
Expand capacity, increase patient satisfaction, improve outcomes
Takeaways:
- Outside of the United States, countries such as England, Canada, and Australia have long operated hospital-at-home programs.
- Studies indicate that hospital at home can lower costs, reduce length of stay, and improve patient satisfaction.
- as more health systems partner with payers to create value-based care arrangements, delivering more cost-effective, high-quality care outside the hospital becomes even more attractive.
On July 13, 2020, Sue Davis drove her husband of 33 years, Richard (Allen) Davis, to the emergency department (ED). Three days later, she was so ill she could barely get out of bed and eventually drove herself to the ED at the urging of her family physician at Indiana University Health (IU Health). She spent 10 days in the hospital (her husband died) and was then discharged home to become part of the IU Health hospital-at-home program, which provides remote around-the-clock care. She received virtual nursing and daily nurse practitioner (NP) visits. With the help of her daughter, Davis was an ideal candidate for the program and remained in its care for 3 weeks.
Davis is one of more than 1,500 patients who had COVID-19 and benefitted from the collaborative interprofessional IU Health program between April 2020 and January 2022. The team includes members of IU Health specialties and service lines who worked together in 2020 to define program eligibility criteria, which encompass medical factors such as condition severity, pre-existing conditions, vital signs, oxygen levels, and social factors (for example, having a caregiver at home and adequate housing). (See Hospital-at-home criteria.)
Hospital-at-home criteria
Leadership at Indiana University Health developed the following criteria for discharging patients with Covid-19 to its hospital-at-home program.
- The inpatient provider gives approval.
- The patient shows an improved or resolved fever that doesn’t exceed 100.4° F (38.0° C) for 24 hours off antipyretics.
- Patient’s dyspnea and other respiratory symptoms have improved.
- Patient’s oxygen requirement has decreased.
- Oxygen saturation >88%
- Maximum oxygen requirement 6 liters by nasal cannula
- Patients weaned down on oxygen 24 hours before discharge should be given standard as-needed oxygen orders that allow them to go home with an oxygen tank.
- Patient must have adequate housing and home support.
- An appropriate adult support person must be available at home 24/7 for at least the first 48 hours after discharge. (Indicate need for a translator on the hospital-at-home referral.)
- For patients still requiring isolation, a separate bedroom must be available where the patient can recover without sharing immediate space with others.
- The patient must have resources for access to food and other necessities.
- Provide the patient and support person with masks at discharge. They must be capable of adhering to precautions (respiratory hygiene, cough etiquette, hand hygiene) recommended as part of home care or isolation.
- Patients and high-risk household members should adhere to Centers for Disease Control and Prevention guidelines to lower transmission risk, including mask wearing, avoiding shared surfaces, distancing, and hand hygiene. The patient and family can pursue enrollment if they have high-risk individuals in the household, but the hospital-at-home team may decline a referral if the patient doesn’t meet criteria or if the risk is unacceptable to the patient or caregiver.
- A smart device (phone, tablet) is preferred but not required.
- Patients who live in group homes are ineligible.
- The patient must be able walk to the bathroom or bedside commode with the help of no more than one person.
- Family and patient education about warning signs of deterioration and appropriate protective precautions as applicable must be provided.
- For any concerns about the patient’s ability to perform activities of daily living (ADLs), physical therapy and occupational therapy should perform an assessment prior to program enrollment.
- If a patient doesn’t require assistance with transfers, ambulation, or ADLs, document this information in the patient record.
- Patients with unmanaged co-morbid conditions are ineligible.
- Patients with confusion or lethargy are ineligible.
- Patients with dementia are ineligible.
- Patients shouldn’t be discharged if they’re expected to arrive at their home after 6:00 pm.
Hospital-at-home history
Outside of the United States, countries such as England, Canada, and Australia have long operated hospital-at-home programs because payment policies encourage delivering healthcare in less-costly venues. For example, notes Klein, in Australia every metropolitan and regional hospital has such a program, providing approximately 6% of all hospital days at home. Recently, some U.S. health systems have instituted hospital-at-home with dramatic savings to both Medicare and private payers.
Much of the savings comes from eliminating the fixed costs associated with operating a hospital and freeing up bed space for other conditions. One of the earliest examples of hospital-at-home in the United States occurred in 1994 at Johns Hopkins Medicine, a health system near Baltimore, MD. According to Klein, the program found that the total cost of care was 32% less than traditional hospital care and the mean length of stay about 30% shorter. In addition, a study by Leff and colleagues noted a reduced incidence of hospital-acquired complications (9% vs. 24%).
