Use technology to support bedside nurses, increase care access, and expand education.
The big experiment of providing services via virtual platforms, necessitated by the pandemic, resulted in positive and negative outcomes. Overall, we’ve learned that patients value a personal presence, but when offered a virtual process (a simulated healthcare encounter facilitated by technology), patients frequently found it a satisfactory alternative to in-person encounters.
Organizations predominately use telehealth (delivery of healthcare, health education, and health information services via remote technology) to improve access, provide care management, and offer education to providers and patients. As we navigate and innovate through future pandemics and other challenges, we’ll need to expand the current concepts of telehealth to develop new ways of working with and for patients.
Virtual processes in practice
As we adjust our lens to see a healthcare world with fewer people resources, we can envision virtual processes to support nursing activities that don’t necessarily require a personal presence. Across the country our colleagues are putting the idea to the test.
In May 2020, using iPads and a virtual command center, Houston Methodist Hospital initiated video-enabled physician rounds for patients with COVID-19 to minimize personal protective equipment use and staff exposure. The hospital has deep experience with remote real-time technology through the development of its Virtual ICU (vICU). This 24-hour operation center, staffed by critical care nurses and intensivists, monitors real-time physiologic data with predictive analytic tools to identify patients at risk for decompensation. Staff can see and hear what’s happening in the patient rooms, which are remotely located in the emergency department.
St. Luke’s Health System of Kansas City established a virtual inpatient unit based on the premise that many nursing tasks are repetitive, which creates inefficiency. The support of a centralized staff to monitor and perform data entry allows the bedside team to provide essential patient care.
In 2014, Catholic Health Initiatives trademarked its Virtually Integrated Care (VIC) model, which uses a remote primary nurse for a group of inpatients to maintain continuity for patients and provide support, education, and guidance to the bedside care team. This remote nurse’s responsibilities include patient monitoring, care coordination, physician collaboration, admission, and discharge activities.
Virtual opportunities
These programs, and others, serve as examples of the virtual possibilities for your team and organization. Case management and discharge planning, for example, could be converted to a fully telehealth model using video conferencing and revised workflows or a hybrid of telehealth and in-person processes. The bedside team or a rounding case manager conducts and documents the patient’s psychosocial status in the electronic health record (EHR). The remote case management and discharge planning team performs the assessment, documents the plan, and initiates the steps outlined in the discharge plan. The EHR serves as the source for the action plan, findings, next steps, conclusions, and directions. The bedside team is fully informed through EHR documentation and prepared to support a safe, timely discharge with complete instructions for the patient and caregivers. If case management and discharge rounds are necessary, they’re accomplished via a regularly scheduled online video conference.
Care team consultation also presents an opportunity for a virtual platform. For example, a palliative care consult involving the hospitalist, oncologist, pharmacist, and hospice personnel can be effectively and efficiently conducted via video conferencing. Consultants from each discipline make their rounds, document assessments, and outline the proposed plan. They then hold online video office hours at prescribed times for the nursing unit. Each nurse is guaranteed a scheduled virtual face-to-face discussion about their patients and proposed care plans.
Medication reconciliation, an essential and time-consuming activity, requires uninterrupted focus. With an up-to-date medication administration record, a pharmacy technician with demonstrated proficiency in medication reconciliation can review medications and thoroughly document them in the EHR. The technician outlines the details of the differences between prehospitalization and hospital-prescribed medications, accounting for the variations through documented communication with the prescribing physician.
