
With focus and accountability, quality improvement is possible.
Takeaways
- Using traditional strategies, a hospital unit’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) responsiveness domain scores were inconsistently achieving the VBP threshold.
- Using the 4 Disciplines of Execution (4DX) model provided a forward-thinking strategy to improve staff responsiveness and increase patient satisfaction.
- Using the 4DX principles to guide nursing practice, a practice improvement project resulted in improved HCAHPS responsiveness domain scores.
At University of Florida Health Jacksonville, which has received American Nurses Credentialing Center (ANCC) Magnet® recognition, exceptional patient care is an organizational goal. However, 7 North (7N), a 26-bed medical progressive care unit within the hospital, was experiencing inconsistencies in the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) staff responsiveness domain. To address this issue, the unit developed a performance improvement (PI) project using an innovative approach.
Finding opportunity
Under the Centers for Medicare & Medicaid Services’ (CMS’) Value-Based Purchasing (VBP) Program, 7N’s VBP threshold for 2017 was set at 65.96% (the 50th percentile among all hospitals that participate in HCAHPS reporting). Data from January to December 2017 showed a 12-month top box percentage (the percentage of patients who answer “always”) responsiveness average of 60.97%. One month it was as low as 0. To help improve responsiveness, the 7N nurse manager and clinical quality nurse leader (CQNL) designed a PI project using the 4 Disciplines of Execution (4DX), a nontraditional model that focuses on one or two important goals. (See 4DX: A model for change.)
Choosing the goal
In February 2018, the 7N leadership team collaborated with staff to choose a wildly important goal (WIG) that would produce the greatest impact. Baseline unit data revealed an average 6-minute call light response time. Nearly 27% of patient calls exceeded a 5-minute wait time, contributing to the low responsiveness domain score. Using a shared decision-making councils to promote joint accountability and responsibility to improve HCAHPS scores, these data were presented to 7N’s unit practice council (UPC), which chose staff responsiveness as the WIG for the PI project. Using correlation analysis as the project methodology, the UPC postulated that purposeful hourly rounding and call light responses would correlate with improved patient satisfaction, which, in turn, would improve staff responsiveness scores.
Changing the culture
In March 2018, the unit identified two lead measures: a 90% purposeful hourly rounding adherence rate and an average 5-minute or less call light response time. A literature review indicated that no standard exists for acceptable call light response time, so the 5-minute standard was adopted based on a 2017 Lean Six Sigma Green Belt project initiated by the organization’s quality management department.
The 4 Disciplines of Execution (4DX) model—which focuses on a wildly important goal (WIG), lead measures, a compelling scoreboard, and accountability cadence—can be used by healthcare organizations and teams to improve quality measures. The examples are from University of Florida Health Jacksonville.
WIG
Using the WIG concept allows a team to focus on one or two important goals that will make the most difference to the organization or unit. Rather than asking, “What’s most important?” the team asks, “If everything else remained the same, what one change would make the biggest impact?” Energy and attention are required to balance executing the WIG and maintaining daily job responsibilities.
7 North (7N) WIG:
•Staff responsiveness
Lead measures
Many organizations focus on lag measures (goals already achieved). Lead measures, which are predictive and can be influenced by the team, show what’s likely to be achieved.
7N lead measures:
•Purposeful hourly rounding
•Call light response time
Compelling scoreboard
The only way a team will know if it’s achieving its goals is for everyone to know the “score” (how the team is progressing on its path to improvement). Sharing this information publicly keeps everyone accountable and engaged.
7N scoreboard:
•Publicly posted overall unit and individual staff lead measure adherence rates
Accountability cadence
This discipline sets a rhythm for accountability and momentum toward achieving the WIG. Team members meet regularly to report on action steps, review the scoreboard, and plan for next steps.
7N accountability cadence:
•Weekly huddles to inform staff of unit and individual
Purposeful hourly rounding
At the beginning of the PI project, staff members performed purposeful rounding every hour during shifts per organization policy; RNs rounded on even hours, and patient care associates rounded on odd hours. However, no measures were in place to ensure rounding timeliness and focus. In April 2018, to validate rounding adherence, the UPC and leadership team implemented daily audits using the nurse call system. 7N’s CQNL, a master’s-prepared RN with PI methodology expertise in patient outcome improvement, spearheaded the auditing process.