COVID: A perfect storm
Similar to IU Health, many health systems were challenged to respond to COVID-19 by finding alternative care sites. The result included spikes in the popularity of home-based care models and the establishment of interest groups such as the Hospital at Home User Group. These groups support innovation worldwide and advocate for U.S. private and public payers to create a reimbursement mechanism for this care model.
According to Clarke and colleagues, these advocacy efforts led the Centers for Medicare and Medicaid Services (CMS) to approve an Acute Care at Home Waiver in November 2020 to allow inpatient-level payment for care delivered at home. The waiver divides participants into two categories: those with hospital-at-home experience (managed at least 25 patients) and those who have never implemented a program.
CMS Acute Care at Home Waiver
The Centers for Medicare and Medicaid Services (CMS) established the following waiver, which establishes conditions for providing acute care at home.
- Provide or contract for the following services: acute care services at home including pharmacy, infusion, respiratory care, diagnostics, monitoring vitals twice daily, transportation, food services, durable medical equipment, physical, occupational, and speech therapy, and social work and care coordination
- Meet minimum required frequency of personnel visits, defined as:
- Once-daily physician/advanced practice provider can be remote after an initial in-person visit
- Once-daily in-person or remote RN visit
- Twice daily in-person visits by either RN or paramedics
- Meet minimum emergency response times for each patient of 30 minutes. This can be provided by 911 or emergency paramedics
- Use a published set of selection criteria
- Agreement to track the following three metrics
- Metric 1: Unanticipated mortality during the acute episode of care
- Metric 2: Escalation rate
- Metric 3: Volume of patients treated in the program
- Agreement to establish local safety committee review dedicated to this program to review above metrics
- Agreement to use InterQual, Milliman, or another accepted patient leveling process to ensure that only patients requiring an acute level of care are treated in this program
CMS approved IU Health to use the waiver, which includes a twice-daily, in-person visit requirement. However, IU Health’s program blends daily or as-needed virtual and in-person care. Outcomes indicate the effectiveness of this model for patients with COVID-19, so IU Health hasn’t submitted payment under the waiver.
After 2 years of strategy meetings to determine whether IU Health should implement hospital-at-home, the COVID-19 pandemic hit all 16 hospitals. As a result, the health system turned to leaders on April 2, 2020, to develop a program to help alleviate the stress of the surge. Via multidepartment partnerships, IU Health increased the already established remote patient monitoring (RPM) nurse team capacity to 24/7, provided hospitals with home monitoring equipment to give to patients before discharge, and created twice-daily interdisciplinary huddles to discuss patient needs. In an incredible feat of cooperation and innovation, the hospital-at-home program received its first patient on April 9, 2020.
How does IU Health’s program work?
During the initial phase of the program, RPM nurses performed vital sign assessments three times per day and reached out to patients based on predetermined alerts. They contacted hospitalist physicians for clinical support and in the event of abnormal vital signs.
In November 2020, IU Health transitioned clinical support to a team of four NPs, with hospitalist physicians at two hospitals as backup support. The NPs staffed the program from 6:00 am to 11:00 pm with on-call shifts from 11:00 pm to 6:00 am. IU Health RPM nurses conducted daily virtual visits and home health nurses provided in-home visits as needed. RPM nurses escalated care to the NPs for guidance, at pre-determined alerts, and for adjustments to the plan of care. (See RPM nurse competencies.)
RPM nurse competencies
Nurses who serve on the Indiana University Health remote patient monitoring (RPM) team must possess the following competencies:
- Awake prone positioning
- Incentive spirometry
- Telemonitoring equipment education
- Oxygen weaning protocol
- Escalation criteria
- Nutrition for COVID-19
- Centers for Disease Control and Prevention and Indiana Department of Health COVID-19 Education
After a few weeks of caring for complex COVID-19 patients in the hospital-at-home program, the clinical leadership team adjusted the NP scope, requiring NPs to complete a history, physical, and discharge summary for all patients. The history and physical provide documentation for a seamless patient transition from the hospital to hospital-at-home and create a baseline reference for team members. To ensure continuity of care, the NPs copied the primary care provider on the discharge summary.
In January 2021, the program added part-time physician’s assistants (PAs) and a hospitalist medical director. In addition, it transitioned advanced practice providers (APPs), including NPs and PAs, to the virtual hospitalist team. The team holds two daily huddles. The morning huddle consists of all care team stakeholders and leadership; the evening comprises APPs and virtual hospitalists.
APP escalation
Adding full-time APPs to the program ensured real-time provider access for RPMs and consistent communication and care delivery to improve patient safety. The ability of APPs to engage patients in virtual visits allows the team to successfully manage more complex problems. It’s essential to keeping readmissions to less than 6%.
