
Assessment, treatment, and self-management
Takeaways:
- Epilepsy is a complex disease that includes seizures that may or may not be active.
- Recognizing comorbidities can improve health and quality of life outcomes.
- People with epilepsy who continue to have seizures during treatment with the first or second medication should be referred to a comprehensive epilepsy center.
- Nurses are critical to increase awareness of epilepsy and the need for comprehensive care in inpatient and outpatient settings.
EPILEPSY is one of the most common disorders of the central nervous system, affecting 65 million people worldwide—3.4 million in the United States. It can occur with or without a known cause (60% of cases have no known cause) and is diagnosed when seizures are spontaneous and recurrent (two or more unprovoked seizures). One of the fastest-growing populations developing epilepsy is veterans who sustained complicated traumatic brain injuries (TBIs) as a result of exposure to explosive blasts and post-traumatic stress disorder. Automobile accidents and falls also contribute to TBI with secondary epilepsy.
Patients with epilepsy may have a specific seizure or seizure types depending on their epilepsy syndrome/diagnosis. All patients with epilepsy are at risk for secondary generalized tonic-clonic seizures.
Seizures
Seizures occur when uncontrolled electrical neuronal brain discharges interrupt normal brain function. They’re relatively common and are associated with many neurologic disorders, including tumors, trauma, and infectious processes such as meningitis. They also may occur with non-neurologic disorders, such as dehydration and other metabolic problems. Seizures can occur at any age, but they’re most common in children and in people more than 60 years old. Many types of seizures have been identified, and each is associated with different presentations, symptoms, and treatment regimens. Effective care for patients with seizures requires the healthcare team to know about the different types, their presentations, and available treatments.
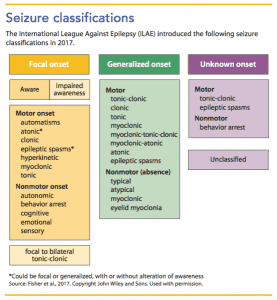
In 2017, the International League Against Epilepsy (ILAE) introduced new information about seizure classification. Seizures are classified as focal (originating in one area of the brain), generalized (crossing both hemispheres of the brain), unknown (onset of seizure activity can’t be determined), or unclassified (inadequate information or inability to place in other categories). A focal seizure can be further differentiated by whether the person maintains awareness during the seizure. (See Seizure classifications.)
Common seizures
Describing what occurs before, during, and immediately after a seizure can assist with classification and may help identify the area of the brain from which the seizure originated.
In the outpatient or community setting, nurses may observe any type of seizure. Focal seizures, which can present with preserved or altered awareness, require supportive care until the seizure ends. Remember that bystanders and first responders sometimes confuse focal seizure symptoms with behavior problems or illicit drug use. Nurses are a critical educational source for loved ones, caretakers, and other community members who might need to assist a person experiencing a seizure.
Generalized motor seizures with tonic-clonic activity involve stiffness and jerking of the body with loss of consciousness. When this type of seizure lasts more than 5 minutes, it’s considered status epilepticus, a medical emergency that requires pharmacologic intervention to stop prolonged seizure activity. Status epilepticus is focal or generalized seizure activity that lasts more than 30 minutes, but healthcare providers typically treat nonstop seizure activity when it lasts more than 5 minutes to prevent complications.
Other generalized seizures can occur in nonstop patterns, such as nonmotor (absence seizures), which are common in childhood and typically last 30 seconds or less before the person returns to his or her normal baseline. Teachers may inform school nurses that a child doesn’t seem to be paying attention and has a decline in school performance. The nurse may consider attention or learning disorders, but absence epilepsy syndrome should be ruled out if frequent, brief staring events where the child is unresponsive are observed. Absence seizures that last more than 5 minutes are considered nonmotor status epilepticus, and medication is needed to stop them.
