
Reducing falls on an acute geriatric medical–surgical unit
- A quality improvement project aimed to reduce falls by focusing on evidence-based delirium prevention strategies.
- The ESCAPE bundle includes Early mobilization, Sunlight and Sleep, Constant reorientation, avoiding Stimulants, Pain control, and Effective communication.
- Implementing an evidence-based delirium prevention bundle can reduce fall incidence rates, decrease the need for patient companion hours, and significantly improve patient safety and satisfaction scores.
Learning Objectives
- Distinguish between delirium and dementia in hospitalized geriatric patients.
- Identify common medical and pharmacological triggers of delirium.
- Describe the components, implementation, and impact of the ESCAPE bundle on fall reduction.
No relevant financial relationships were identified for any individuals with the ability to control content of the activity.
Expiration: 9/1/28
Falls in hospitals frequently coincide with delirium, a common yet sometimes unrecognized comorbidity among geriatric patients. Delirium is characterized by sudden, rapid cognitive impairment (distinct from the gradual onset of disorders like dementia) and fluctuating levels of attention and awareness. It also may present with psychomotor changes ranging from hypoactivity to hyperactivity, disrupted sleep patterns, and varied emotional disturbance. Some patients experience cognitive and functional effects for up to a year after discharge.
When up is down: Delirium superimposed on dementia
Seven reversible causes of dementia in older adults
Delirium can result from a medical condition or other trigger, such as infections, medication side effects, metabolic imbalances, or neurologic disorders. Effectively managing delirium and preventing further complications require identifying and addressing the underlying medical cause.
To address the need to prevent delirium and reduce falls, we implemented a quality improvement (QI) project on a medical–surgical unit dedicated to acute-care geriatric patients.
Evidence review
We began by reviewing evidence related to falls and delirium. In the United States, according to the Centers for Disease Control and Prevention, falls significantly impact the health of adults over 65, with 37% incurring injuries that add roughly $750 million in healthcare costs annually. The persistence of falls, despite various prevention strategies, indicates an urgent need for effective programs that enhance patient outcomes and optimize hospital costs.
According to Ueda and colleagues, delirium affects 18% to 35% of patients in adult geriatric medical units, underlining the need for healthcare professionals well-versed in its causes, management, and preventive measures. A study by Kalivas and colleagues found that 37.6% of patients who fell had positive delirium screenings, directly associating the occurrence of delirium with an increased risk of falls. Feinkohl and colleagues delved into the complex origins of delirium, including medication side effects, metabolic issues, and infections as potential triggers, suggesting a multi-faceted approach to prevention. (See Delirium contributors.)
Delirium contributors
The following can contribute to delirium in hospitalized patients:
Infections
Systemic infections, particularly urinary tract infections and pneumonia, have been associated with delirium in hospitalized patients. These infections can lead to inflammatory responses that impact the central nervous system and trigger delirium. If staff suspects this, the provider will order urine and blood testing.
Hypoglycemia
Low blood sugar levels can result in neurological symptoms, including confusion, dizziness, and, in severe cases, delirium. Regular monitoring and timely intervention by nursing staff can prevent hypoglycemic episodes and their adverse effects.
Metabolic syndromes
Electrolyte imbalance, thyroid dysfunction, and renal or hepatic insufficiency can disrupt brain functions, making these factors critical to monitor and manage. Nursing staff also should monitor the patient’s hydration status.
Medications
Researchers, such as Chyou and colleagues and Rossi Varallo and colleagues, have found several medications that either induce or exacerbate delirium, including anticholinergics, sedative-hypnotics, corticosteroids, and some antihistamines. In instances where providers prescribe medications known to influence delirium, nurses should proactively voice their concerns to the prescribing provider or raise them during team huddles, fostering a collaborative approach to patient care.
The significant correlation between delirium and falls emphasizes the need for an evidence-based prevention bundle and early identification of high-risk patients to enhance patient safety, improve care quality, and achieve economic savings.
Theoretical framework
Our QI project leveraged the Knowledge-to-Action (KTA) framework, as described by Ham-Baloyi, to translate delirium research into clinical practice. This framework operates in two main phases: knowledge creation and action.
