
Commitment and persistence pay off in improved outcomes.
Takeaways
- Lessons learned and best practices from 10 years of Joint Commission inpatient diabetes certification.
- Changing inpatient culture and behaviors in diabetes care takes repeated data collection and evaluation, automated solutions when possible, and perseverance.
- Embedding guidance in the electronic health record and at the point-of-care minimizes uncertainty and errors and standardizes procedures to match current guidelines.
Diabetes quality improvement (QI) in an inpatient academic hospital setting can be challenging because of communication gaps among staff, pre-established mealtime delivery schedules, complex patient populations, provider turnover, and competing staff demands. At the VA Northeast Ohio Healthcare System, we’ve maintained 10 years inpatient diabetes certification from The Joint Commission. What follows are our lessons learned and best practices for a diabetes QI project at your organization.
QI team
Start an organization-wide diabetes QI initiative by creating an engaged interprofessional team of leaders from nursing, medicine, QI, and nutrition. To expedite protocol design, implementation, and maintenance, consider including endocrinology, pharmacy, and information technology staff on the team. For smaller units, begin with a group of interested nurses, nurse educators, and other leaders. Look for people who are passionate about improvement, dedicated to spearheading change, and able to persevere through challenges. To foster good team communication across departments, schedule regular team meetings. Initially, our team met monthly; we now meet quarterly.
QI goals
The Joint Commission’s Certificate of Distinction for Inpatient Diabetes Care requires establishing four QI goals every 2 years. Choose goals that are measurable, meaningful, and manageable (for example, glycemic control). To ensure success, involve stakeholders in goal selection.
Goals not achieved in a 2-year Joint Commission evaluation cycle can be continued until they’re completed. Use frequent plan, do, study, act cycles to help generate improvement in selected measures. In our organization, QI was implemented on all acute medical and surgical units as well as intensive care units (ICUs).
Glycemic control
Improving glycemic control lowers hospital complication rates in general medicine and surgery patients. The American Diabetes Association recommends an inpatient blood glucose target range of 140 to 180 mg/dL for most patients. During hospitalization, managing glycemic variation can be challenged by underlying illnesses, corticosteroid use, unpredictable test scheduling, changing diet orders, and patient eating patterns. Confidence with insulin dosing and administration varies among nurses, providers, and trainees, and competing demands interfere with coordinated timing of blood glucose checks, insulin administration, and meal-time delivery schedules.
Achieving outcomes
The intent of establishing goals to ensure glycemic control is to reduce the incidence of hypoglycemia and hyperglycemia. Here are strategies we used to achieve our goals.
Hypoglycemia
Hypoglycemia mitigation is a safety priority for all organizations, and evaluating adherence to hypoglycemia protocols is an excellent starting point for reducing incidence. For example, monitoring hypoglycemia events, timely blood glucose value rechecks, and event charting can prompt needed re-evaluation of insulin dosing. In response to gaps in hypoglycemia blood glucose recheck rates at our hospital, the QI team created a hypoglycemia documentation template and laminated pocket cards with guidance tips to be placed at the point of care to ensure all nurses understand the correct procedures. We used unit data to benchmark progress; deeper dives into the timing of mealtime blood glucose checks, insulin administration, and meal delivery helped us evaluate safe practices to reduce hypoglycemia.
Hypoglycemia prevention also requires evaluating insulin prescribing protocols, timing meals in relation to insulin testing and administration, coordinating nothing by mouth (NPO) orders with antiglycemic medications, and titrating antiglycemics for persistent lows. For example, an endocrinology service review of our insulin prescribing orders, hypoglycemia rates, and patient demographics (frail elderly and comorbidities such as chronic kidney disease) prompted changes in calculating the daily dose of insulin, including routinely reducing the total dose in patients with chronic kidney disease. The endocrinology service also provided guidance on insulin prescribing that we embedded into the electronic health record (EHR), providing a valuable resource for residents who rotate through the system.
Since implementing these changes, hypoglycemia rates have remained stable and severe hypoglycemia rates have declined overall. In addition, nurse hypoglycemia recheck rates of within 30 minutes of the first low reading have remained consistent (ranging from 72% to 92% and averaging 82.25%).
Hyperglycemia
We also embedded guidance for preventing, monitoring, and treating hyperglycemia into the EHR. For example, nurses may be reluctant to administer basal insulin to an NPO patient or a patient with poor oral intake or whose point-of-care glucose is low to normal, yet in some cases patients should still receive insulin. The EHR now includes orders to notify the provider if basal insulin is held during NPO status to discourage nurses from making a unilateral decision.
Another guidance requires notifying the provider if two consecutive blood glucose values are > 300 mg/dL. In ICUs (but not on other units), this would prompt nurses to obtain an insulin infusion order. In our organization, nurse discharge case managers round with providers and notify them of blood glucose outliers obtained via automated daily reports. We also use a computerized dashboard to track persistent hyperglycemia. The team physician monitors the dashboard daily and then discusses options for glycemic control improvement with the patient’s care provider.
Our overall rates of severe hyperglycemia are low and relatively stable. Audit and feedback on treatment and documentation have gradually reduced hyperglycemia in these acutely ill patients.
Action steps
As part of our QI project, we took steps to address competing demands, cultivate diabetes champions, provide education, and develop point-of-care guidance.