Families need to know seizure first aid as any seizure can secondarily generalize to a motor (tonic-clonic) seizure, and subsequently, result in status epilepticus. (See Seizure first aid.) Nurses can teach families about first aid and work with patients and families to develop a seizure action plan that highlights what to do if a breakthrough or prolonged seizure occurs. The plan can be modified as needed for inpatient versus outpatient care (epilepsy.com/learn/managing-your-epilepsy/seizure-response-plans-101).
Seizure first aidHelp patients with epilepsy and their families prepare for seizures by teaching them about seizure first aid.
Source: Epilepsy Foundation (epilepsy.com) |
Sudden unexplained death in epilepsy
The risk of sudden unexplained death in epilepsy (SUDEP) is about one in 1,000. How and why SUDEP occurs is still being researched. Typically, evidence is found of a seizure occurring before SUDEP. SUDEP can be difficult to discuss with patients and families, but understanding it and knowing what to do can reduce risks. (See Reducing SUDEP risk.)
Reducing SUDEP riskSudden unexplained death in epilepsy (SUDEP) typically occurs following a seizure. Educate patients about SUDEP and take steps to reduce the risks.
Source: Shorvon and Tomson, 2011 |
Comorbidities
Epilepsy is considered a spectrum disorder because of its potential effects on cognitive, behavioral, physical (such as muscle weakness, fine and gross motor coordination disorders, migraines, fertility issues), and social areas (such as social isolation) of life as well as core pathologies shared by seizures. In addition, many individuals with epilepsy face obstacles to appropriate healthcare, education, employment, and family planning. Adults who were diagnosed with epilepsy in childhood are less likely to be well educated and are two to three times as likely to be unemployed as the general population. They may experience decreased autonomy and social difficulties related to appropriate restrictions (driving, high-impact sports, swimming) and increased supervision recommended by epilepsy healthcare providers. The stigma of epilepsy is longstanding and is second only to the stigma of HIV.
Approximately 40% to 60% of people with epilepsy experience mental/behavioral health and neurodevelopmental symptom disorders. For example, attention-deficit hyperactivity disorder (ADHD) has a prevalence rate of 30% to 40% in people with epilepsy compared with only 6% to 12% in the general population. Even in the absence of an ADHD diagnosis, many patients experience inattention and executive functioning deficits, which may require intervention. Other common mental/behavioral health comorbidities are depression (25% experience depression symptoms and 20% report suicidal ideation) and anxiety (30% report anxiety symptoms).
One of the most important health goals for patients living with epilepsy is good quality of life. Nurses who understand the comorbidities can provide education, facilitate screening, and make referrals to resources that support people with epilepsy and their families. (Click for a PDF of Free screening tools.)
Evaluation
When a person has a seizure, a clinical description of the event, comprehensive patient history, including psychiatric/behavioral health history, and complete physical assessment are typically performed by the primary care provider to begin the seizure evaluation. At a minimum, a complete blood count and an electrolyte panel are ordered. If the patient appears impaired, a toxicology screen is obtained. If the patient has a fever or is immunocompromised without a fever, a lumbar puncture may be ordered to determine if an infection is the cause of the seizure. In most cases, an electroencephalogram (EEG) is ordered to determine the seizure type and possible epilepsy syndrome. Specific patterns are associated with epilepsy syndromes. A nonspecific abnormal EEG doesn’t indicate a diagnosis of epilepsy, and a normal EEG doesn’t indicate the absence of epilepsy. EEG patterns change during the developmental stages of life, so a neurologist or epileptologist should evaluate the EEG.
If the patient’s neurologic exam and EEG are abnormal and seizure activity continues even with medication, he or she should be referred to an center. After evaluation at the epilepsy center, other assessments— such as magnetic resonance imaging of the brain with epilepsy protocol and neuropsychological, psychiatric/behavioral health, occupational, speech, and physical function evaluations—may be warranted. If determining the seizure type or epilepsy syndrome is difficult, an inpatient admission for a prolonged video-EEG may be scheduled. Video-EEGs (simultaneous recording of the patient’s brain and behavior to compare clinical symptoms of the seizure with the EEG findings) help determine the epilepsy syndrome and evaluate for other treatment options, including surgery. Typically, at least three seizures are recorded before terminating the video-EEG. If a person is determined to be a possible epilepsy surgery candidate, he or she may be scheduled for other tests, including those that look at brain activity and seizure onset location.
