
Shorten delays, improve safety, reduce costs
- Hospital discharge delays can result in patient safety issues, reduced patient satisfaction, and increased costs.
- An assessment tool that goes into effect at admission can help the patient and healthcare team prepare for discharge.
Hospital discharge delay, defined as more than 2 hours from the time of a written order, can negatively impact patients and hospitals. In addition to patients experiencing some level of unhappiness or frustration, they also may face adverse clinical outcomes, such as falls or hospital-acquired infections. According to Bai and colleagues, the consequences for hospitals range from overcrowding in the emergency department (ED) to inappropriate use of high-cost hospital beds for care better provided in alternate settings. A study by Rojas-Garcia and colleagues found that between 8% and 10% of beds in an acute care hospital were occupied by patients whose discharge had been delayed. The causes behind delays must be addressed, and discharge discussions should begin at admission.
The problem
Many nurses are overwhelmed by a heavy workload that includes an increased number of patients with a high acuity level, so they might not be aware of the barriers resulting in discharge delays. On the 32-bed medical/surgical unit at our community hospital, the average discharge time (from the time the provider wrote the order to the time when the patient was physically discharged) was 5 hours and 6 minutes. The unit patient experience Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) discharge category score was 71.1 (national average 68.5).
Safe, effective, and timely discharge requires good communication among the healthcare team, the patient, and the family. According to a study by Meo and colleagues, effective healthcare team member communication during daily rounds can help reduce length of stay by 21%.
The solution
To help bedside nurses effectively communicate with patients, families, and providers in preparation for discharge, an interprofessional team at our organization developed a six-question discharge-planning assessment tool, which we piloted on the medical-surgical unit. We provided unit nurses with a written copy of the tool and explained its purpose—to expedite safe and effective hospital discharge. We instructed the nurses to use the tool as a prompt for discussing different aspects of discharge preparation during shift changes and at daily rounds with other healthcare team members. (See Ask the right questions.)
Ask the right questions
The discharge planning assessment tool includes the following questions to help staff expedite safe discharges.
- What is the anticipated discharge date of the patient?
- Where is the anticipated discharge destination?
- Is the family aware of discharge planning?
- Are their questions being answered?
- Do they have any concerns?
- Does the patient need any resources at home?
- Home health (PT, OT, RN, or aide)
- DME (oxygen, walker, beside commode)
- Does the patient have a central line or a urinary catheter?
- Is the patient going home with it?
- Confirm the patient’s pharmacy.
- Is the pharmacy open?
- Does the patient use meds by mail?
DME = durable medical equipment, OT = occupational therapy, PT = physical therapy
Between November 1, 2020, to May 31, 2021, 1,788 patients were discharged from the unit (1,552 discharged home and 236 discharged to a facility). The pre-data collection period began on November 1; the next 6 months included the implementation and post-implementation phases of the pilot.
Question 1: Discharge date
The discharge planning assessment tool begins with the question, “What is the anticipated discharge date of the patient?” Using information about a patient’s diagnosis, lab values, test results, and admission status before transfer from the ED and admission to the unit, nurses can anticipate an approximate discharge date and discuss it with the patient and family when they arrive on the unit. The patient and family can continue that discussion with the provider and then make necessary arrangements with their place of employment and other family members or friends who may offer assistance.
Question 2: Discharge destination
The nurse asks, “Where is the anticipated discharge destination?” Assuming a patient’s discharge location acts as a significant cause for delay. For example, some patients may live alone or have no family in the area so they won’t be able to care for themselves. Others may be unhoused and living on the streets. Asking this simple question at admission can help start the discharge process before it even begins.
Question 3: Family concerns
Asking, “Is the family aware of discharge planning? Are their questions being answered? Do they have any concerns?” acknowledges the caregivers’ role in the discharge process, including managing vital tasks, such as transportation and treatment options. Nurses may think that all questions were answered at admission, but family members can’t be expected to retain all the information relayed on a stressful day. Nurses and other members of the healthcare team must continue to address families’ questions and concerns throughout the patient’s hospital stay. They can help guide family members and reduce their anxiety by offering compassion and engaging with them about their loved one’s diagnosis and treatment plan.