In this project, the knowledge creation phase involved gathering and adapting evidence on delirium prevention, identification, and management to fit the project’s local context. Development of the ESCAPE (Early ambulation, Sunlight and sleep, Constant reorientation, Avoid stimulants, Pain control, and Effective communication) prevention bundle evolved out of the knowledge creation phase of the KTA framework.* Research has found each intervention to aid mitigation of the risks associated with delirium.
In the action phase, we undertook strategic implementation of the ESCAPE bundle. We identified local barriers and facilitators, engaged stakeholders (RNs, patients, families, and physicians), and tailored the approach to the local healthcare setting while adhering to the bundle’s core principles.
Project aims and methods
This project aimed to reduce the number of falls among hospitalized patients by focusing on delirium prevention using the ESCAPE prevention bundle, implementing the Confusion Assessment Method (CAM) score for delirium as a screening tool, and providing education to clinical staff. The CAM score provides a validated method for assessing acute symptom onset, inattention, disorganized thinking, and altered consciousness.
The revised Standards for Quality Improvement Reporting Excellence underpinned the project’s methodology. Conducted on a 30-bed acute geriatric medical–surgical unit at a community hospital in Westchester County, New York, the project targeted a diverse patient demographic (predominantly geriatric).
Intervention
Nursing staff across all units received pre-intervention training on the ESCAPE bundle components, the CAM score, and delirium recognition. In-person education included presentations on delirium, which covered its signs, symptoms, various types, and causes. Approximately 90% of the staff, including nursing assistants and patient care technicians, have completed the training. We also reviewed the material with providers to enhance discussions during medical rounds.
Addressing the link between delirium and increased fall risk, the project emphasized educating nursing and support staff on delirium’s nature and its hypoactive, hyperactive, and mixed presentations. This comprehensive education aimed to equip staff with the knowledge necessary for effective delirium management and prevention.
The project underwent internal ethical review to ensure the safety and well-being of all participants. Senior nursing leadership and nursing quality team members provided verbal ethical approval, which we documented in internal meeting minutes. We maintained patient confidentiality throughout the project, and mitigated all potential conflicts of interest, especially financial ones.
ESCAPE bundle
We introduced the ESCAPE prevention bundle after foundational training on delirium. This evidence-based, holistic approach to delirium prevention synergizes the following six core components:
Early ambulation. Studies, including by Anada and colleagues, have shown that early mobility decreases delirium and that it’s safe and feasible. As appropriate, staff moved patients out of bed to sit in a chair (including for meals) or provided assistance with walking as needed and appropriate. We removed commodes from the bedside to encourage ambulation to the bathroom with assistance. Clinical nurses, physicians, nursing assistants, physical therapists, and occupational therapists performed early mobility tasks.
Sunlight and sleep. As noted by Lee and colleagues, exposure to natural sunlight aids circadian rhythm regulation, which promotes better sleep and potentially reduces the onset and persistence of delirium. Proper and high-quality sleep supports cognitive function. Nursing staff opened window blinds in the morning and moved the patient to a chair if tolerated. Night shift nursing staff minimized noise and interruption (including curtailing vital signs and certain medications) to promote adequate sleep, especially between 11 pm and 5 am.
Constant reorientation. Reorientation can help reduce confusion and disorientation by connecting the patient to reality. It involves continually reminding patients of their location, time, and recent events. To aid reorientation, staff implemented environmental modifications (such as updating whiteboards, providing clocks, and permitting familiar items from home), assisted with calls to family members, and ensured patients had glasses or hearing aids. In the event of a distressed patient, staff limited the number of individuals in the room.
Avoid stimulants. Certain medications stimulate the onset and exacerbation of delirium, especially in vulnerable patient populations. Nurses reviewed patients’ medication lists during each shift and proactively communicated concerns about potentially deliriogenic medications (anticholinergics, benzodiazepines, and opioids) to prescribing providers and raised these concerns during interdisciplinary team huddles. They also monitored patients closely for early signs of medication-related confusion or agitation and implemented nonpharmacologic comfort measures (repositioning, reassurance, environmental modifications) before requesting additional medications that could contribute to delirium.
Pain control. Pain can lead to sleep disturbances, anxiety, agitation, and physiologic stress, all of which can contribute to delirium. However, some pain medications, such as opioids, also can cause delirium in susceptible and high-risk patients. Nurses screened patients for pain at every shift. For patients receiving pain medication, nurses performed hourly reassessments.
