
Education, training, and collaboration are keys to success.
Takeaways:
- RN leaders can facilitate education initiatives and geriatric training for long-term care (LTC) staff.
- RN leaders can initiate evidence-based practice processes and lead staff in measuring outcomes.
- RN leaders can collaborate with LTC staff by valuing their input for quality improvement projects.
- RN leaders can support and recognize the entire team by advocating best practices.
Long-term care (LTC) facilities are faced with many care hurdles, including a growing geriatric population, complexities associated with chronic conditions, and an insufficient workforce. Evidence-based practices (EBPs) facilitated by nurses can bridge the gap between current and best practices and help LTC facilities overcome these hurdles.
EBP involves problem-solving that merges nurses’ clinical expertise with evidence derived from systematic research to improve patient care (in conjunction with patients’ values and preferences) and outcomes. Implementing EBP can be a challenge for any healthcare system because of limited resources, time, and knowledge. However, LTC facility challenges are unique and require innovative strategies to overcome them.
Challenges to EBP implementation
Challenges to EBP implementation in LTC facilities include resident and workforce characteristics, lack of geriatric training and EBP education, and staff turnover.
 LTC resident and workforce characteristics
LTC resident and workforce characteristics
 LTC resident and workforce characteristics
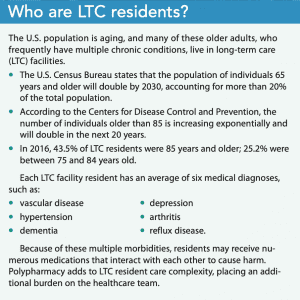
LTC resident and workforce characteristicsOlder adults residing in LTC facilities are likely to have multiple chronic conditions, such as dementia, physical disabilities, and decreased functional status. These needs significantly increase the burden on staff to provide quality care and assist with activities of daily living. (See Who are LTC residents?)
According to the Centers for Disease Control and Prevention, LTC facilities have fewer trained personnel than other healthcare agencies, and unlicensed staff provide most of the direct care. In 2016, 971,100 full-time equivalent staff worked in 15,600 U.S. LTC facilities. Of these workers, more than 60% were unlicensed personnel (certified nurse aides/assistants, medication technicians, and other aides) and 22.3% were licensed practical nurses (LPNs). The small percentage of RNs who work in LTCs (about 12% of the staff in most LTC facilities) primarily provide indirect care, such as staff supervision and care coordination; certified nursing assistants (CNAs) provide most of the direct care. This workforce pattern poses a challenge to implementing evidence-based care because although LPN and CNA training may include basics of elder care, these healthcare workers receive insufficient EBP training.
Lack of geriatric training and EBP education
Caring for older adults requires geriatric training and knowledge of the intricacies of age-related changes, as well as how those changes affect chronic conditions, medication metabolism, and functional status. Despite this need, many RNs, CNAs, LPNs, and other healthcare providers don’t have specific geriatric training and are inadequately prepared to care for LTC residents. In addition, LPN programs are 1 year and CNA programs are completed within 12 weeks (about 75 hours of didactic education and 16 hours of clinical training), leaving no time for EBP education. This limited preparation is insufficient for delivering safe evidence-based care for medically complex older adults.
Staff turnover
Turnover rates in LTC facilities are high and have been attributed to low wages, inadequate staffing, and poor relationships with supervisors. Limited staffing further compromises quality care for a fragile dependent population, adversely affecting resident outcomes. Research by Trinkoff and colleagues directly links high CNA turnover to increases in pressure injuries, pain, and urinary tract infections; high RN turnover doubles pressure injury rates. Turnover ultimately results in fewer caregivers taking on more responsibilities, leading to poor care quality in some settings.
Strategies for implementing EBP
Overcoming challenges to implementing EBP in LTC facilities requires making a commitment to staff training, getting staff buy-in, addressing high turnover rates, enlisting advance practice registered nurses (APRNs), and collaborating with other LTC facilities and academic institutions.
Make a commitment to geriatric and EBP training
Staff development sessions for CNAs positively impact resident outcomes, especially for pain, falls with injury, weight loss, use of psychoactive medications, and depressive symptoms. Staff education facilitated by nurse leaders should include both informal and formal learning opportunities tailored to meet individual facilities’ needs. Nurses can begin by encouraging staff (as well as families and residents) to visit hign.org/consultgeri/elearning a clinical nursing website established and maintained by the Hartford Institute for Geriatric Nursing. All content (including podcasts, geriatric protocols, evidence-based assessment instruments, and continuing education opportunities) on the site can be accessed for free.
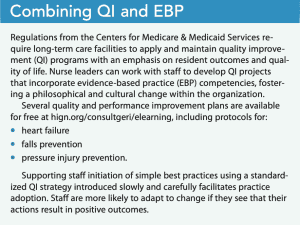
Short educational programs for staff can be offered each month to address topics such as mealtime difficulties, fluid overload, frailty, or sleep problems. Varying learning styles can be supported by providing access to audio, visual, and printed material. A selected monthly topic can be discussed at staff meetings, at team huddles, or in lunch-and-learn sessions. Nurse leaders also can ask family members if they have topics they’d like to review and discuss with staff. Quality improvement (QI) projects are another way to integrate EBP. (See Combining QI and EBP.)