Question 4: Patient needs
The need for resources creates another barrier to discharge, so the nurse should ask, “Does the patient need any resources at home? Do they need home health, physical therapy, or a nurse aide? Do they need any medical equipment, such as oxygen, a walker, or a bedside commode?” Waiting to coordinate resources or medical equipment delivery can delay discharge from a couple of hours to an entire day. In some cases, an insurance company won’t cover all of the resources, so the family will need time to research options so they can make informed decisions.
Question 5: Invasive lines
Invasive lines can create another barrier to timely discharge, so nurses should ask, “Does the patient have a central line or a urinary catheter? Are they going home with it?” For a patient with an invasive line, the healthcare team should begin addressing it the day or night before the anticipated discharge. Central lines require a provider order to continue or discontinue access as well as the necessary dose of heparin to maintain patency after discharge. A urinary catheter also will require a provider order for continuation or removal. If the provider orders removal, the patient must void within 4 to 6 hours before discharge, which creates the potential for delays. If the patient can’t void within that timeframe, the provider may order reinsertion of the catheter. Addressing these issues during the shifts prior to discharge can help prevent a delay.
Question 6: Medications
To avoid delays related to discharge medications, the healthcare team should ask, “Which pharmacy does the patient prefer, and do they receive meds by mail?” Many hospitals send new discharge medications electronically to the patient’s preferred pharmacy rather than writing a paper prescription, but what if a patient is discharged over a weekend, on a holiday, or after hours when the pharmacy isn’t open? Medications delivered by mail can reduce costs and provide convenience, but this delivery option won’t accommodate patients who need to start medications immediately. Asking the provider for a written prescription before discharge, providing the patient with a list of 24-hour pharmacies in the area that can fill their medications, and sharing information about medications with discounted price coupons can help expedite the patient’s discharge and improve their overall experience.
Believing in the process
Using this tool in combination with collaboration among healthcare team members during daily rounds improved the discharge time on this pilot unit by 57 minutes. In addition, patient experience scores on the HCAHPS discharge process questions improved by 16.4 points. (See Steady improvement.)