Effective communication. Clear, empathetic, and emotional communication can help alleviate patients’ fear and anxiety, which can reduce the severity of delirium episodes. Effective communication involves reassurance, active listening, and validating the patient’s feelings.
After implementing the ESCAPE bundle, we provided additional education to reinforce its critical role in improving patient outcomes.
Audit process
To monitor the intervention’s effectiveness, we established an audit process. Each month, we reviewed nursing documentation, including neurological and pain assessments, patient status changes, and delirium CAM scores. The audits showed a correlation between improved documentation of interventions (including CAM scores and the ESCAPE bundle) and decreased falls. For example, only patients identified with delirium using the CAM score were targeted for intervention, which ensured focused and timely management for those at risk.
To systematically assess the impact of the intervention on patient outcomes, especially concerning the incidence of delirium and falls, we adopted a multifaceted approach. We used quantitative (chart audits, fall rates) and qualitative (feedback) methods to provide a holistic understanding of the project’s effectiveness.
Random monthly chart audits. We reviewed the quality and consistency of nursing documentation, including targeted documentation on the CAM score, pain evaluation, neurological assessments, and mental status changes.
Documentation correlation with fall rates. We established monthly trends and compared the frequency and quality of documentation with the incidence of falls.
Evaluation of medication adjustments. Given the ESCAPE bundle’s emphasis on avoiding stimulants, we closely monitored any medication adjustments, especially those known to exacerbate delirium. This evaluation included tracking instances where nurses advocated for medication changes and the subsequent decisions taken during medical team huddles.
Feedback mechanism. After each audit, nursing staff received feedback regarding areas of strength and those needing improvement.
Process and outcome measures
The project examined how enhanced nursing documentation and the implementation of the ESCAPE bundle, documented through the CAM score, impacted fall rates. Discussion during interdisciplinary huddles, as well as regular feedback sessions with providers and nursing teams, played a critical role in evaluating the intervention’s success.
We ensured data integrity by cross-verifying information with electronic health records and conducting patient chart audits, with discrepancies flagged for review. The project monitored the ESCAPE bundle’s monthly utilization rates by assessing the frequency of nursing documentation on the CAM score.
The primary outcome measure was fall incidence, with pre-intervention data collected from October to December 2022, and the intervention phase measured from February to April 2023. We assessed post-intervention fall rates from May to July 2023. Secondary outcomes, potentially directly influenced by ESCAPE bundle use, included total companion hours and Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores, providing a comprehensive view of the project’s impact on patient care and satisfaction.
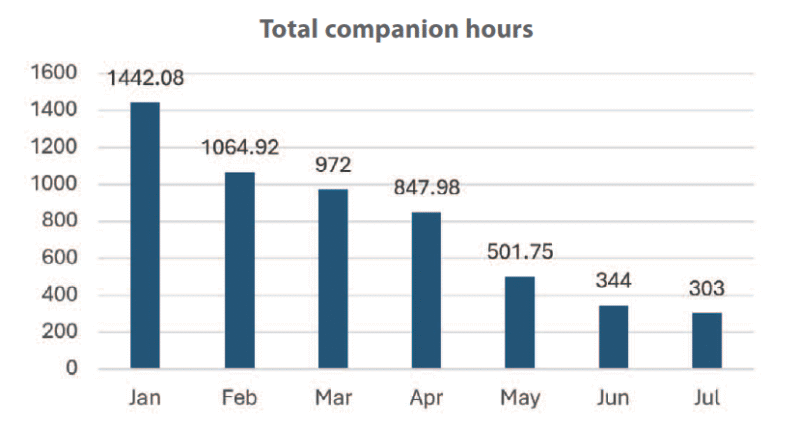
Companion hours. This secondary outcome gauged the overtime hours allocated for 1:1 sitters for confused or at-risk patients. We observed a directly proportional decrease in these hours (from 1,422 hours to 847.98 in April) in conjunction with ESCAPE bundle use, indicating improved patient care outcomes and potentially reduced confusion and agitation. We didn’t collect companion hour data between October and December because this wasn’t one of the project’s primary aims.