Get staff buy-in
Successfully integrating EBP requires staff buy-in. Allowing staff to contribute to change at every opportunity empowers them to identify problems, share ideas for practice change initiatives, and improve their clinical practices. When nurse leaders introduce EBP, they must acknowledge and value input from direct care staff who spend the most time with residents and are most likely to recognize new concerns—such as skin changes, weight loss, cognitive changes, or deficits—and can identify opportunities for an EBP project.
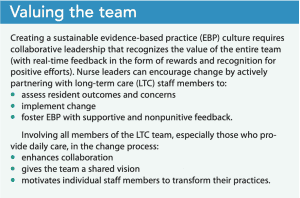 Nurse leaders also can involve QI champions who help evaluate intervention effectiveness and provide direction to improve outcomes. QI champions assist in the EBP process, integrating research evidence with clinical expertise and resident input. They facilitate EBP implementation on their units, lead QI teams, encourage staff in QI initiatives, and advocate for practice change. Designating CNAs or LPNs as QI champions validates their importance and demonstrates the belief that they can help improve care quality and resident outcomes. Partnering staff who have QI experience with new hires creates an opportunity for sharing and mentoring. Forming EBP teams, led by a QI champion, can inspire staff to make practice changes and influence EBP adoption. (See Valuing the team.)
Nurse leaders also can involve QI champions who help evaluate intervention effectiveness and provide direction to improve outcomes. QI champions assist in the EBP process, integrating research evidence with clinical expertise and resident input. They facilitate EBP implementation on their units, lead QI teams, encourage staff in QI initiatives, and advocate for practice change. Designating CNAs or LPNs as QI champions validates their importance and demonstrates the belief that they can help improve care quality and resident outcomes. Partnering staff who have QI experience with new hires creates an opportunity for sharing and mentoring. Forming EBP teams, led by a QI champion, can inspire staff to make practice changes and influence EBP adoption. (See Valuing the team.)
Address high turnover and job dissatisfaction
Reducing turnover rates ensures care continuity, ultimately improving resident outcomes, and may improve EBP success. CNA satisfaction is tied to a number of factors including adequate staffing, residents’ overall satisfaction, and management. Nurse leaders can help ensure adequate staffing levels by remaining supportive of CNA staff, demonstrating empathy, and modeling collegial and respectful relationships. CNAs who believe that supervisors are their advocates are more likely to remain in their jobs. Supportive leaders who empower CNAs, giving them greater autonomy in decision-making, will enhance job satisfaction and lower turnover rates.
Enlist APRNs
APRNs employed in LTC facilities can enhance EBP implementation by providing clinical expertise, helping the LTC team reflect on clinical issues, and encouraging clear communication between residents, families, and the LTC team when developing and implementing care plans and practice changes. They also can serve as mentors and leaders, conduct education and training activities, and participate in QI projects. According to Rantz and colleagues, APRNs working in LTC facilities improve care quality, decrease hospital admissions and readmissions, improve health outcomes, and decrease spending.
Partner with other LTC facilities and academic institutions
LTC facility leaders should consider collaborating with other LTC facilities to share best practices, education initiatives, clinical concerns, QI projects, clinical guidelines, and the latest evidence-based clinical recommendations to encourage EBP uptake and sustainability. Learning about successful QI projects and EBP initiatives can help staff reflect on their current practices and consider trying what has worked for others.
Some LTC facilities can collaborate and draw support from academic institutions. Collaborating with faculty on research initiatives might expose LTC staff to research and encourage doctor of nursing practice students interested in LTC to initiate QI projects. Academic partnerships can foster access to the EBP process and guide staff in interpreting the literature and applying standardized guidelines.
Initiate, support, and reward
Healthcare systems benefit when they deliver evidence-based care that improves residents’ health outcomes. Implementing EBP into LTC can be challenging, but it’s possible when leaders initiate, support, and reward positive practice changes that lead to improved resident outcomes.
Jill Brennan-Cook is an assistant clinical professor of nursing at Duke University School of Nursing in Durham, North Carolina.
References
Applequist J, Miller-Day M, Cronholm PF, Gabbay RA, Bowen DS. “In principle we have agreement, but in practice it is a bit more difficult”: Obtaining organizational buy-in to patient-centered medical home transformation. Qual Health Res. 2017;27(6):909-22.
Centers for Medicare & Medicaid Services. Medicare and Medicaid Programs; Reform of requirements for long-term care facilities. Final rule. Fed Regis. 2016;81(192):68688-872. govinfo.gov/content/pkg/FR-2016-10-04/html/2016-23503.htm
Chamberlain SA, Hoben M, Squires JE, Estabrooks CA. Individual and organizational predictors of health care aide job satisfaction in long term care. BMC Health Serv Res. 2016;16(1):577.