Treatment
Epilepsy treatment includes antiepileptic drugs (AEDs), surgery, neurostimulation, and diet. However, the overarching goal for patients and families living with epilepsy is management using health behaviors and related processes (cognitive, emotional, and social). Even when a patient adheres to medication recommendations, gets enough sleep, decreases stress, and makes other lifestyle modifications, a seizure still can break through. With self-management, the patient and family can promote quality of life and achieve the best health outcomes.
Antiepileptic drugs
Many medications are used to treat epilepsy, and critical factors must be considered in choosing the best medication for each patient. For example, some AEDs are indicated for certain types of seizures and/or epilepsy syndromes. Other considerations include patient characteristics such as age, sex, ethnicity, and comorbid conditions. Divalproex/valproic acid is a broad-spectrum AED, but young women may have side effects, such as irregular menses, weight gain, fatigue, possible polycystic ovarian syndrome, and risk of fetal abnormalities. Topiramate may be a good choice for patients who also have migraines and are overweight, but it’s not appropriate for patients who have cognitive issues, are underweight, have appetite issues, or are prone to kidney stones. Generic medications may need to be considered due to insurance plan coverage or drug availability.
Patient and family resourcesRefer patients and families to these resources to learn more about living with epilepsy. American Academy of Pediatrics: National Coordinating Center for Epilepsy Centers for Disease Control and Prevention—Epilepsy: You Are Not Alone: Resource Guide Epilepsy Foundation Job Accommodation Network—Epilepsy Seizure Disorder: Accommodation and compliance: Accommodating employees with epilepsy/seizure disorder Managing Epilepsy Well Network World Health Organization—Global Campaign Against Epilepsy: Out of the Shadows |
Cannabidiol (CBD), one of 113 cannabinoids identified in marijuana, appears to decrease seizures in patients with severe forms of epilepsy such as Lennox-Gastaut syndrome or Dravet syndrome. Epidiolex® is the only CBD approved for treating severe forms of epilepsy. CBD oil is gaining in popularity, and nurses should explain to patients that Epidiolex is the only cannabinoid safe for treating epilepsy. Other cannabinoids may cause more seizures or unwanted side effects. Ask patients if they’re taking any nutritional supplements or herbs; some can cause increased seizures or be contraindicated with AEDs. You can find an AED reference guide at journals.sagepub.com/toc/epib/18/4_suppl.
AED adverse effects. Be aware of potential AED adverse effects and ask patients about them at each visit or during any communication. Many adverse effects resolve with time and occur with less frequency and severity if a low AED dose is slowly titrated up to a therapeutic level. Common adverse effects of AEDs include nausea and vomiting, drowsiness and fatigue, dizziness, blurred vision, appetite changes, tremor, and behavioral, attention, and mood changes. AEDs that are processed through the liver or kidneys can have potential effects on organ function, so intermittent blood work is indicated. Some AEDs can impact white blood cells (carbamazepine) or platelets (valproic acid), requiring periodic lab work. Some AEDs (for example, carbamazepine, oxcarbazepine, and valproic acid) can stabilize mood but others (for example, levetiracetam, topiramate, and zonisamide) can cause or worsen depression. Medication dose increases or decreases may affect mood or sleep, and all AEDs have the potential to cause an allergic reaction in the form of a skin rash that typically occurs during the first 6 months of treatment. A skin rash can progress to the potentially fatal Stevens-Johnson syndrome, so patients should contact their primary care providers to report any worsening skin rash. Most AEDs have established blood drug levels that can be monitored to evaluate efficacy and adverse effects (journals.sagepub.com/toc/epib/18/4_suppl).