Making the transition
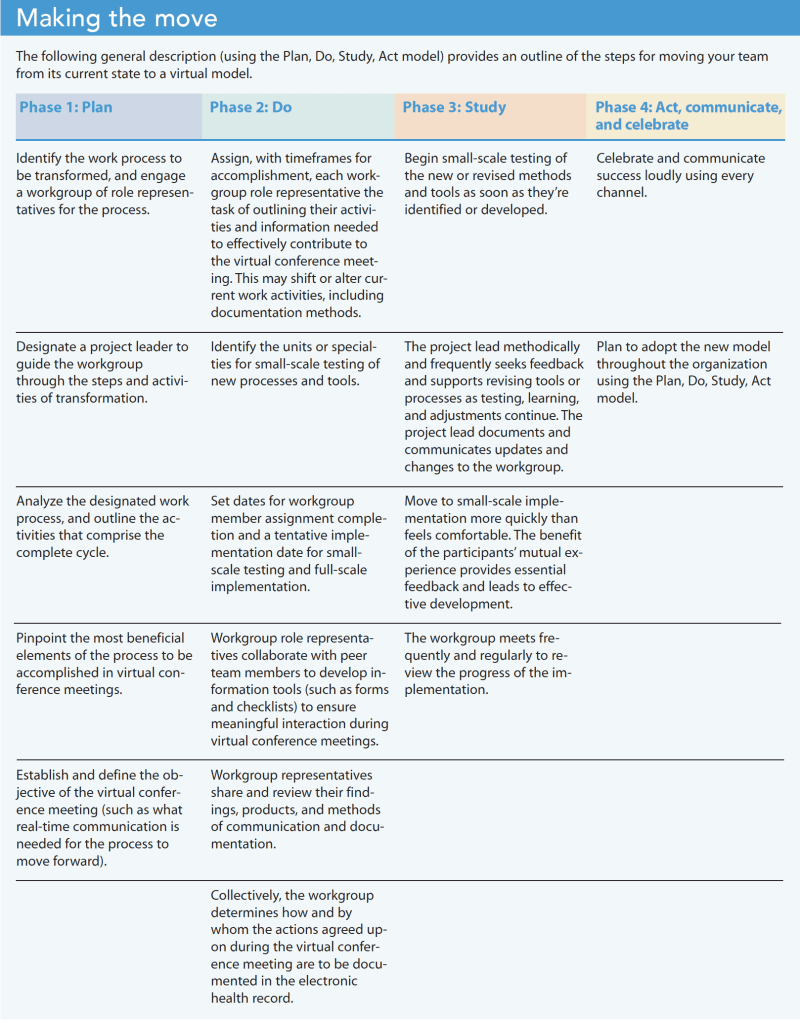
Transitioning to a virtual model for a team function makes optimal use of expert human resources, enhances team members’ technology skillsets, and increases organizational intelligence via the smart use of technology. However, making this transition presents challenges. It requires planning, practice, patience, and the development and acceptance of new tools. Following the Plan, Do, Study, Act (PDSA) method can help your team move from its current state to a new virtual model. (See Making the move.)
Best practices
As your team works through the PDSA phases, incorporating best practices will ensure a smooth transition and reduce resistance.
Central information location:
Establish an easy-to-access online intranet page that serves as a central location for information and a meetings calendar. Include meeting times with URL links, an up-to-date agenda with expected participants, and the order of presentations.
Virtual conference meeting administrator:
Designate one person responsible for maintaining the central calendar, outlining the agenda, and being notified by participants of their expected presence or replacement. The administrator facilitates the meeting by taking participant attendance, reviewing the agenda, and focusing the discussion in accordance with the timetable. The virtual conference meeting administrator serves as the main point of contact for participants who have questions about the agenda, discussion items, and connectivity.
Individual participant responsibility:
Individual participants must complete their assigned prework and attend the virtual meeting, signing-in 5 minutes before the start time to ensure connectivity. They also should review the agenda, understand their meeting responsibilities, and participate accordingly.
Patient privacy:
Maintain protected health information (PHI) safeguards and ensure each participant understands and adheres to the organization’s regulations about patient information when communicating outside of the EHR. Participants should plan ahead for a meeting location that provides privacy, minimal noise, and limited interruptions.
Substitute and new participants:
Before a new or substitute participant is introduced to the team, the current role participant and preceptor should review virtual conference meeting responsibilities and practice using the platform.