Harris-Kojetin L, Sengupta M, Lendon JP, et al. Long-term care providers and services users in the United States, 2015-2016: Analytical and epidemiological studies. Vital Health Stat 3. 2019;(43):i-vii, 1-78. cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf
Harris-Kojetin L, Sengupta M, Park-Lee E, et al. Long-term care providers and services users in the United States: Data from the National Study of Long-Term Care Providers, 2013-2014. Vital Health Stat 3. 2016;(38):x-xii, 1-105.
Higuchi KS, Edwards N, Carr T, Marck P, Abdullah G. Development and evaluation of a workshop to support evidence-based practice change in long-term care. J Nurses Prof Dev. 2015;31(1):28-34.
Hunt SR, Corazzini K, Anderson RA. Top nurse-management staffing collapse and care quality in nursing homes. J Appl Gerontol. 2014;33(1):51-74.
Kim SC, Stichler JF, Ecoff L, Brown CE, Gallo AM, Davidson JE. Predictors of evidence-based practice implementation, job satisfaction, and group cohesion among regional fellowship program participants. Worldviews Evid Based Nurs. 2016;13(5):340-8.
Lalic S, Sluggett JK, Ilomäki J, et al. Polypharmacy and medication regimen complexity as risk factors for hospitalization among residents of long-term care facilities: A prospective cohort study. J Am Med Dir Assoc. 2016;17(11):1067.e1-e6.
Matthews M, Carsten MK, Ayers DJ, Menachemi N. Determinants of turnover among low wage earners in long term care: The role of manager-employee relationships. Geriatr Nurs. 2018;39(4):407-13.
Moore KL, Boscardin WJ, Steinman MA, Schwartz JB. Patterns of chronic co-morbid medical conditions in older residents of U.S. nursing homes: Differences between the sexes and across the agespan. J Nutr Health Aging. 2014;18(4):429-36.
Ortman JM, Velkoff VA, Hogan H. An Aging Nation: The older population in the United States. Current Population Reports. U.S. Census Bureau; 2014. census.gov/prod/2014pubs/p25-1140.pdf
Plaku-Alakbarova B, Punnett L, Gore RJ. Nursing home employee and resident satisfaction and resident care outcomes. Saf Health Work. 2018;9(4):408-15.
Popejoy L, Vogelsmeier A, Galambos C, et al. The APRN role in changing nursing home quality: The Missouri Quality Improvement Initiative. J Nurs Care Qual. 2017;32(3):196-201.
Rantz MJ, Popejoy L, Vogelsmeier A, et al. Impact of advanced practice registered nurses on quality measures: The Missouri Quality Initiative Experience. J Am Med Dir Assoc. 2018;19(6):541-50.
Rowe JW, Berkman L, Fried L, et al. Preparing for better health and health care for an aging population: A vital direction for health and health care. National Academy of Medicine. September 19, 2016. nam.edu/preparing-for-better-health-and-health-care-for-an-aging-population-a-vital-direction-for-health-and-health-care
Trinkoff AM, Han K, Storr CL, Lerner N, Johantgen M, Gartrell K. Turnover, staffing, skill mix, and resident outcomes in a national sample of US nursing homes. J Nurs Adm. 2013;43(12):630-6.
Trinkoff AM, Storr CL, Lerner NB, Yang BK, Han K. CNA training requirements and resident care outcomes in nursing homes. Gerontologist. 2017;57(3):501-8.
Wang KN, Bell JS, Chen EYH, Gilmartin-Thomas JFM, Ilomäki J. Medications and prescribing patterns as factors associated with hospitalizations from long-term care facilities: A systematic review. Drugs Aging. 2018;35(5):423-57.
Woo K, Milworm G, Dowding D. Characteristics of quality improvement champions in nursing homes: A systematic review with implications for evidence-based practice. Worldviews Evid Based Nurs. 2017;14(6):440-6.
Zhang Y, Punnett L, Gore R. Relationships among employees’ working conditions, mental health, and intention to leave in nursing homes. J Appl Gerontol. 2014;33(1):6-23.


















1 Comment.
This is a great lead to address LTC staff and empowerment. As a new staff development coordinator with a certification in Wholistic Nurse coaching. The EBP concept is very important, as the current frontline staff who have been loyal express that support because of staffing with travelers and high turnover rates have left them diminished. The follow up and support of some of the leaders in place who have not been kept accountable and have been managing resist the culture change. This is a sad event for the patients. My focus is to mentor and support the front line with education as well as provide a team culture with coaching. This is a challenge because of the lack of staff and also, boundaries as well as fear of losing more staff. This comment “I know that they are not doing the job but there is no one to perform the job”. How do you write up employees that have been in that environment without respect.