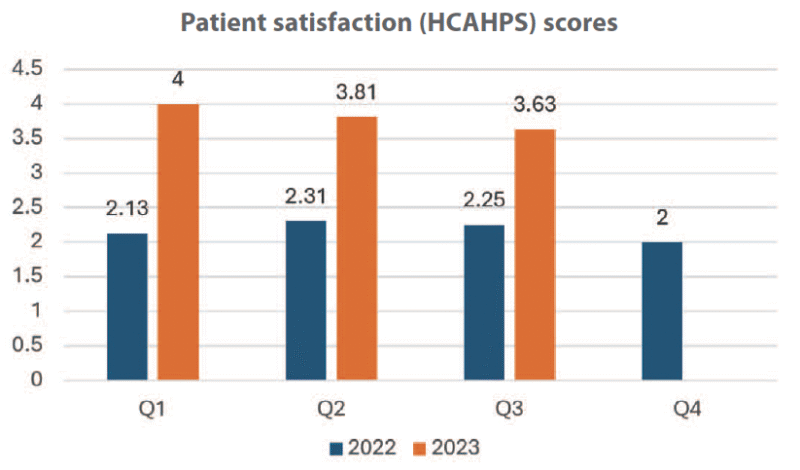
HCAHPS score. The HCAHPS score offers insights into patients’ perceptions of their hospital experiences. HCAHPS scores are expressed in star ratings (from 0 to 5). From the fourth quarter of 2022 to the first quarter of 2023, the unit’s patient satisfaction score rose from 1 to 4 stars. During the post-intervention phase, the unit maintained a 3.5-star rating in the second quarter of 2023. (See Secondary outcomes.)
Secondary outcomes
In addition to delirium prevention and falls reduction, this quality improvement project resulted in positive outcomes related to patient satisfaction and costs.
HCAHPS score
The quarterly Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores indicated an overall improvement in patient satisfaction during the intervention, potentially because of the enhanced care stemming from application of the ESCAPE bundle.
Companion hours
The project resulted in a 79% reduction in companion hours from a peak of 1,442.08 in January 2023 to 303 in July 2023. This finding points to the ESCAPE bundle’s effectiveness at managing patient agitation or confusion, reducing the need for 1:1 sitters.
Data analysis
We used a mixed-methods approach, encompassing qualitative interviews and quantitative data. Patient feedback, nursing notes, and medical observations provided qualitative insights, while fall rates and delirium occurrences were statistically analyzed. We collected cumulative data from the unit on the first day of each month.
Results
The project’s pre-intervention phase occurred from October to January 2023, with staff education provided in January 2023. The intervention phase ran from February to April 2023, beginning with staff training on the ESCAPE bundle and then integration into daily routines.
Fall incidence rates decreased as ESCAPE bundle use and documentation of relevant categories (such as pain, neurological assessment, change in status, and CAM scores) increased. From January to December 2022, the unit’s fall incidence rate peaked at 22. In the last quarter of 2022 and January 2023, the unit experienced seven falls. We included January 2023 because that month focused on education before intervention implementation; one fall occurred in January. From February to July 2023, the unit experienced only three falls—two during the implementation phase (February to April) and one post-intervention (July).
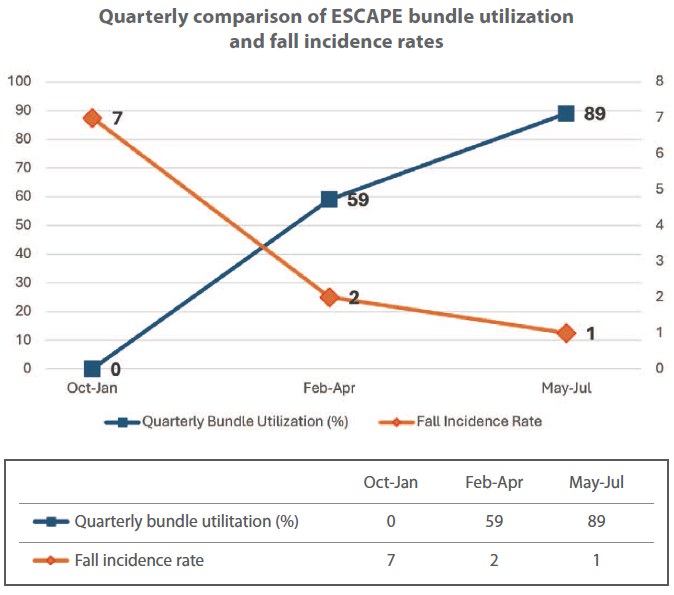
The percentage of nurses using the bundle grew substantially from February (25%) to July (90%) 2023, demonstrating effective adoption of the guidelines. We used the seven falls that occurred from October 2022 to January 2023 as the benchmark against which to measure the impact of the ESCAPE bundle. The reduction in falls from February to July 2023 marked a 71.4% decrease in fall rates from the baseline to the intervention phase. Moreover, the unit experienced a 50% decrease in fall incidence from the intervention to the post-intervention phase. These results suggest a strong association between consistent application of the ESCAPE bundle and decreased fall rates. (See Positive results.)
