
Nurses need to engage in self-care to reduce moral distress.
Takeaways:
- The COVID-19 pandemic brings many ethical dilemmas for nurses and their patients.
- The ethical framework used during a crisis remains significantly different than in a normal state.
- This article provides an overview of the ethical framework used in crisis standards of care and begins to explore methods to support identifying and addressing moral distress at the bedside.
Disasters, including global pandemics such as COVID-19, disrupt standard care and present ethical challenges. Planning helps us prepare for disasters, but it can’t eliminate the ethical dilemmas and moral distress that clinicians will face. Staffing and supply shortages and patient surges require nurses and other healthcare providers to make decisions that may not align with standard care but are necessary under the circumstances. Familiarity with the ethical foundations for shifting standards of care will help nurses navigate moral distress and achieve some degree of resilience during challenging times.
Disaster planning
In 2009, the Institute of Medicine, motivated by a looming H1N1 pandemic, created a toolkit to guide disaster planning. The toolkit includes definitions for conventional, contingency, and crisis states with strategies for each state when communities are faced with a patient surge.
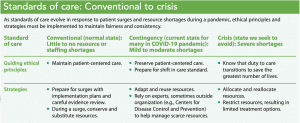
In our normal state, conventional, we can handle a surge of up to 120% of our normal intensive care unit (ICU) patients. To handle this minor surge, we may call in extra staff and conserve or substitute resources. When a larger surge of ICU patients (up to 200% of normal volume) occurs, we use contingency standards and begin to adapt and reuse. In contingency, the spaces, staff, and supplies used aren’t consistent with daily practices, but they support care that’s functionally equivalent to usual patient care practices. All of these efforts aim to avoid crisis. If crisis is reached, we must allocate and reallocate dwindling critical care resources with life-and-death consequences. (See Standards of care: Conventional to crisis.)
Many U.S. states have developed and made publicly available guidelines for crisis standards of care. Two main goals frame all disaster planning: Do everything to avoid a crisis state and, if those efforts fail, work to fairly save the greatest number of lives possible. Leaders will continue to refine plans, although no amount of planning can account for all that an emergency may bring. Leaders must, however, consider how to manage a surge.
Surge strategies
In the midst of the COVID-19 pandemic, many parts of the country are operating under contingency standards, and some organizations may be closer to crisis than others. For example, personal protective equipment (PPE) appears to be at or near crisis standards in many locations, with those in healthcare being asked to adapt and reuse PPE in ways normally considered unacceptable. Based on the best information available in a rapidly changing environment, we’re addressing resource shortages by conserving, substituting, adapting, reusing, and reallocating PPE and other supplies. (See Scarce resource allocation.)
Surge collaboration
Cities, counties, and states are collaborating to meet surge needs. For example, patients who arrive at a hospital lacking resources will be transferred to one that has what’s needed, or the resources will be redistributed to the hospital in need until all hospitals are at or near capacity. The decision to move to crisis standards of care is made by an institution, region, and/or state. For example, a state might declare a crisis at the state level, yet allow each hospital to determine whether it is at crisis. These types of decisions are made at the incident command level. Incident command varies by location; for instance, the person in charge could be a state health officer or a local hospital administrator.
This table illustrates how a resource (in this case, masks) is allocated during patient surges in conventional, contingency, and crisis states of a pandemic. Masks are the indicator, and percent reduction in supply is the trigger. Multiple strategies are applied as supplies diminish. (The % values are for illustration purposes only.)
| Mask allocation during patient surges | |||
| Conventional (surplus) | Contingency (20%) | Crisis (50%) | |
| Prepare |
| ||
| Conserve |
|
| |
| Substitute* |
|
| |
| Adapt* |
| ||
| Refuse* |
| ||
| Allocate** |
| ||
| Reallocate** |
| ||
*Per Centers for Disease Control and Prevention, U.S. Occupational Safety and Health Administration, and public health guidance
**Per regional, state, and/or federal guidance
Obligation to safety
Even optimal planning and collaboration often can’t eliminate ethical conflicts that may arise for nurses. These can arise partly because of nurses’ obligation to maintain safety—for our patients and ourselves. Safety guides our duty to care, and we rely on organizations to provide the PPE and other resources we need to maintain safety. Scarce PPE puts nursing practice ethics to the test. We may need to reuse and adapt PPE, accepting the risks to our patients and ourselves, because the alternative is providing no care at all. In addition, a crisis surge can result in lack of access to standard resources such as ICU nurses, impairing our ability to adhere to the ethical principles we’re used to, creating more conflict, which can lead to moral distress. (See Guiding ethical principles.)
Moral distress
A simple definition of moral distress is the feeling that occurs when we’re prevented from doing what we believe is right. When we experience moral distress, we feel compromised in our ability to practice as moral agents according to professional values and standards. Anyone working in healthcare during the current COVID-19 pandemic should expect to experience moral distress.
