
Support comes from many sources.
- Nurses reported that primary supportive factors that help prevent burnout include their relationships with friends, loved ones, colleagues, patients, and their community.
- These connections allow for greater workplace engagement, which can lead to improved patient outcomes.
“Hello, I’ll be your nurse today.” These six words signal to a nurse’s brain that they’re no longer an individual but rather part of a collective engaged in a fascinating rollercoaster of assessment, intervention, and evaluation of the human experience. As part of this collaborative endeavor to address obstacles to health, others frequently examine individual nurses through the lens of the nurse–patient relationship. However, the effects of personal and professional relationships on nurses themselves require better documentation. Moving out from under the shadow of the COVID-19 pandemic, nurses have spotlighted some hard-won insights. I highlighted these insights in this summary of findings from a qualitative, interpretive phenomenological study, which used hermeneutics (interpretation of written or spoken language) to identify emerging themes of the lived experience of intensive care unit (ICU) nurses.
Uncovering the nurse experience
The COVID-19 pandemic pushed many nurses to their breaking point; this trial by fire burned away the extraneous façade of nursing to reveal the strength at the core of many nursing professionals. You’ll find much in the current literature about the initial impact of chronic exposure to traumatic events while caring for patients with COVID-19 in frontline healthcare workers. In what has been dubbed “The Great Resignation,” many nurses have examined their commitment to the profession and what they need for the best quality of life. Experienced and novice nurses have reflected on what helped them endure one of the most chaotic and high-pressure settings in pandemic history. In this study, I sought to illuminate not only the rote experiences of these nurses but also the motivation behind those resilient enough to endure the effects of the pandemic and remain in the field.
Methods
In this qualitative, interpretive phenomenological inquiry, I aimed to learn about the lived experiences of ICU nurses throughout the United States. I used Heideggerian hermeneutics to illuminate emerging codes and themes, as well as Patricia Benner’s method for data analysis with interpretive phenomenology. I chose these methods because they’ve been used extensively within the profession to illustrate the science and art of nursing. The rationale included the consideration that caring for patients with COVID-19 tested both the logical and emotional talents of nurses.
After the University of Southern Mississippi internal review board considered and approved this study, I recruited the sample population (ICU nurses from across the United States) using professional organizations, social media, and snowball sampling. (See Data collection and analysis.)
Data collection and analysis
Nurses indicated their initial interest and consent to participate in this study via a Qualtrics survey. They answered questions about demographics and scheduling for future recorded online interviews using the following structure:
- Semi-structured interviews, conducted via Zoom, for a duration of approximately 30 minutes
- Transcribed audiovisual data from recordings for data immersion and identification of preliminary codes
- Data analysis conducted using the Heideggerian framework for the hermeneutic circle and Benner’s method for data analysis of interpretive phenomenology
- Member checking performed to ensure accuracy of identified emerging themes
I applied the hermeneutic circle to data as follows:
- Reflection on the understanding of the lived experience
- Application of situational context
- Reflection and analysis of emerging parts of the lived experience
- Reintegration of new understanding with context into the whole
- Repetition to facilitate the emergence of meaning
I applied Benner’s method of interpretive phenomenological analysis as follows:
- Analysis of data for themes
- Global assessment, emerging codes identified to direct future data collection
- Lines of inquiry used to design interpretive plan based on patterns
- General categories formed based on re-integration of new data
- Analysis of key incidents
- Situations grouped to identify environment and participant similarities
- Exemplars classified into strong intention within the narrative
- Search for paradigm
- STranscripts reviewed for patterns of meaning, rich descriptions, and situational context
Sources of support
I interviewed 20 ICU nurses who cared for patients with COVID-19 in various settings across the country. They identified relationships with friends and loved ones, their community, colleagues, and patients as primary factors in supporting them through horrific working conditions and sobering patient outcomes. The nurses reported that supportive relationships provided protection against compassion fatigue and burnout and also played a key factor in enabling them to stay in the profession. Moving toward a better and brighter future, these insights have the potential to improve nursing professionals’ quality of life, bolster nurse morale, support nursing workforce retention, and promote healthy work environments. (See Nurses’ voices.)