Positive results
This quarterly comparison indicates a strong association between increased ESCAPE bundle use and decreased fall rates.
Discussion
The ESCAPE strategy markedly decreased delirium and fall rates on the unit, aligning with our goal to improve patient safety and care. Research supports a strong link between delirium prevention and decreased fall rates, further evidenced by our project’s findings. However, unlike Kalivas’s study, which relied on retrospective data, our project applied the ESCAPE bundle directly in clinical settings, offering fresh insights from bedside practice.
This project extends the application of delirium prevention bundles from intensive care to the medical–surgical unit, addressing the high delirium risk among elderly patients. This approach fills a gap in existing research.
The significant drop in fall rates and incidence of delirium confirms the effectiveness of the ESCAPE approach in improving patient outcomes. This project aligns with and exceeds similar studies’ achievements, indicating substantial benefits from a structured care model. The outcomes include risk reduction for patients and decreased operational costs.
The extent of improvement, surpassing initial expectations, likely stems from strong staff engagement and patient compliance. Although initial training and adjustments introduced additional costs, the savings achieved from fewer extended stays and reduced fall litigation risk offer substantial financial advantages. Documentation time served as the ESCAPE approach’s main challenge; however, the intervention required no extra staffing and fit seamlessly into RNs’ existing workflows. Using a secure messaging system within the electronic health record for communication ensured efficient updates on patient conditions without additional workflow changes.
Limitations
Because we conducted this project on one unit in a single hospital setting, it may not reflect the diversity of all healthcare institutions. Future research and replication of the project in other hospitals require adequate knowledge of the educational interventions and staff perceptions of implementing the ESCAPE bundle.
Potential biases include the Hawthorne effect, where medical staff might have changed their behavior due to observation. To minimize biases, we collected anonymous feedback and strived to ensure staff comfort with the observation process.
Implications for nursing and health policy
This project underscores the importance of evidence-based delirium prevention strategies, including education, nursing documentation, and assessment. Although the project required nurse time, the benefits to patient safety and hospital metrics outweighed these challenges. The reduced overtime hours for one-to-one sitters indicate improved patient care and resource management. Further research is needed to identify reversible causes of delirium and reduce hospital length of stay.
Success and sustainability
The 71.4% reduction in falls during the intervention phase of this project and the 50% reduction post-intervention demonstrate the significant impact of the ESCAPE delirium prevention bundle. In addition, the 79% decrease in companion care hours and notably improved patient satisfaction scores underline the bundle’s effectiveness in enhancing patient safety and offering cost-efficient care.
Observed benefits and positive feedback indicate sustainability. To streamline processes, future efforts could include automated reports for easier monitoring and integration of the CAM screening into bedside hand-offs. Incorporating standardized communication could further support the program’s longevity by ensuring comprehensive awareness of patient needs among all staff.
The ESCAPE bundle has the potential for broader application across various healthcare settings. Ongoing research should leverage technology to refine and expand the model’s applicability. A multi-center trial could validate the approach’s effectiveness on a larger scale and across diverse patient populations, paving the way for widespread adoption.
The authors work at Presbyterian Westchester in Bronxville, New York. Thanoon Thabet is a clinical nurse. Catherine Lombardi is director of nursing. Alexis Aningalan is a wound and ostomy care manager.