The overlap among AED adverse effects, behavioral health disorders, and seizure symptoms creates challenges for patients, families, and healthcare providers. Comorbid behavioral health symptoms can worsen the severity of adverse effects associated with AEDs. Not surprisingly, these comorbidities also are associated with poor adherence to prescribed AED regimens and health-related quality of life. More than half of families of children with new-onset epilepsy and one-third of adults with epilepsy have difficulty following the prescribed AED regimen in the first few months of treatment. Lack of epilepsy knowledge, forgetting to take medications, poor coping skills (problem-solving, communication, and epilepsy management), and perceived lack of social support contribute to non-adherence.
Refractory epilepsy. If the first prescribed AED doesn’t reduce or eliminate seizures, investigate why. For example, is the epilepsy refractory (up to 40% of patients will have difficult-to-control or refractory epilepsy), is the diagnosis correct, are nonepileptic events occurring, did the patient adhere to the AED regimen, or has a medication error occurred? The next AED must be chosen after careful review of the diagnosis, including whether the seizures are indeed epileptic.
If two AEDs haven’t controlled seizures, refer the patient to an epilepsy center to re-evaluate the diagnosis and explore other possible treatments. In addition to daily medications and nonpharmacologic treatments, patients with epilepsy who have breakthrough seizures may need seizure rescue medications such as benzodiazepines (for example, diazepam that can be administered rectally or intramuscularly or lorazepam administered intranasally).
Nonpharmacologic treatment
Nonpharmacologic treatments for refractory epilepsy include surgery, neurostimulation, and diet. These treatments should be provided by an interprofessional team at a comprehensive epilepsy center.
Surgery. The goal of surgery is to stop the seizure activity (resection, ablation) or to prevent the spread of disabling seizures (disconnection). Surgical options include resection or ablation of the brain tissue causing seizures or severing of specific nerve pathways (disconnection) to stop seizures from spreading. All surgeries carry the risks of bleeding, infection, and death.
Recovery from surgery may include rehabilitative therapies, depending on the area of the brain treated. Up to 68% of patients who have epilepsy surgery will achieve seizure freedom. Patients should undergo neuropsychological evaluation pre- and postsurgery to track any changes in neurocognitive and behavioral and emotional functioning.
Neurostimulation. For patients who aren’t surgical candidates, neurostimulation via vagus nerve stimulation (VNS) or responsive neurostimulation (RNS) may be an option. The VNS device is a small stimulator surgically implanted under the left clavicle with a lead attached from the device to the left vagus nerve. The electrical stimulation is programmed wirelessly and provides ongoing intermittent stimulation that changes levels of neurotransmitters in the brain, which results in decreased seizure frequency and/or length. The device can provide additional on-demand stimulation to stop or shorten a breakthrough seizure with use of a magnet applied to the VNS implant through clothes.
VNS adverse effects include voice alteration, coughing, or throat discomfort during stimulation; these events decrease with dose adjustment. VNS therapy is well tolerated and appears to have a positive cumulative effect on decreasing seizures over time. In a recent study, up to 60% of patients with refractory epilepsy experienced decreased seizures. VNS also is used in patients with refractory depression; patients with epilepsy also report improved mood, increased alertness, and better focus.
RNS is appropriate for patients who have focal seizures with a defined area of seizure onset (for example, seizure activity localized to both temporal lobes) that can’t be removed or ablated. The RNS device is a small microcomputer implanted in the skull with electrodes placed close to the source of the seizures. Similar to VNS, the goal is to reduce seizure activity with electrical stimulation and to provide additional stimulation to stop breakthrough seizures. The RNS records data that are transmitted to a website so the neurologist/epileptologist can review and make any needed changes using a handheld wand and laptop computer.
Common RNS adverse effects include abnormal thinking or confusion, dizziness, drowsiness, headache, nausea, and vomiting. The RNS is typically well tolerated. A recent study demonstrated that almost 50% of patients with refractory epilepsy achieved a seizure reduction of 50% or more over 2 years of therapy, with an additional 7% achieving seizure freedom.