Shifting standards of care, interrupted patient relationships, triaging limited resources, working in unfamiliar environments, and uncertainty about disease progression and transmission are only a few of the potential sources of moral distress during the pandemic. For many, the change in how we care for dying patients has been a significant contributor to our moral distress. In many instances, visitor restrictions prevent families from being present when their loved one dies. Compassion and respect for patients have inspired some workarounds and exceptions; some organizations use video technology to allow virtual presence and others have designated a staff member to support a limited number of family members who, at their own risk, are permitted to visit a dying patient. None of these options feel right, because under normal circumstances global visitor restrictions would be unacceptable. But doing our best with current resource limitations has to be good enough.
These ethical principles should act as an overlay to professional codes of ethics and guide actions throughout the pandemic as patient surges and resource availability fluctuate.
- Fairness: Standards must be applied fairly and consistently.
- Transparency: Leaders must transparently communicate decisions and information to promote trust, particularly when circumstances require actions contrary to standard practice.
- Duty to care: The duty to care for the healthcare workforce tempers the duty to care for the community. Fidelity to individual patients is in tension with avoiding harm to the broader community.
- Consistency: We must provide consistency in how scarce resources are allocated.
- Duty to steward resources: Scarce resources must be allocated fair- ly using the utilitarian goal of saving the greatest number of lives.
- Proportionality: Actions must be in proportion to the emergency and the degree of scarcity.
- Accountability: Nurses must be accountable for the just allocation of scarce resources.
Addressing moral distress
Mapping your moral distress is an effective strategy for navigating the experience. (Click here for a visual image that illustrates how to map moral distress) Acknowledging and naming the emotions that define your distress is the first step to reflecting on it. Then challenge yourself to move beyond your immediate emotional response and apply ethical frameworks to the actions available to you. Although you may not agree with the options, seeking to understand the ethical rationale may help you understand the context of the constraints in the ethically permissible actions available. When possible, organizations may want to provide opportunities for staff to discuss ethical challenges, facilitated by someone trained in ethics. (See Self-care strategies and resources.)
ANA Code of Ethics
Turning to the American Nurses Association (ANA) Code of Ethics for Nurses with Interpretive Statements during the pandemic may help nurses shift our focus and decrease moral distress. During a pandemic, we move away from a focus on relationship-centered care (Provision 2, Commitment to Patient) and adopt an outcome-based framework (Provision 8, Promotion of Community and World Health) with the two primary goals mentioned earlier: Use strategies to avoid entering crisis standards of care and, if crisis is unavoidable, work to fairly save the greatest number of people possible.
Despite this shift, Provisions 1 and 5—Compassion and Respect for Every Person and Equal Duty to Self—remain constant; we always practice with compassion and respect, and we owe the same duty to ourselves that we do to patients. These standards can be hard to accept, especially if it means self-protection compromises a response to a patient. It creates a tension between avoiding harm (nonmaleficence) to oneself and doing good (beneficence) for a patient. However, failing to protect ourselves compromises the patient in front of us and our ability to care for future patients.
Nurses must take concrete steps to care for ourselves during the pandemic. Be intentional about:
- taking breaks
- eating nutritious food
- getting adequate sleep
- acknowledging the emotional toll of the situation and seeking support.
You may find the following resources helpful.
- American Association of Critical Care Nurses: This site offers clinical re- sources related to COVID-19, including information about moral distress and how nurse managers can mitigate nurse post-traumatic stress disorder.
- American Nurses Association (ANA): This site offers access to free webinars, applications for funds, ethical considerations, and other resources.
• down dog: This app (which includes yoga for beginners, high-intensity interval training, barre, and 7-minute workouts) is available for free to all healthcare professionals through January 1, 2021.
• 425Magazine: This article outlines the COVID-19 visitation procedure developed by nurses at Virginia Mason.
• First Aid Arts: Access science-based arts activities to help reduce stress and build resilience.
• Headspace: This app is offering free access to videos to aid in meditation, sleep, and movement.
• Mindfulness for Healthcare Workers During COVID: Access mindful- ness practices and meditations.
• National Suicide Prevention Life- line: This resource can be accessed around the clock by phone: 1-800-273-8255.
• 9TO5Mac: This site offers links to apps and services providing free wellness information during the COVID-19 pandemic.
• Project Parachute: Pro-bono teletherapy for COVID-19 frontline
Unfortunately, a code of ethics doesn’t eliminate the challenges of making sound ethical decisions. Barriers to doing the “right thing” (such as not having sufficient supplies to care for patients) create ethical tensions in a pandemic. Internal and external constraints influence our actions, making us feel as though we’re violating our professional integrity by not providing the care patients deserve and that we’re capable of providing, if only we had more resources.
Ethical reflection
The COVID-19 pandemic puts two ethical frameworks in direct tension with each other. In standard practice, nurses embrace a principle- or virtue-based framework that focuses on respect for patient autonomy. We strive to help patients in front of us navigate their illness or injury and minimize suffering; our patients, in a normal state, guide our work. However, when resources are severely limited, we’re asked to participate in a shift that means some patients may not have access to the treatment they desire. This utilitarian framework asks organizations to work together to achieve the greatest good for the greatest number of people in their shared communities. Crisis standards of care are designed to provide fairness through the equitable allocation of scarce resources.