American Nurse Journal. 2025; 20(9). Doi: 10.51256/ANJ092506
References
Anada S, Iigaya M, Takahashi M, Soda K, Wada N. Impact of early mobilization on the duration of delirium in elderly hospitalized patients: A retrospective cohort pilot study. Medicine. 2022;101(44):e31641. doi:10.1097/MD.0000000000031641
Burton JK, Craig LE, Yong SQ, et al. Non-pharmacological interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2021;7(7):CD013307. doi:10.1002/14651858.CD013307.pub2
Centers for Disease Control and Prevention. Cost of older adult falls. July 9, 2020. stacks.cdc.gov/view/cdc/122747
Chyou TY, Nishtala PS. Identifying frequent drug combinations associated with delirium in older adults: Application of association rules method to a case-time-control design. Pharmacoepidemiol Drug Saf. 2021;30(10):1402-10. doi:10.1002/pds.5292
Dutta C, Pasha K, Paul S, et al. Urinary tract infection induced delirium in elderly patients: A systematic review. Cureus. 2022;14(12):e32321. doi:10.7759/cureus.32321
Farasat S, Dorsch JJ, Pearce AK, et al. Sleep and delirium in older adults. Curr Sleep Med Rep. 2020;6(3):136-48. doi:10.1007/s40675-020-00174-y
Feinkohl I, Janke J, Slooter AJC, et al. Metabolic syndrome and the risk of postoperative delirium and postoperative cognitive dysfunction: A multi-centre cohort study. Br J Anaesth. 2023;131(2):338-47. doi:10.1016/j.bja.2023.04.031
Ten Ham-Baloyi W. Assisting nurses with evidence-based practice: A case for the Knowledge-to-Action Framework. Health SA. 2022;27:2118. doi:10.4102/hsag.v27i0.2118
He S, Rolls K, Stott K, et al. Does delirium prevention reduce risk of in-patient falls among older adults? A systematic review and trial sequential meta-analysis. Australas J Ageing. 2022;41(3):396-406. doi:10.1111/ajag.13051
Iglseder B, Frühwald T, Jagsch C. Delirium in geriatric patients. Wien Med Wochenschr. 2022;172(5-6):114-21. doi:10.1007/s10354-021-00904-z
Kalivas B, Zhang J, Harper K, et al. The association between delirium and in-hospital falls: A cross-sectional analysis of a delirium screening program. J Aging Res. 2023;2023:1562773. doi:10.1155/2023/1562773
Lee HJ, Bae E, Lee HY, Lee SM, Lee J. Association of natural light exposure and delirium according to the presence or absence of windows in the intensive care unit. Acute Crit Care. 2021;36(4):332-41. doi:10.4266/acc.2021.00556
Ludolph P, Stoffers-Winterling J, Kunzler AM, et al. Non-pharmacologic multicomponent interventions preventing delirium in hospitalized people. J Am Geriatr Soc. 2020;68(8):1864-71. doi:10.1111/jgs.16565
Ogrinc G, Davies L, Goodman D, Batalden P, Davidoff F, Stevens D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): Revised publication guidelines from a detailed consensus process. BMJ Qual Saf. 2016;25(12):986-92. doi:10.1136/bmjqs-2015-004411
Rossi Varallo F, Maicon de Oliveira A, Barboza Zanetti AC, et al. Drug-induced delirium among older people. In: Herdeiro MT, Roque F, Magalhães Silva T, Figueiras A (eds): New Insights into the Future of Pharmacoepidemiology and Drug Safety. IntertechOpen; 2021. doi:10.5772/intechopen.95470
Sampson EL, West E, Fischer T. Pain and delirium: Mechanisms, assessment, and management. Eur Geriatr Med. 2020;11(1):45-52. doi:10.1007/s41999-019-00281-2
Ueda N, Igarashi M, Okuyama K, et al. Demographic and clinical characteristics of patients with delirium: Analysis of a nationwide Japanese medical database. BMJ Open. 2022;12(9):e060630. doi:10.1136/bmjopen-2021-060630
Wang XT, Lyu L, Tang B, Wang C, Liu DW. Delirium in intensive care unit patients: Ten important points of understanding. Chinese Med J. 2017;130(20):2498-502. doi:10.4103/0366-6999.216405.
Wilson JE, Mart MF, Cunningham C, et al. Delirium. Nat Rev Dis Primers. 2020;6(1):90. doi:10.1038/s41572-020-00223-4
Zhao H, Ying HL, Zhang C, Zhang S. Relative hypoglycemia is associated with delirium in critically ill patients with diabetes: A cohort study. Diabetes Metab Syndr Obes. 2022;15:3339-46. doi:10.2147/DMSO.S369457
Key words: delirium, falls, patient safety


















2 Comments. Leave new
Helpful article
This was an interesting and helpful article