Diet. Evidence has demonstrated that special diets can decrease seizures in patients with epilepsy. The classic epilepsy diet is ketogenic and has been studied mostly in children. In children with refractory epilepsy, 50% to 60% experience seizure reduction, up to 33% experience a 90% reduction, and more than 10% are seizure free. The diet isn’t difficult to learn but requires a firm commitment from families and a complete change in dietary behaviors.
The ketogenic diet appears to alter neurotransmitter activity and increase cerebral energy and metabolism through ketosis (using ketones as a source of energy rather than glucose). A recent consensus guideline developed by dietitians and neurologists recommends the ketogenic diet after two AEDs have failed and as the first line of treatment for certain glucose metabolism disorders (for example, glucose transporter type 1 deficiency syndrome and pyruvate dehydrogenase deficiency). Patients with epilepsy must be screened for contraindications, such as fatty metabolism disorders. The diet can be used in inpatient or outpatient settings.
The dietitian is critical to educating the family and developing recipes and meal plans. A written seizure treatment plan, which includes a “sick day” plan with food and hydration options, must be readily available because patients on this diet can’t receive I.V. infusions with glucose or other glucose products, which will alter ketosis. A “sick day” plan should include food and hydration options. Patients and their families must commit to a 3- to 6-month trial; the diet is typically used for at least 2 years. Side effects include abdominal pain, bone density loss, constipation, dehydration, diarrhea, hyperlipidemia, hypoglycemia, kidney stones, and reflux. These effects can be eased with diet adjustments and appropriate supplement therapy. Regular laboratory evaluation helps to maintain good health.
Less-restrictive epilepsy diets, including the modified Atkins diet for epilepsy and the low glycemic index diet, can provide improved seizure control and may be easier to maintain.
Treating psychiatric/behavioral health comorbidities
Assessing behavioral health symptoms before initiating AED treatment (and periodically during treatment) helps the healthcare team differentiate comorbid behavioral health symptoms related to AED adverse effects and address adherence to the AED regimen. Healthcare providers and families also must balance AED efficacy with adverse effects and quality of life when making treatment decisions. Medication can be adjusted or nonmedication interventions can be implemented.
Healthcare providers should use a three-tiered stepped-up health promotion approach. The first tier includes cognitive and behavioral health screening and asking patients and families about their self-management awareness and needs. If mild concerns are noted and the family has strong resources, a community-based referral (for example, a local Epilepsy Foundation advocacy group) or broad epilepsy self-management resources (for example, a vetted educational website) may be sufficient. If significant concerns are noted, clinicians should make referrals to a mental or behavioral health professional for further evaluation.
At the second tier, clinicians should perform a more comprehensive evaluation for patients at risk for self-management challenges, such as those with refractory epilepsy, behavioral health or neurodevelopmental diagnoses, and adherence challenges. At this level, screen for particular concerns (for example, depression screening if depressive symptoms are reported). Referrals for further evaluation and specific treatment and interventions (adherence, coping skills, depression) may be necessary.
The third tier targets patients with known comorbid neurodevelopmental behavioral health disorders and/or a history of treatment nonadherence. Inquire about current symptom severity, self-management challenges, and behavioral health support (for example, is the patient receiving behavioral health services or educational or vocational support). If the patient isn’t receiving adequate services, refer him or her for indicated services as necessary. The provider should consider pharmacologic and nonpharmacologic interventions to treat specific disorders or nonadherence.
Evidence indicates the effectiveness of psychological-based treatments that focus on epilepsy self-management, specific behavioral health symptoms (depression, anxiety), quality of life, and treatment nonadherence. Most interventions are skills-based and emphasize coping, cognitive restructuring, problem-solving, and mood-enhancing behaviors. Evidence also supports using psychotropic medications with patients who have ADHD, depression, or anxiety.