Nurses’ voices
Interviews with nurse participants provided insight into the importance of support from friends and loved ones, colleagues, patients, and the community.
Friends and loved ones
- “I have a really supportive husband…. I feel like he’s just been a great support, and so on those days that are like particularly hard… he’s just really supportive. He’ll ask, ‘Okay, do you want to talk it out? What can we do?’ I feel like he’s always been that way, but I feel like he stepped into a really supportive role on a more daily basis.” (Nurse #7)
- “They [family] understood I couldn’t just quit nursing and not take care of these patients. Nobody signed up for a pandemic, but it’s just what we have to do…. We have to take care of these patients. So, my family was very supportive, and my extended family was very supportive.” (Nurse #10)
- “I had some reach out to me to say, ‘Hey we’re praying for you.’ [tearfully] At least in my family they would reach out to say they were praying for me and to hang in there.” (Nurse #8)
- “I asked my spouse if I became distant from her. She said no, but that it did feel like every single off night was a debrief…and I wasn’t trying to! I didn’t tell her a lot of stuff. What would be the point of telling specifics and making someone else as miserable as you? But…I guess I talked about it more than I thought that I did.” (Nurse #18)
Community
- “Sometimes they would make [thank-you] signs and put them in the parking lot. It was a nice gesture that made it a little easier to have positive thoughts and know that someone did notice…that they did care about us…elementary kids writing [thank-you] letters really touched our hearts. It helped me, and a lot of us, to feel like we could keep going.” (Nurse #15)
Colleagues
- “One thing that I’ve seen that has been maybe just a little glimmer of good is the ICU nurses were always very militant kind of like, “Suck it up…you can do anything for 12 hours.” Remember? That goes through our heads; that’s literally how we’re trained. Then recently in the last 6 months, people have been like, ‘I’m suffering,’ and mental health is not as stigmatized as it has been for so long. ICU nurses…we never talked about our pain or our trauma. We never talked about how it was to code an old man and feel every bone pop in his body…. If there’s any glimmer of hope I think ICU nurses are being more open with their mental health crises.”
- “Honestly, people don’t want to deal with how intense this stuff is… the people who are outside of our team. We can’t talk to anybody else besides a trained provider, mental health provider. We can talk to each other. So, we’re closer than ever and that at least is wonderful.” (Nurse #3)
- “I can’t tell you how many coworkers I’ve cried with. There’s this reassurance from hearing what my coworkers are venting about, and I can finish their sentence in my head because I feel the exact same way.” (Nurse #4)
- “I absolutely love who I work with and that’s why I’ve stayed where I’m at.” (Nurse #7)
- “I’ll always want to keep track of this group of people, probably for the rest of my life, because we’ve shared this experience and things that no one else can understand.” (Nurse #12)
- “They understood everything that you felt, and everything that you were going through and what you needed.” (Nurse #18)
- “Now you are always on the lookout or listening out to see if anybody you know needed help.” (Nurse #3)
- “Before the pandemic, if someone poked their head out of their room and was like, ‘Hey, I need this,’ people would be like, ‘Get it yourself.’ Now someone pokes their head out and everyone is like, ‘Hey, what do you need? What can I get you?’ and that’s just a basic change.” (Nurse #4)
- “We were trying to be very helpful for each other… just because some of these patients were a lot of work. You had to be in tune with each other. Everybody has to be a team player and help each other out.” (Nurse #10)
- “We have to take care of each other.” (Nurse #13)
- “The good things were the positivity that we would see in some caregivers…stepping up and being there for each other and really helping each other out with little things to make each other’s day a little brighter.” (Nurse #15)
- “…our leadership tells us to call our counseling office for debriefing, but then when they get there into the room full of freshly traumatized healthcare providers who start talking about what happened…they shut it down every time…. The only thing that people [nurses] get out of these group counseling sessions is that they can see by the number of people that…they’re not the only one that is hurting. Some of us have been doing this for more than a decade. We have a lot of new ones [nurses], but I mean, most of us have been doing this for more than a decade. We have a lot of barriers that you have to bring down, and then some of that is stoicism. Plus, this is just what we do…but we’re all still human beings. At least we can talk to each other…. We’ve started our own little debriefings together, and that’s honestly been what has helped the most.” (Nurse #5)
