
An intervention aimed at improving nurses’ ability to manage stress revealed the need for adaptation.
- This study provided unique insight into the ability of nurses to reduce stress by encouraging positivity thinking skills.
- Successful implementation requires adapting interventions to the needs of direct care nurses.
In 2022, our team (Keller and colleagues) reported on our first study examining the impact of a positive thinking skills training intervention designed to improve nurse leaders’ engagement and ability to cope with stress. We recognized that the stress experienced by nurse leaders (including nurse managers, assistant nurse managers, and unit educators) not only negatively impacts them but also has the potential to affect the nurses they serve.
In our first study, we conducted a randomized controlled trial to evaluate a positive thinking skills training intervention, which consisted of a 1-hour in-person class, daily affirmations sent to the nurse leaders for 1 month, and weekly homework designed to hardwire the positivity skills. This low-cost intervention resulted in increased use of positive thinking skills, enhanced engagement, and improved ability to cope with stress among nurse leaders.
In 2023, our organization, like many in the United States, began struggling with post-pandemic high turnover. Many nurses across the country report experiencing moderate-to-high levels of stress, which can increase nurse burnout, decrease job satisfaction, decrease organizational commitment, and increase intention to leave nursing. An analysis by Gallup named lack of employee engagement as a major risk factor for resignation.
To address these issues, we decided to replicate our nurse leader intervention with direct care nurses.
What did we do?
We used a cross-over controlled design to evaluate the positive thinking skills intervention on direct care nurses’ use of these skills as well as on their engagement and ability to cope with stress. Our organization’s Institutional Review Board approved the study.
To recruit direct care nurses for the study, we sent emails to all employees with eligible job codes. Eligible participants included clinical RNs who spend more than half of their time providing direct patient care and have been employed at our organization for at least 6 months. Members of the research team presented information about the study at nursing team meetings, retreats, and unit huddles. Nurses who indicated interest in participating signed an informed consent form. We then sent those nurses a 27-question baseline survey, which included the Positive Thinking Skills Scale, the Brief Resiliency Coping Scale, and a Workforce Engagement survey.
After nurses completed the baseline survey, they attended a 1-hour, in-person positive skills training class. We offered multiple class dates, times, and locations to make attendance as convenient as possible. The class encouraged self-reflection and promoted purposeful positive thinking. Participants engaged in exercises to identify positive aspects in their surroundings. The instructor introduced Bekhet and Zauszniewski’s eight positive thinking skills:
Transforming negative thoughts
Highlighting positive aspects
Interrupting pessimistic thoughts by using relaxation techniques and distraction
Noting the need to practice positive thinking
Knowing how to break a problem down into smaller more manageable parts
Initiating optimistic beliefs with each part of the problem
Nurturing ways to challenge negative thoughts
Generating positive feelings by controlling negative thoughts
Participants explored scenarios relevant to nursing and brainstormed possible positive responses. They also learned Achor’s happiness-promoting activities: gratitude, journaling, exercise, meditation, and random acts of kindness. To reinforce behavioral change, participants completed daily homework for 4 weeks, documenting their engagement in these activities. We designed the homework to help transform these skills into habits and integrate them into the nurses’ daily routines.
The final part of the intervention involved sending the participants daily positive affirmations. After attending the in-person session, we added the participants to a smartphone application, GroupMe, on their personal cell phones. Using this platform, we sent the nurses daily positive affirmations for 28 days after the class. The affirmations included messages such as the following: “The art of being happy lies in the power of extracting happiness from common things,” “Happiness is when what you think, what you say, and what you do are in harmony,” and “Start each day with a grateful heart.”
The nurses received the messages at random times throughout the day. The goal was to provide unexpected reminders to help the nurses refocus on the positive aspects of each day.
To assess sustainment of the positive-thinking skills the participants learned, we asked them to retake the same surveys they completed at baseline. We sent the surveys 1 month, 3 months, and 6 months after the intervention.
What did we learn?
