
A dedicated discharge unit decreases length of stay and improves ED treat and admit times.
Takeaways:
- Implementing a discharge unit in an acute care hospital can improve patient throughput in emergency departments (EDs) and inpatient units.
- Improving patient throughput allows ED patients to be initially examined and subsequently admitted sooner to the inpatient unit.
Holding patients with admission orders in the emergency department (ED) is a global problem that results in overcrowding, which is linked to poor patient outcomes and poor efficiency metrics. Specifically, holding patients in the ED is associated with decreased patient satisfaction and increased left-without-being-seen rates, hospital length of stay (LOS), and mortality.
Inpatient bed availability determines how quickly a patient in the ED can be transitioned to the admitting inpatient unit. For a variety of reasons (for example, lack of transportation), hours may pass from the time a physician enters discharge orders to when a patient actually leaves the room, decreasing patient throughput and delaying patient admission from the ED. Timely inpatient bed availability is essential to efficient patient throughput in acute-care hospitals.
Evidence-based intervention
Hospital throughput quality-improvement projects typically target patients being discharged to home because they make up the highest percentage of discharged patients and provide the greatest opportunity to improve patient flow. One such evidence-based intervention is the discharge unit.
Since the 1990s, discharge units have been used as an intervention to expedite inpatient bed availability, which has been shown to reduce ED holding times. Studies indicate that discharge units can improve customer satisfaction, decrease ED boarding times, increase patient throughput efficiency, and reduce hospital LOS and discharge errors.
In 2018, the treat and admit times (defined as the time a patient registers in the ED to the time they’re admitted to the inpatient unit) at Sentara Obici Hospital were consistently more than 400 minutes compared to a goal of 240 minutes. In an effort to reduce this time, a discharge unit proposal was presented and approved by hospital administration. To evaluate the efficacy of the unit after implementation, we conducted a quality-improvement project to assess if treat and admit times and inpatient LOS were reduced.
Discharge unit how-to
Sentara Obici Hospital is a Magnet®-recognized, 175-bed hospital in rural Virginia. To develop and implement the discharge unit, we had to be creative when stretching already limited resources. We faced two main challenges: selecting the location for the unit and staffing it.
Location
With hospital administration support and facilities management personnel assistance, we secured an unoccupied human resources office at the front of the hospital as our original discharge unit location; a new outpatient pharmacy required that we relocate to our current location (two vacant inpatient rooms). Facilities management personnel helped us turn the rooms—one for patients who can sit upright and one for those who need a hospital bed to be discharged by stretcher—into a functioning discharge unit for staff and patients.
Staffing
Discharge unit staffing is based on our specific hospital needs. The daily census for our discharge unit was 10 to 15 patients. Our goal was to staff it with one RN and one nursing assistant (NA) per shift. To meet that goal, we enlisted RNs and NAs who wanted extra hours and those who are employed by the hospital’s resource pool.
Patient eligibility
Patient eligibility for discharge via the new unit is based on the following criteria:
- discharge order to home or a skilled nursing facility
- all conditions met for discharge
- planned transportation available
- no form of isolation
- no high-acuity patient care needs.
Obstetric and mental health patients are automatically excluded from the discharge unit. Daily forms were created for screening and logging patients.
After a patient arrives to the unit, the discharge nurse makes follow-up appointments, administers medications, and provides meals, nursing care, and high-quality discharge instructions.
Training and implementation
Clinical nursing staff were educated on the discharge unit and patient eligibility criteria via email communication, printed flyers, and just-in-time education. During the first few months of implementation, the discharge unit nurse educated eligible patients’ primary nurses on the unit’s processes and care. Nurse buy-in was difficult in the first few months; many nurses were wary of handing over the discharge process to another nurse. However, after they realized the decrease in their workload by sending patients to the discharge unit and observed positive patient outcomes, the unit became standard care.
Implications
The discharge unit has helped Sentara Obici Hospital reduce treat and admit times and improve patient throughput efficiency. Sending eligible patients to the discharge unit has resulted in freeing up inpatient beds more quickly, and anecdotally observed decreased workloads have gained more nurse buy-in. (See Head-to-head comparison.)
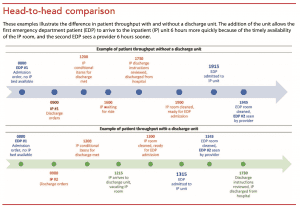
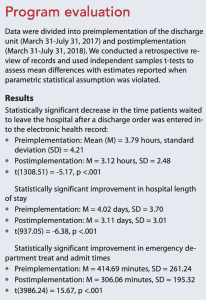
Our program evaluation indicates that the discharge unit contributed to lowering ED treat and admit times by 109 minutes on average. This likely resulted in patients receiving timely care on the admitting unit. The discharge unit also was effective in reducing the time from discharge order placement to physical discharge by 40 minutes on average. This significantly lower LOS (almost 1 day shorter on average) can be partially attributed to more timely discharge. (See Program evaluation.)
 One qualitative benefit of the discharge unit is that patients receive more personalized discharge instructions with fewer interruptions. When patients have the discharge nurse’s full attention, they have an opportunity to ask questions and receive clarification.
One qualitative benefit of the discharge unit is that patients receive more personalized discharge instructions with fewer interruptions. When patients have the discharge nurse’s full attention, they have an opportunity to ask questions and receive clarification.
Next steps for our team are to continue to evaluate the impact of the discharge unit on treat and admit times, discharge order times, and LOS. For other facilities considering implementing a discharge unit, different development and staffing formats may be needed based on discharge census and other site-specific constraints. Collaborating with other hospital departments was critical to the development of our unit and will remain vital for its continued success.
Brittney W. Curle is an adult-gerontology clinical nurse specialist at Sentara Obici Hospital in Suffolk, Virginia. Ralitsa Maduro is a biostatistician at Sentara Healthcare Quality Research Institute in Virginia Beach, Virginia.
References
Di Somma S, Paladino L, Vaughan L, Lalle I, Magrini L, Magnanti M. Overcrowding in emergency department: An international issue. Intern Emerg Med. 2015;10(2):171-5.
El-Eid GR, Kaddoum R, Tamim H, Hitti EA. Improving hospital discharge time: A successful implementation of Six Sigma methodology. Medicine. 2015;94(12):e633.
Franklin BJ, Vakili S, Huckman RS, et al. The inpatient discharge lounge as a potential mechanism to mitigate emergency department boarding and crowding. Ann Emerg Med. 2020;75(6):704-14.
Hernandez N, Dinesh J, Mitchell J. A reimagined discharge lounge as a way to an efficient discharge process. BMJ Qual Improv Rep. 2014;3(1):u204930.w2080.
Vermeulen MJ, Guttmann A, Stukel TA, et al. Are reductions in emergency department length of stay associated with improvements in quality of care? A difference-in-differences analysis. BMJ Qual Saf. 2016;25:489-98.
Yarmohammadian MH, Rezaei F, Haghshenas A, Tavakoli N. Overcrowding in emergency departments: A review of strategies to decrease future challenges. J Res Med Sci. 2017;22:23.

