Patients
- “You have this very guarded sick person who has no idea what’s going on with them. You’re coming in their room in this get-up and I think that for them [the patient] it’s that moment of, ‘How do I let this person in and trust them when they act like I have the plague and won’t even touch me?” (Nurse #13)
- “It’s just a long process…so you become way more invested in them and that aspect of it really doesn’t ever get easier because you really do form an attachment.” (Nurse #17)
- “I try to not let my heart get calloused. Like, ‘You might pass away, or you might have a bad outcome so I’m just not going to get to know you at all.’ I don’t want to be like that.” (Nurse #7)
- “I found that it was hard to convince patients to do the treatments when they didn’t believe in the virus.” (Nurse #12)
- “We had a really good relationship with the patient, and they were very grateful for the care that we gave right up until the moment that the patient passed.”(Nurse #14)
- “We had an example of a patient that needed some blood, and they went as far as to ask, ‘Has the donor of this blood had the vaccine? If they’ve had the vaccine, then I don’t want that blood.” The patient really needed the blood, they were very anemic. Whether or not a blood donor had been vaccinated should have been a non-issue. Just really strange ideas…it makes me think; are we really to this point? Sometimes their families would tell us, ‘The treatments you’re doing are killing them.’ That really, really affected me.” (Nurse #15)
- “They [patients] asked us [when getting meds], ‘What are you pushing? Are you trying to sneak me the COVID vaccine?’” (Nurse #11)
- “I’ve been a nurse for going on 17 years, and I’ve never been involved with patients that are saying, ‘Hey, I’ve done all this research, and we’re not going to take this medication. We want to take this medication [instead].’ It’s a very new dynamic…they really think we’re trying to kill them…and these people do not cope well. We see people that basically die because they can’t manage their anxiety, and we can’t manage their anxiety for them, and therefore they aren’t able to tolerate the care that they need.” (Nurse #16)
- “The ones that feel like you have done something to make their loved one worse, or you’re not doing enough, or they’re on the internet reading about all these other types of treatments that are not recommended, and they want you to do those things. Then, you know, they’re calling you all confident and just using negative words that you shouldn’t have to put up with when you’re on the job. The words aren’t so bad as when they start threatening, you know, and saying they’re going to come back for you after work. We’re here taking care of your person, and then you threaten the healthcare people. It’s just…it’s crazy.” (Nurse #3)
Family, friends, and the community
Nurses who felt that their family and friends provided meaningful support for their efforts in the workplace said they were more likely to continue caring for patients. Those whose families understood their dedication felt more fulfilled. Overall, the quality of relationships with family and friends held significant weight in nurses’ perceptions of their mental and emotional ability to care for patients.
This support and understanding included having loved ones ask if they wanted to talk about their day or other challenges from work. Nurses who participated in the study described therapeutic listening from family and friends as important as debriefing on the job. Other nurses said that having family or friends reach out with words of encouragement, comfort, and support helped them feel debriefed in a safe setting with people they trusted.
Community support played a significant role in the morale and resiliency of these ICU nurses. Nurses shared that their communities’ efforts made it easier to face challenges throughout the day and feel seen and appreciated. One nurse described elementary school children sending letters with encouraging hand-drawn pictures or words.
Colleagues
Many nurse participants described being “bonded” with their colleagues, which I classified into the following subthemes: supporting each other, helping out, and opening up. Several nurses described caring for patients during the pandemic as similar to the bonding that soldiers experience while protecting each other and serving in battle. They explained that opening up, helping each other, and supporting each other fostered greater strength than they would have possessed alone.
One nurse said about her coworkers, “They understood everything that you felt, and everything that you were going through and what you needed.” Another nurse shared, “The good things were the positivity that we would see in some caregivers…stepping up and being there for each other and really helping each other out with little things to make each other’s day a little brighter.” These statements illustrate the strength and resiliency that nurses found meaningful as they worked with their teams.