The change and improvement didn’t happen quickly. It required continuing education and reinforcement with the staff. Slowly, the times from the discharge order to actual discharge decreased, and patient experience scores improved. As the results came in every month, the staff began believing in the process, and it became a natural part of their bedside care.
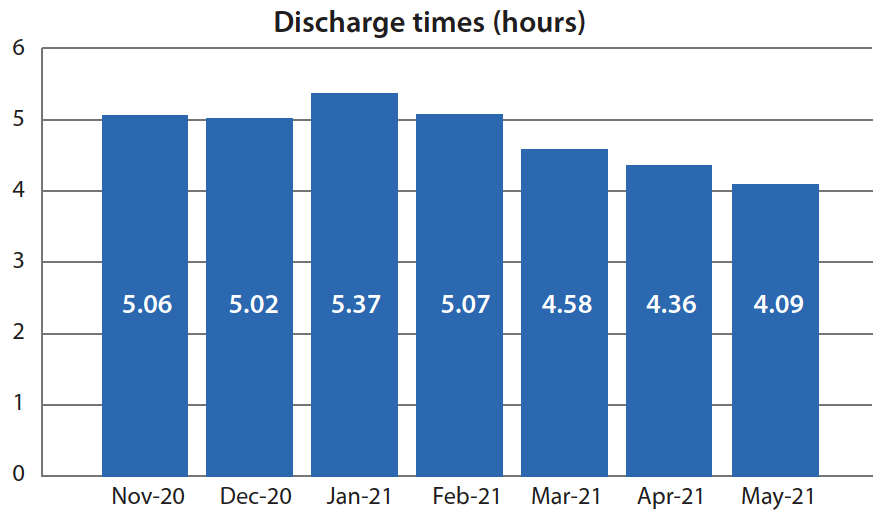
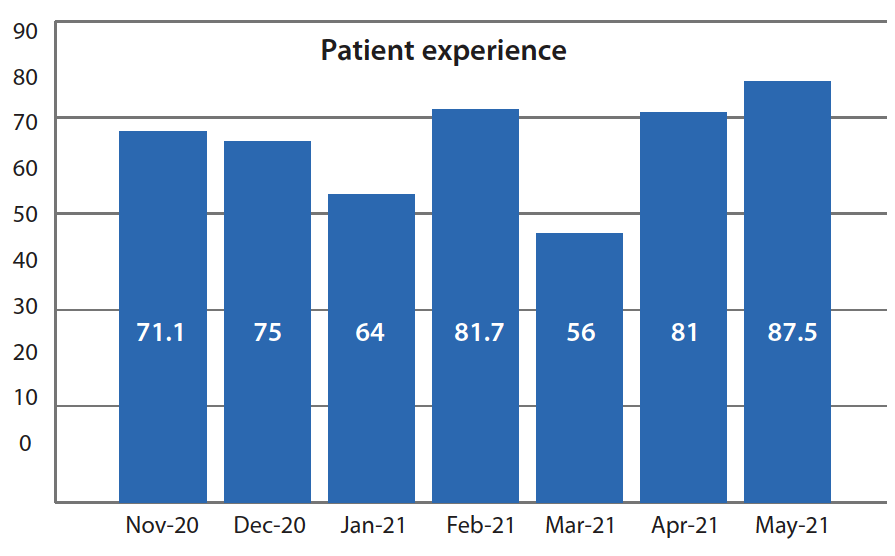
Steady improvement
Both discharge times and patient satisfaction scores improved during the discharge planning assessment tool pilot project.
A noticeable decrease in discharge times occurred from November 1, 2020, to May 31, 2021.
During the same period, we also observed a noticeable improvement in patient experience HCAHPS scores. (In March 2021, a decline occurred during a high vacation time when float pool nurses covered the unit.) Patients answer three questions about discharge as part of HCAHPS:
- When I left the hospital, I had a good understanding of things I was responsible for in managing my health.
- When I left the hospital, I clearly understood the purpose for taking each of my medications.
- Did you get information in writing about symp or health problems to look out for after you left the hospital?
The authors work at Houston Methodist West Hospital in Houston, Texas. Heather Stein is an operations administrator, Keshia S. Duhon is a case manager, and Jose Sepulveda is a social worker.
American Nurse Journal. 2023; 18(6). Doi: 10.51256/ANJ062314
References
Bai AD, Dai C, Srivastava S, Smith CA, Gill SS. Risk factors, costs and complications of delayed hospital discharge from internal medicine wards at a Canadian academic medical centre: Retrospective cohort study. BMC Health Serv Res. 2019;19(1):935. doi:10.1186/s12913-019-4760-3
Centers for Medicare and Medicaid Services. HCAHPS: Patients’ perspectives of care survey. December 1, 2021. cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/HospitalHCAHPS
Family Caregiver Alliance. Hospital discharge planning: A guide for families and caregivers. caregiver.org/resource/hospital-discharge-planning-guide-families-and-caregivers
Ibrahim H, Harhara T, Athar S, Nair SC, Kamour AM. Multi-disciplinary discharge coordination team to overcome discharge barriers and address the risk of delayed discharges. Risk Manag Healthc Policy. 2022;15:141-9. doi:10.2147/RMHP.S347693
Meo N, Bann M, Sanchez M, Reddy A, Cornia PB. Getting unstuck: Challenges and opportunities in caring for patients experiencing prolonged hospitalization while stable for discharge. Am J Med. 2020;133(12):1406-10. doi:10:1016/j.amjmed.2020.05.024
Rojas-Garcia A, Turner S, Pizzo E, Hudson E, Thomas J, Raine R. Impact and experiences of delayed discharge: A mixed-studies systematic review. Health Expect. 2018; 21(1):41-56. doi:10:1111/hex.12619
Key words: discharge planning, assessment tool, cost reduction, discharge delays, patient safety


