The audit was based on a report of data obtained from the nurse call system, which includes a badge worn by each staff member to monitor location and amount of time spent in each location. The report compiled an overall purposeful hourly rounding compliance percentage by using the initial visit end time and the follow-up visit start time to calculate “minutes in between presences.” For example, entering 120 minutes as the time between presences informs the nurse call system that each staff member should perform purposeful hourly rounds at least every 2 hours. If a nurse exits a patient’s room at 1200, the nurse call system knows that he or she should reenter the room for purposeful hourly rounding at 1400. Each day, staff members received an email with a letter-grade scorecard for their purposeful hourly rounding compliance. (See Keeping score.) Once a week, the CQNL calculated 7N’s overall purposeful hourly rounding adherence by di
Every week, the average purposeful hourly rounding score for each staff member and the overall unit-based average were displayed on the unit. Publicly displaying this information recognized staff members who were meeting or exceeding the 90% compliance goal and those who were performing below the standard. It also initiated some healthy competition that resulted in increased rounding by low performers. Within 90 days, staff were exceeding the 90% adherence rate, and hourly rounding was ruled out as an area of concern.
Call light response
7N maintained an average weekly call light response time of 5 minutes or less. However, to reduce a false sense of accomplishment, the unit shifted focus to assessing patient calls that exceeded the 5-minute standard. The CQNL reviewed data from the nurse call system to determine variables affecting response times, and a detailed daily workflow report identified patients who waited longer than 5 minutes. The report—which displays facility, unit, date, patient, room location, start time, stop time, category, response time, request type, stop reason, and request—allows the CQNL to observe individual patient request workflows active during a specific date range. 7N’s nurse manager and CQNL opted to exclude variables such as rapid responses, code blues, and staffing challenges from the report.
In conjunction with the workflow report, a nurse call system staff locator report was used to identify staff member location and preassigned alternate staff members at the exact time a patient called for assistance. Identifying staff members who weren’t adhering to the 5-minute response time lead measure presented an opportunity for real-time education and coaching. In addition, individual emails were sent to staff to remind them of expectations.
Measuring success
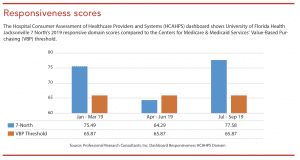
Focusing on lead measures (90% purposeful hourly rounding adherence rate and answering patient call lights within 5 minutes) resulted in improved patient satisfaction. From March to December 2018, the average call light response time declined from 6 minutes to 3 minutes, and waiting times longer than 5 minutes decreased from 27% to 17%. The HCAHPS responsiveness domain scores ranged from 68.75% to 87.5%, remaining at or above the VBP threshold of 65.87%, except for August and September, which fell below the threshold because of nonadherence to the organization’s policy of ensuring all patient calls are appropriately paged to nursing staff using the call system. These gains have been sustained for the majority of 2019. (See Responsiveness scores.)
Validating change
7N’s PI project created a unit culture focused on teamwork and accountability rather than division of labor. Using the 4DX model, existing technology, and enhanced staff accountability, 7N improved patient satisfaction with no additional cost to the organization. Ultimately, the project validated that with sufficient support and guidance, improving patients’ perceptions of care quality is attainable.
Danielle T. Jones is the 7 North medical progressive care unit clinical quality nurse leader at the University of Florida Health Jacksonville.
References:
Centers for Medicare & Medicaid Services. The Hospital Value-Based Purchasing (VBP) Program. November 19, 2019. cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/HVBP/Hospital-Value-Based-Purchasing.html.
McChesney C, Covey S, Huling J. The 4 Disciplines of Execution: Achieving Your Wildly Important Goals. New York: Free Press; 2016.
Murray A, Mohamed M. Bridging the gap between strategy and execution. April 28, 2015. kmworld.com/Articles/Columns/The-Future-of-the-Future/Bridging-the-gap-between-strategy-and-execution-103363.aspx

