Nurses also reported that they found healing power in grieving together, which resulted in the ability to find hope and positivity. One of the biggest opportunities for bonding occurred during debriefing events. One nurse recalled, “ICU nurses were always…kind of like, ‘Suck it up, you can do anything for 12 hours.’ That’s literally how we’re trained…[but] mental health is not as stigmatized [now] as it has been for so long. We never talked about our pain or trauma. We never talked about how it was to code an old man and feel every bone pop in his body…. If there’s any glimmer of hope, I think ICU nurses are being more open with their mental health crises.” This statement indicates a willingness to share traumatic experiences, which hasn’t always been the case with nurses.
Patients
Nurses reported that finding connections with their patients, despite the outcomes, brought them a sense of purpose and peace. The nurse participants explained that they could ask patients to trust them only after first being willing to connect with them on a personal level during their care. Despite the pain of potentially losing patients, threats of abuse or harm, and rampant medical mistrust, these nurses continued to list quality nurse–patient relationships as a protective factor against leaving the nursing profession.
Implications for nurse leaders
Nurse leaders can promote positive working relationships among unit staff by modeling authentic leadership. Getting to know each nurse individually and asking about their experiences show genuine concern and investment in them as a person and a professional.
Safe, quality debriefing sessions provide significant support. Each nurse experiences a single patient event differently based on their backgrounds, experiences, and coping mechanisms. For this reason, providing a psychologically safe debriefing space will help nurses express emotions, thoughts, and feelings. Some nurses may focus on reviewing the technical aspects of the event and marginalize their emotions. This doesn’t negate the value of the debriefing. Nurses are trained to approach situations with logic and compassion. Debriefing should include both elements.
Appointing a morale council of peers also may contribute to better awareness and engagement in quality relationships. The members of the council assess unit morale and plan meaningful recognition. Study participants reported that involving the community in recognition and interventions designed to raise staff morale helped them feel seen and appreciated. Recognizing and celebrating personal and professional accomplishments as a team can foster quality interpersonal relationships and strengthen colleague bonding.
Nurse leaders also must ensure that bedside nurses participate in opportunities to balance work challenges with personal needs. Such balance includes adequate resources to take regular bathroom breaks, participate in rotating lunch hours, make use of their vacation time, and attend to their own personal and family emergencies.
These interventions can contribute to the nurses’ overall perception of a healthy work environment. They also have the potential to promote professional quality of life, improve patient outcomes, and encourage nurse retention. (See A little help in your back pocket.)