A total of 69 direct care nurses enrolled in the study and signed up for the in-person class. Recruitment and enrollment of direct care nurses was similar to that for recruiting and enrolling nurse leaders. Direct care nurses seemed excited and eager to participate. However, after sending out the initial baseline survey, we noticed a stark difference between the nurse leaders’ and direct care nurses’ participation. Of the original 69 direct care nurses, 29 didn’t respond to the baseline survey and didn’t enroll in a class; we removed them from the study. Out of the 40 remaining nurses, nine didn’t attend a class. Of the 31 who completed the baseline survey and attended the class, only 12 completed all of the post-intervention surveys. (See Participant demographics.)
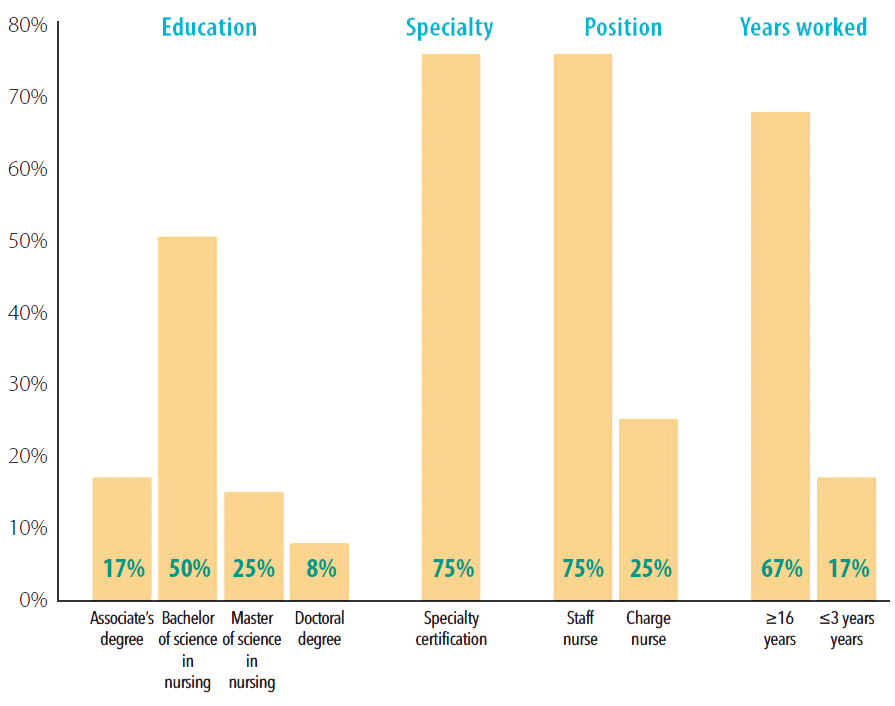
Participant demographics
Among the 12 nurses who completed the intervention and all surveys, we acquired the following demographic information:
The surveys measured positive thinking skills, ability to cope with stress, and participant engagement. Scores for positive thinking skills ranged from 0 to 24 with higher scores indicating more frequent use. For those nurses who completed the intervention and both pre- and post-intervention surveys, the frequency of using positive thinking skills increased from baseline (M=14.08, SD=3.03) at 1 month (M=17.75, SD=4.22, p<0.05), 3 months (M=17.67, SD=2.90, p=0.005), and 6 months (M=18, SD=3.54, p=0.011) post-intervention.
Scores for the ability to cope with stress ranged from 4 to 20 with a higher score indicating better coping ability. Participants’ ability to cope with stress also increased from baseline (M=14.33, SD=1.50) at 1 month (M=15.75, SD=1.82, p=0.037), 3 months (M=16.25, SD=1.29, p=0.005), and 6 months (M=15.75, SD=1.66, p=0.012) after the intervention.
Workforce engagement scores ranged from 6 to 30 with higher scores indicating more engagement. Nurse participants’ engagement didn’t significantly change from baseline (M=23.92, SD=4.36) at 1 month (M=24.75, SD=3.47), 3 months (M=25, SD=3.91), or 6 months (M=25.83, SD=4.20) post-intervention.