However, a fair process during a disaster may not feel fair, and doing our best may not feel like enough when individual patient needs outpace our ability to meet them. We should strive for our best and be forgiving when it doesn’t feel good enough. We can minimize harm by speaking up, seeking support inside and outside of our organizations, and leading the way to forge creative paths forward. We don’t know how long the COVID-19 pandemic will last, but as the surge of patients fluctuates, we must act to minimize the strain of looming cumulative distress now. Work must continue to outline methods of support during this acute phase until we reach a place to rebuild.
The declaration of a public health emergency has shifted some elements of the standards of care already. We must prevent further spread of the disease, which can’t be achieved without protecting healthcare providers so we can safely care for patients. That means we must preserve scarce PPE for those at the bedside by limiting visitation and postponing elective surgeries as able. How we demonstrate compassion in a crisis will, by necessity, look and feel different. It may not feel good to not have access to the choices we’re used to, but this doesn’t mean individual providers are doing anything wrong. The PPE shortage has exposed gaps in our health system, but the pandemic requires that we put our trust in a flawed system. We must act together to promote solidarity and work to provide equitable care to our community and patients.
These are uncertain times. Sadly, no perfect options exist during a pandemic, but moral distress can be mitigated when we listen to all perspectives, identify sources of conflict, and, when presented with limited choices, seek to identify options that minimize moral harm. Nurses must continue to speak up and reach out. We can bring calm to our patients, our community, and our profession during this challenging time. We’re in this together.
Laura Webster is the bioethics program director at Virginia Mason in Seattle, Washington, and affiliate faculty in the department of bioethics and humanities at the University of Washington School of Medicine in Seattle. Lucia D. Wocial is an adjunct assistant professor at Indiana University School of Nursing in Indianapolis.
References
American Nurses Association. Code of Ethics for Nurses with Interpretive Statements. Silver Spring, MD: American Nurses Association; 2015. nursingworld.org/practice-policy/nursing-excellence/ethics/code-of-ethics-for-nurses
American Nurses Association. Crisis Standard of Care: COVID-19 Pandemic. 2020. nursingworld.org/~496044/globalassets/practiceandpolicy/work-environment/health–safety/coronavirus/crisis-standards-of-care.pdf
Berlinger N, Wynia M, Powell T, et al. Ethical Framework for Health Care Institutions Responding to Novel Coronavirus SARS-CoV-2 (COVID-19): Guidelines for Institutional Ethics Services Responding to COVID-19. The Hastings Center. March 16, 2020. thehastingscenter.org/wp-content/uploads/HastingsCenterCovidFramework2020.pdf
Chiafery MC, Hopkins P, Norton SA, Shaw MH. Nursing ethics huddles to decrease moral distress among nurses in the intensive care unit. J Clin Ethics. 2018;29(3):217-26.
Curtis JR, Kross EK, Stapleton RD. The importance of addressing advance care planning and decisions about do-not-resuscitate orders during novel coronavirus 2019 (COVID-19). JAMA. March 27, 2020. jamanetwork.com/journals/jama/fullarticle/2763952
Daugherty Biddison EL, Faden R, Gwon HS, et al. Too many patients…A framework to guide statewide allocation of scarce mechanical ventilation during disasters. Chest. 2019;155(4):848-54.
Dudzinski DM. Navigating moral distress using the moral distress map. J Med Ethics. 2016;42(5):321-4.
Emanuel EJ, Persad G, Upshur R, et al. Fair allocation of scarce medical resources in the time of Covid-19. N Engl J Med. 2020;382(21):2049-55.
Hamric AB, Epstein EG. A health system–wide moral distress consultation service: Development and evaluation. HEC Forum. 2017;29(2):127-43.
Hick JL, Hanfling D, Wynia MK, Pavia AT. Duty to plan: Health care, crisis standards of care, and novel coronavirus SARS-CoV-2. NAM Perspectives. March 5, 2020. nam.edu/duty-to-plan-health-care-crisis-standards-of-care-and-novel-coronavirus-sars-cov-2
Institute of Medicine (US) Committee on Guidance for Establishing Standards of Care for Use in Disaster Situations. Guidance for Establishing Crisis Standards of Care for Use in Disaster Situations: A Letter Report. Washington, DC: National Academies Press; 2009.
Papadimos TJ, Marcolini EG, Hadian M, et al. Ethics of outbreaks position statement. Part 1: Therapies, treatment limitations, and duty to treat. Crit Care Med. 2018;46(11):1842-55.
Papadimos TJ, Marcolini EG, Hadian M, et al. Ethics of outbreaks position statement. Part 2: Family-centered care. Crit Care Med. 2018;46(11):1856-60.
Truog RD, Mitchell C, Daley GQ. The toughest triage—Allocating ventilators in a pandemic. N Engl J Med. 2020;382(21):1973-5.
Vaughn L. Bioethics: Principles, Issues, and Cases. 3rd ed. New York: Oxford University Press; 2016.
Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet. 2020;395(10229):1054-62.


















1 Comment.
Thank you so very much for this valuable article. The article is valuable in that it provides the important steps health professional can take to identify the internal conflicts, acknowledge moral distress, and speak out about our experiences in a productive fashion.