A little help in your back pocket
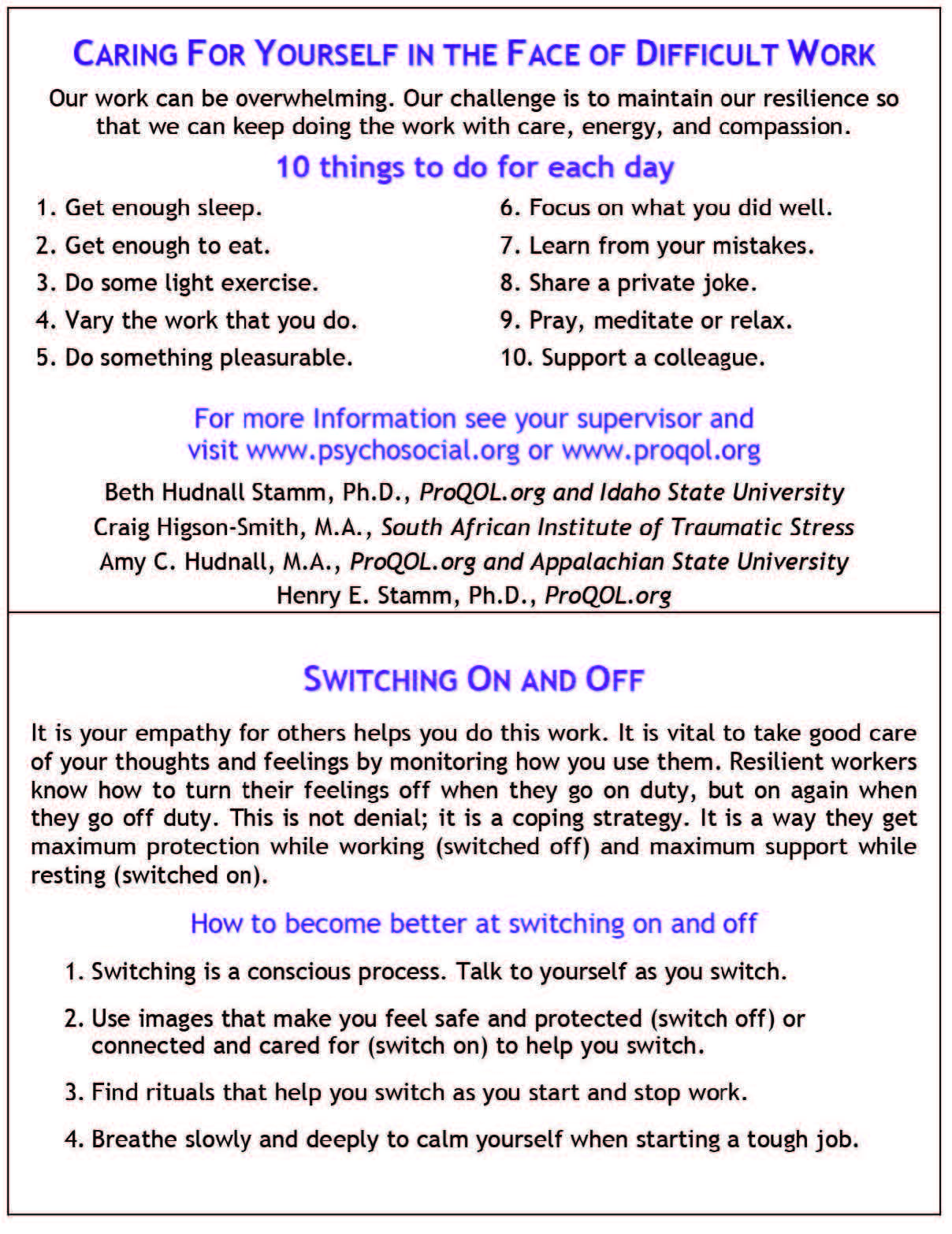
The Helper Pocket Card, designed by Dr. Beth Hudnall Stamm, a trauma-informed care expert and creator of the Professional Quality of Life survey, is one of the most widely used tools to gauge compassion fatigue in nursing. One side of the card lists 10 ideas nurses can implement to care for themselves while performing difficult work. The other side offers techniques for focusing on empathy and shifting between work mode and home mode.
Implications for nurses
Nurses can implement the findings from this study in their personal and work relationships to promote a good professional quality of life and a healthy work environment. Start by setting clear boundaries between job responsibilities and home life. Make time for family and friends who help lift and encourage you personally and professionally. Prioritize connecting with people who bring positive emotions—through video or phone calls, emails, and visits—to help strengthen interpersonal relationships.
Engaging in positive coping behaviors (alone and with others) can promote your professional quality of life. Examples of positively perceived individual coping behaviors include listening to music, spending time in nature, exercising, reading for pleasure, writing creatively, learning a new hobby, prioritizing sleep, focusing on positive thoughts, gratitude journaling, meditating, watching relaxing videos, and using stress and anxiety management apps. Activities you can do with others include participating in discussions or informal conversations, taking walks or running, starting a new hobby together, getting involved in a unit-based sports team or book club, attending weekly movie outings, or attending professional events (virtually or in person).
Nurses also can build quality relationships with others by making a concerted effort to support their colleagues. This includes new hires and veteran nurses, as well as temporary and permanent staff. Every nurse has valuable experience that others can learn from. Recognizing that each nurse is at a different point in their professional journey can foster camaraderie and promote a successful team. Likewise, modeling positive behaviors and relationships can help set the tone for a thriving team culture.
Implications for family and friends
Nurses’ families and friends want to provide support but may not know where to start, and sometimes nurses have difficulty recognizing when they need support. Nurses who want to increase their overall resiliency and professional quality of life will benefit from nurturing supportive relationships with their friends and loved ones. I recommend that friends and family use POLST (Patience, Openness, Listening, Supporting, and Time) to help nurses they love. (See POLST.)
POLST
Share the following with family and friends so they can better support you during difficult times.
- Patience: As much as possible, be patient with each other. Remember that each family member processes challenging situations differently. It can take time for nurses to be ready to open up or connect with their own friends and family, especially after a traumatic experience.