How can we adapt the intervention?
With regard to a sustained increase in the use of positive coping skills and improved stress management among direct care nurses, we achieved almost identical results as in our nurse leader study. We found a slight improvement in engagement among the nurse leaders, but the improvement wasn’t sustained over time; no significant improvement in engagement occurred among the direct care nurses.
Only four of the 58 nurse leaders who committed to the study didn’t complete it, but 57 of the 69 direct care nurses didn’t. We achieved positive results with the 12 nurses who did follow through; however, we learned that the intervention that worked so well with nurse leaders wasn’t as readily accessible and convenient for direct care nurses.
In both studies, we offered in-person learning and text message updates and reminders. However, the large completion difference led us to explore possible barriers to direct care nurses’ participation. Within our organization, many nurse leaders have on-site full-time day shift positions (Monday through Friday). Direct care nurses have varying shifts, work locations, and workdays. During the nurse leaders’ study, most participants could attend the education class during a scheduled workday. All direct care nurses had to come in on a day off, arrive early for a class offered immediately before a shift, or stay late for one held after a shift.
Communication also presented a challenge. We communicated with nurse leaders through the organization’s clinical communications platform. Direct care nurses had to download an app on their personal phone to receive the daily affirmations because they don’t have access to the clinical communications platform.
We can address these obstacles in future interventions. For example, offering online positive thinking skills education would provide more flexibility for direct care nurses. To ensure the direct care nurses receive all communications, we would ask them to download the communication app when they sign up and send a test message to ensure successful connection between the participants and researchers. Future interventions also could include incorporating positive thinking skills at unit huddles and team meetings.
Recognize and adapt
An intervention successful with one group of nurses may not necessarily have the same results with another group. Recognizing barriers to success and adapting the intervention to individual groups with unique needs can help ensure beneficial outcomes.
The authors work at TriHealth in Cincinnati, Ohio. Amy Keller is a professional excellence specialist. Michele Huff is manager of nursing quality and VAT. Amanda Broyles is a charge nurse. Handada Atetih is a staff nurse. Brandon Ballhaus is vice president of operations. Rachel Baker is a nurse researcher.
American Nurse Journal. 2025; 20(5). Doi: 10.51256/ANJ052534
References
Achor S. The Happiness Advantage: The Seven Principles of Positive Psychology That Fuel Success and Performance at Work. New York: Broadway Books; 2010.
Bekhet AK, Zauszniewski JA. Measuring use of positive thinking skills: Psychometric testing of a new scale. West J Nurs Res. 2013;35:1074-93. doi:10.1177/0193945913482191
Comparcini D, Simonetti V, Totaro M, et al. Impact of traumatic stress on nurses’ work ability, job satisfaction, turnover and intention to leave: A cross-sectional study. J Adv Nurs. 2025. doi:10.1111/jan.16796
Gandhi V, Robison J. The ‘great resignation’ is really the ‘great discontent’. Gallup. July 22, 2021. gallup.com/workplace/351545/great-resignation-really-great-discontent.aspx
Keller A, Baker RB, Ballhaus B, Brehm S, Hanselman S, Huff M. Power of positivity. Am Nurse J. 2022;17(12). https://www.myamericannurse.com/power-of-positivity/ doi:10.51256/ANJ122224
Li N, Zhang L, Li X, Lu Q. The influence of operating room nurses’ job stress on burnout and organizational commitment: The moderating effect of over-commitment. J Adv Nurs. 2021;77(4):1772-82. doi:10.1111/jan.14725
Schoberer D, Bauer S, Schuettengruber G, Reiter L, Hoedl M. A secondary data study of frontline nurses’ and nursing managers’ assessed stress levels during the second COVID-19 wave. Nursing Forum. 2024;2024(1). doi:10.1155/2024/7012431
Key words: positive thinking, stress management, engagement


