Foundational program workflow components include the following:
- Patients leave the hospital with a kit that contains an iPad, blood pressure cuff, pulse oximeter, and thermometer.
- Patients requiring oxygen receive a tank from the hospital, and the durable medical equipment provider delivers a concentrator to the patients’ homes.
- The patient and their home caregiver receive an overview of program expectations and monitoring equipment instruction.
- RPM nurses monitor patients virtually three times a day to ensure a safe home recovery.
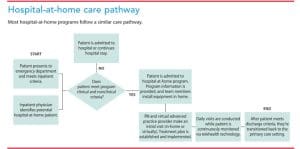
- The team provides in-home visits as needed (IU Health doesn’t use the CMS waiver). (See Hospital-at-home care pathway.)
Challenges
Challenges for the IU Health hospital-at-home program include patient complexity, rapidly changing admission criteria, and caregiver expectations. These unique challenges have encouraged health system flexibility regarding access and healthcare provision. (See Challenges and highlights.)
Challenges and highlights
The Indiana University Health hospital-at-home program continues to tackle challenges related to patient complexity, changing admissions criteria, and caregiver expectations.
Patient complexity
Patients with COVID-19 frequently have comorbid conditions and experience social factors that make their care complex.
Solution: Provide wrap-around services, including social work.
Rapidly changing admissions criteria
Program admission criteria have evolved over time based on new information, which created knowledge gaps between inpatient and outpatient providers.
Solution: The interprofessional team created opportunities for feedback from hospital colleagues. Standardized provider-to-provider handoffs closed gaps between inpatient and outpatient teams.
Caregiver expectations
Caregiver understanding of patient needs has been an ongoing challenge. Patients with COVID-19 who transition into the program are considered hospitalized patients who require high-level care.
Solution: Improved education for patients and caregivers has marginally improved caregiver understanding, but efforts for further improvement continue.
Highlights and key findings related to the success of the program include the following:
Operational highlights
- Daily huddles with rapid patient monitoring (RPM) nurses, advanced practice providers (APPs), and hospital leaders for patient handoffs
- Continuous criteria adjustments for patients accepted into the program
- Quality oversight steering committee
- Escalation processes
- Wrap-around services (social work, therapy, and lab draws)
- RPM nurse-to-patient ratio 1:10
- 24/7 RPM, APP, and hospitalist coverage
Key findings
- Over 1,500 patients with COVID-19 cared for (April 2020 to January 2022)
- Readmission rate within 30 days was 4.3% (April 2020 to July 2021)
- Emergency department utilization within 14 days was 3.8% (April 2020 to July 2021)
What’s next for IU Health?
Since its launch, the hospital-at-home program has cared for more than 1,500 patients. As COVID-19 cases began to wane, IU Health shifted its focus to delivering a program to replace a typical hospital stay and deliver complete care in the home. IU Health is still early in this journey. Compared to the number of patients with COVID-19, the number of patients with other conditions (such as heart failure, pneumonia, urinary tract infection, and cellulitis) is low. IU Health continues to investigate shifting its focus to a treatment-based model in which the program offers a suite of services and medications. Any patient who can benefit may then be referred to the program.
Future of hospital-at-home model
As more health systems and payers express interest in delivering hospital-level care at home, the prevalence of this model will increase. Fee-for-service and stringent Medicare definitions of hospital vs. home healthcare create reimbursement challenges that prevent some systems from investing in these types of programs. However, as more health systems partner with payers to create value-based care arrangements, delivering more cost-effective, high-quality care outside the hospital becomes even more attractive.
The authors work at Indiana University Health in Indianapolis. Shelly Maersch is executive director of home health and hospice. Rob Schrock is clinical director of advance practice providers. Victoria Bratcher is executive director of population health operations.
References:
Banes TJ. ‘Hospital at home’ patient: ‘They spoiled me. I couldn’t have asked for better care.” Indiana University Health. April 22, 2021.
Centers for Medicare and Medicaid Services. Acute hospital care at home resources.
Clarke DV, Newsam J, Olson DP, Adams D, Wolfe AJ, Fleisher LA. Acute hospital care at home: The CMS waiver experience. NEJM Catalyst. December 7, 2021. catalyst.nejm.org/doi/full/10.1056/CAT.21.0338
Klein S. “Hospital at home” programs improve outcomes, lower costs but face resistance from providers and payers. The Commonwealth Fund.
Leff B, Burton L, Mader SL, et al. Hospital at home: Feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann Intern Med. 2005;143(11):798-808. doi: 10.7326/0003-4819-143-11-200512060-00008


