- Openness: Keep an open mind about developing connections. Ideal supportive responses and experiences may not be immediate on either side, but when they finally surface, the connection and long-term benefits are worth the wait for both parties.
- Listening: Family members and friends of nurses can help by listening when the nurse wants to work through the challenges and emotions of the day out loud. Frequently, this is the first time that a nurse has allowed themselves to look at their own experience in a safe place.
- Supporting: Having the support of friends and family can mean much more to nurses than is realized. Strive to be present and offer encouragement during your time together.
- Time: Spend time together, and as much as you can, try to make that time a positive experience.
Make the connection
Nurses indicated that primary supportive factors preventing nursing burnout include their relationships with friends, loved ones, colleagues, patients, and their community. These connections help nurses feel supported, which aids workplace engagement and improved patient outcomes.
Nurses reported that connections with team members provided profoundly meaningful support, primarily due to shared experiences. They also explained the negative effects associated with lack of debriefing after a stressful or traumatic incident. They considered open communication (including conversations with a mental health professional) as therapeutic and described sharing thoughts and feelings with their peers as beneficial to building better nursing connections and allowing them to heal and gain a sense of meaning. For all nurses, from novice to expert, these findings indicate key actions and relationships that can help prevent burnout and promote professional quality of life, even in challenging circumstances.
Adrianna Lorraine Watson is an assistant teaching professor at Brigham Young University in Provo, Utah.
American Nurse Journal. 2024; 19(2). Doi: 10.51256/ANJ022426
References
Benner PE. Interpretive Phenomenology: Embodiment, Caring, and Ethics in Health and Illness. Thousand Oaks, CA: Sage Publications; 1994.
Heidegger M. On Time and Being. New York, NY: Harper & Row; 1972.
Hu Z, Wang H, Xie J, et al. Burnout in ICU doctors and nurses in Mainland China—A national cross-sectional study. J Crit Care. 2021;62:265-70. doi:10.1016/j.jcrc.2020.12.029
Lyman B, Prothero MM, Watson AL. Building thriving healthcare teams through organizational learning. Nurse Leader. 2023;21(3):391-4. doi:10.1016/j.mnl.2023.02.007
Robinson KR, Gierach M, Bartelt S, et al. Battle of COVID-19: Frontline nurses feel abandoned during the pandemic. Am Nurse J. 2023;18(3):12-6. doi:10.51256/anj032312
Skarbek A, Mastro KA, Kowalski MO, et al. Nursing work environment staffing councils: An alternative to mandatory regulated staffing ratios. J Nurs Adm. 2022;52(7-8):419-26. doi:10.1097/nna.0000000000001175
Stamm BH, Higson-Smith C, Hudnall AC, Stamm HE. General helper card. Pro QOL. 2020. proqol.org/helper-pocket-card
Thrysoee L, Dyrehave C, Christensen HM, Jensen NB, Nielsen DS. Hospital nurses’ experiences of and perspectives on the impact Covid‐19 had on their professional and everyday life—A qualitative interview study. Nurs Open. 2022;9(1):189-98. doi:10.1002/nop2.1053
Ulrich B, Cassidy L, Barden C, Varn-Davis N, Delgado SA. National nurse work environments—October 2021: A status report. Crit Care Nurse. 2022;42(5):58-70. doi:10.4037/ccn2022798
Watson AL. The evolution of professional identity in intensive care nurses during COVID-19—An interpretive phenomenological study. Intensive Crit Care Nurs. 2024;80:103538. doi: 10.1016/j.iccn.2023.103538
Watson AL. The COVID-19 experience: An intensive care nursing perspective [dissertation]. Hattiesburg: University of Southern Mississippi; 2022.
Zhu X, Shepley MM. Assessing preferences and perceived restorative qualities of break spaces for nurses in China. HERD. 2022;15(3):126-42. doi:10.1177/19375867221075837
Zipf AL, Polifroni EC, Tatano Beck C. The experience of the nurse during the Covid‐19 pandemic: A global meta‐synthesis in the year of the nurse. J Nurs Scholarsh. 2021;54(1):92-103. doi:10.1111/jnu.12706
Key words: work engagement, compassion fatigue, morale, professional quality of life
















