environment.
Christy Perry is an assistant professor at Southeastern Louisiana University in Hammond. Sattaria Dilks is department head of graduate nursing at McNeese State University in Lake Charles, Louisiana.
References:
American Hospital Association. Fast facts on U.S. hospitals, 2022.
Angel C, Brooks K, Fourie J. Standardizing management of adults with delirium hospitalized on medical-surgical units. Perm J. 2016;20(4):16-002. doi:10.7812/TPP/16-002
Appold K. Experts suggest ways to deal with challenges surrounding care of psychiatric patients. March 16, 2016. The Hospitalist.
Avery J, Schreier A, Swanson M. A complex population: Nurse’s professional preparedness to care for medical-surgical patients with mental illness. Appl Nurs Res. 2020;52(3): 151232. doi:10.1016/j.apnr.2020.151232
Clement S, Schauman O, Graham T, et al. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol Med. 2015;45(1):11-27. doi:10.1017/S0033291714000129
Knaak S, Mantler E, Szeto A. Mental illness-related stigma in healthcare: Barriers to access and care and evidence-based solutions. Healthc Manage Forum. 2017;30(2):111-16. doi:10.1177/0840470416679413
Lippmann S, Perugula ML. Delirium or dementia? Innov Clin Neurosci. 2016;13(9-10):56-7.
National Institute of Mental Health. Mental illness. January 2022.
Nyblade L, Stockton MA, Giger K, et al. Stigma in health facilities: Why it matters and how we can change it. BMC Med. 2019;17(1):25. doi:10.1186/s12916-019-1256-2
Roppolo LP, Morris DW, Khan F, et al. Improving the management of acutely agitated patients in the emergency department through implementation of Project BETA (Best Practices in the Evaluation and Treatment of Agitation). J Am Coll Emerg Physicians Open. 2020;1(5):898-907. doi:10.1002/emp2.12138
Scott G, Beauchamp-Lebrón AM, Rosa-Jiménez AA, et al. Commonly diagnosed mental disorders in a general hospital system. Int J Ment Health Syst. 2021;15(1):61. doi:10.1186/s13033-021-00484-w
Thornicroft G, Mehta N, Brohan E, Kassam A. Stigma and discrimination. In: Morgan C, Ghugra D, eds. Principles of Social Psychiatry. Chichester, UK: John Wiley & Sons, Ltd; 2010; 331-40.
Ungar T, Knaak S, Szeto ACH. Theoretical and practical considerations for combating mental illness stigma in health care. Community Ment Health J. 2016;52(3):262-71. doi:10.1007/s10597-015-9910-4
Walker J, Burke K, Wanat M, et al. The prevalence of depression in general hospital inpatients: A systematic review and meta-analysis of interview-based studies. Psychol Med. 2018;48(14):2285-98. doi: 10.1017/S0033291718000624
World Health Organization. Key messages.
Key words:
psychiatric care, inpatient care, mental illness, comorbid mental illness, acute care


















2 Comments.
Very comprehensive yet specific need to know information.
This article is informative and will help me to better take care / understand my patients.