Time management:
Virtual conference meetings have the advantage of advance scheduling and a predictable format. Structuring time allocations for participant discussion of essential topics allows everyone to plan their time and helps maintain meeting focus.
Education opportunities
Many aspects of nursing education and orientation already use virtual experiences, including PowerPoint presentations, videos, and animated lessons. The challenge stems from ensuring learners understand the organization’s mission and standards for safe practice within professional ethical guidelines and policies using these techniques.
Online learning:
Practical online vignettes (using text, animation, or video) should engage participants to recognize and acknowledge their understanding of the concepts and allow for deep learning. Guided discussions through virtual conference meetings with a staff development team member provides learners with an opportunity to review the vignettes and their selection of actions to reinforce best practices.
Mentoring:
Mentors can work with nurses virtually, making it possible for experienced nurses in specialty roles throughout the organization to serve in this role. Because all nurses share the same nursing process, a nurse mentor, regardless of specialty, can relate to new-to-the-organization and new-to-nursing nurses. Contracts that outline the mentor/mentee relationship include objectives and expectations of both participants. A mentor can hold virtual conference meetings at mutually agreed-upon times, as frequently as needed, and at the mentee’s request. Both participants benefit from accessible online information that outlines expectations, required collaboration, and the timeframe for accomplishing activities that demonstrate progress toward objectives.
Precepting:
Using shadowing, observation, and demonstration, nursing preceptors impart the healthcare setting’s nursing process expectations. Preceptors serve as role models and guides to best practices. Precepting goals include learning to use available resources to ensure nursing care safety, efficiency, and effectiveness. The preceptor uses a checklist that enumerates the essential topics and activities in which the preceptee must demonstrate competency. This mastery learning or competency-based education approach requires a tight structure with the following five elements for each item:
- Specific, clear, demonstrable learning objectives
- Specific definitions of what competency looks like or means
- Process for demonstrating competency
- Process for assessing competency
- Documentation outlining the preceptee’s progress toward competency. (What is the preceptee competent to do now? What remains to be learned?)
The preceptor can share online a clearly written preceptor checklist that includes the five elements per item and doesn’t depend on a face-to-face relationship. In pre- and post-shift virtual conferences, the preceptor and preceptee can review the day’s activities and experiences for clarification and reflection. In addition, competency for some of the checklist items can be accomplished using simulation or a video conference. Many opportunities for introducing virtual experiences into the current healthcare nursing process exist, but in-person precepting may be lower on the priority list as a candidate for transitioning to a virtual experience.
Worth the effort
Obstacles to adopting any virtual model include participants who resist the change because they’re unfamiliar or uncomfortable with technology and workgroup members who value and enjoy social in-person interactions. Many believe that virtual meetings involve doing everything the same way as an in-person meeting. Although the workload is the same, the timeliness of activities and clarity of documentation are essential for productive virtual meetings.
We’re being challenged to adapt to the reality of our circumstances, now and for the future. Using the power of technology, we can optimize the benefits of collaboration among expert resources. The adoption of virtual conferencing and other practices that loosen time constraints and open the door to flexibility offers important benefits. For example, bedside care teams can focus on the immediate needs of their patients, with fewer interruptions, knowing that the physiologic status of all of their patients is being monitored and administrative activities of multidisciplinary care communications are managed. Those with consultation roles, such as hospitalists, pharmacists, and palliative care staff, can manage their time while meeting role responsibilities. In addition, expert nurses in specialties, critical care, care coordination, and discharge planning can leverage their knowledge and skills across the organization.
When we accept this challenge, we practice the essentials of change management, enhance our knowledge of clinical collaboration processes, and expand the boundaries of technology in our organization. And, most importantly, our patients will receive essential services in a timely manner. The outcome will be worth the effort.
Rebecca Falanga is a healthcare consultant and principal at RJF Enterprises, Inc in Clearwater, Florida.