Consider the developmental level of children with epilepsy when involving them in care and self-management. There’s no ideal age for introducing independence into epilepsy self-care, and research in other pediatric chronic illnesses has found variability depending on a child’s level of understanding. Healthcare providers and families should use their discretion but involving children in their epilepsy management as much as possible is advised and will help them transition to adult care.
Most children with epilepsy (with or without other diagnoses) need caregivers to support them being able to self-manage their condition, and those challenges may not remit as they age. Similar to very young children with epilepsy, children with developmental disabilities will require primary caregiver involvement in their epilepsy management, and providers will need to engage and support caregivers in this commitment to long-term care for their children.
Nursing implicationsNursing care for patients with epilepsy focuses on education, self-management, and comorbidity assessment.
|
Promote self-management
Epilepsy is a complex disease with seizures that may or may not be controlled, a high rate of behavioral health and neurodevelopmental comorbidities, and a first-line treatment with potentially significant adverse effects. The complexities of epilepsy can impact a patient’s life and ability to participate fully in school, work, and the community. A nurse’s role in caring for patients with epilepsy includes teaching them about their condition (including seizure first aid, side effects, and SUDEP) and referring them to self-management resources. (See Nursing implications.) Comprehensive epilepsy care, in addition to controlling seizures and treating comorbid symptoms and conditions, includes optimizing quality of life.
Gigi Smith is executive associate dean for academics and a professor at Medical University of South Carolina College of Nursing in Charleston, South Carolina. Madona Plueger is an adult health clinical nurse specialist in neuroscience nursing at Dignity Health St. Joseph’s Hospital and Medical Center Barrow Neurological Institute in Phoenix, Arizona. Janelle L. Wagner is a research associate professor at Medical University of South Carolina College of Nursing.
Selected references
England MJ, Liverman CT, Schultz AM, Strawbridge LM, eds. Epilepsy Across the Spectrum: Promoting Health and Understanding. Washington, DC: National Academies Press; 2012.
Fisher RS, Cross HJ, French JA, et al. Operational classification of seizure types by the International League Against Epilepsy: Position paper of the ILAE commission for classification and terminology. Epilepsia. 2017;58(4):522-30.
Hickey JV. Seizures. In: The Clinical Practice of Neurological and Neurosurgical Nursing. 7th ed. Philadelphia: Wolters Kluwer/Lippincott Williams and Wilkins; 2014; 643-66.
Kossoff EH, Wang HS. Dietary therapies for epilepsy. Biomed J. 2013;36(1):2-8.
Michaelis R, Tang V, Wagner JL, et al. Cochrane systematic review and meta-analysis of the impact of psychological treatments for people with epilepsy on health-related quality of life. Epilepsia. 2018;59(2):315-32.
Miller WR, Young N, Friedman D, Buelow JM, Devinsky O. Discussing sudden unexpected death in epilepsy (SUDEP) with patients: Practices of health-care providers. Epilepsy Behav. 2014;32:38-41.
Modi AC, Pai AL, Hommel KA, et al. Pediatric self-management: A framework for research, practice, and policy. Pediatrics. 2012;129(2):e473-85.
Selassie AW, Wilson DA, Martz GU, Smith GG, Wagner JL, Wannamaker BB. Epilepsy beyond seizure: A population-based study of comorbidities. Epilepsy Res. 2014;108(2):305-15.
Shorvon S, Tomson T. Sudden unexpected death in epilepsy. Lancet. 2011;378(9808):2028-38.
Vossler DG, Weingarten M, Gidal BE. Summary of antiepileptic drugs available in the United States of America. Epilepsy Currents. 2018;18(4). journals.sagepub.com/toc/epib/18/4_suppl
Wang HS, Lin KL. Ketogenic diet: An early option for epilepsy treatment, instead of a last choice only. Biomed J. 2013;36(1):16-7.
ant7-CE Epilepsy-617a
















2 Comments.
Yes click under the title of the article where it says you can take the test, it’s a red button
This was very interesting and I learned more about seisures. Is there a place to take a test for CEU’s