Competing demands
We’ve taken several steps to address our healthcare teams’ competing demands. For example, when an urgent issue distracts nurses from rechecking a low blood glucose, nursing assistants perform the 15-minute recheck. Nurse discharge case managers monitor hypoglycemia and hyperglycemia on their units and notify providers on rounds to ensure persistent glucose variations aren’t overlooked. Process flow charts are used to discover best practice obstacles. For example, we discovered that hypoglycemia treatments (glucose gel) located in centralized automatic dispensing cabinets were too far away from medication carts and patient bedsides for efficient treatment. Glucose gel is now placed in each of the medication carts. And we remedied a lack of glucometer docking stations by installing additional units.
Diabetes champions
Cultivating diabetes champions—including discharge nurse case managers, unit-based clinical nurse specialists, nurse managers, assistant nurse managers, and dietitians—who regularly interact with staff providers and patients encourages best practice outcomes. Nurse managers include hypoglycemia and hyperglycemia safety in shift safety huddles, and a short briefing on diabetes education is sent to each nurse manager to disseminate to charge nurses for safety huddles. (See In the huddle.) Including glycemic competencies for all nursing staff reinforces the diabetes inpatient improvement culture.

Education
Busy nurses may not always be able to provide patients with diabetes survival skills training, especially during off-shifts or on weekends. This important education is augmented by dietitians and via patient education videos on individual room televisions. The videos cover various diabetes-related topics, including blood glucose meter use, insulin injection, sick-day treatment, nutrition, and hypoglycemia and hyperglycemia.
Point-of-care guidance
Point-of-care guidance, either embedded in the EHR or strategically posted at the bedside, has proved invaluable to medical and nursing staff. EHR-embedded guidance is useful when providers write orders, when nurses read and verify orders, and when nurses document care notes. Examples of automated provider embedded guidance include insulin prescribing protocols and an updated A1c order on admission if the latest results are reported more than 3 months ago.
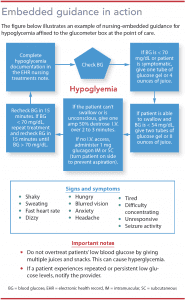
Point-of-care guidance ensures staff follow crucial diabetes safety parameters and standardizes care across the organization. It also provides just-in-time training for new staff and those who are absent on education days. And it acts as reminder in response to information overload. (See Embedded guidance in action.)
Drive change
Our diabetes management changes have increased patient satisfaction. In postdischarge phone surveys conducted in 2019, 98% of patients with diabetes expressed satisfaction with how their condition was managed while they were hospitalized.
Experience has taught us that changing inpatient culture and behaviors in diabetes care takes repeated data collection and evaluation, automated solutions when possible, and perseverance. Data and results are shared with frontline staff to demonstrate the need to change processes and to celebrate QI. Embedding guidance in the EHR at the point of care minimizes uncertainty and errors and standardizes procedures to match current guidelines. Competing demands will always be a challenge for busy hospitals, but enlisting engaged and persistent staff will ultimately drive change in diabetes QI efforts.
The authors work at VA Northeast Ohio Healthcare System. Sharon A. Watts is the national nursing services advisor, metabolic syndrome and diabetes. Drina R. Nemes is a clinical nurse specialist. Timothy Davian, Jr. is a diabetes nurse educator. Amanda L. Pensiero is a staff hospitalist.
References:
American Diabetes Association. Economic costs of diabetes in the U.S. in 2017. Diabetes Care. 2018;41(5):917-28.
American Diabetes Association. Diabetes care in the hospital: Standards of medical care in diabetes—2019.Diabetes Care. 2019;42(Suppl 1):S173-81.
Engle M, Ferguson A, Fields W. A journey to improved inpatient glycemic control by redesigning meal delivery and insulin administration. Clin Nurse Spec. 2016;30(2):117-24.
Lampe J, Penoyer DA, Hadesty S, Bean A, Chamberlain L. Timing is everything: Results to an observational study of mealtime insulin practices. Clin Nurse Spec. 2014;28(3):161-7.
Mann D. Creating a Lean Culture: Tools to Sustain Lean Conversions (3rd ed.). Boca Raton, FL: Routledge; 2014.
Neelon L, Basawil K, Whitney L, Kneblewicz E, Watts SA, Miller DM. Critical care nurse-led quality improvement hyperglycemia reduction initiative. J Nurs Care Qual. 2019;34(2):91-3.
Schneider AL, Kalyani RR, Golden S, et al. Diabetes and prediabetes and risk of hospitalization: The Atherosclerosis Risk in Communities (ARIC) Study. Diabetes Care. 2016;39(5):772-9.
Watts SA, Nemes D. Best practice nursing management of nosocomial hypoglycemia: Lessons learned. MEDSURG Nursing. 2018;27(2):98-102.


















1 Comment.
Dear Ms. Gelinas,
In the article titled “10 Years of Inpatient Diabetes Certification— Lessons Learned,” authored by Ms. Sharon Watts and published in the January 2020 edition of American Nursing Journal, the implementation of the Diabetes Quality Improvement (QI) program for the Veteran Affairs Northeast Ohio Healthcare System has proven vital to the betterment of patient health outcomes. Congratulations to the facilitators and initiators of this program on having been able to maintain the inpatient diabetes certification from the Joint Commission for over 10 years. Ms. Watts mentioned her article that challenges medical staff face in providing adequate care for diabetic patients are communication gaps among staff members; predetermined mealtimes and variations in meal delivery time; the complexity of comorbidities that the aging population now face; and prioritizing staff demands during their designated shifts. For these reasons, the QI program developed by the author not only addresses these challenges, but is a proactive catalyst improvement in health.
The updates to the electronic health record system was a great improvement for those familiar with EHR systems. Through no fault of nursing and medical staff, we see that most medical personnel have full inpatient panels in need of a variety of medical services. The addition of the electronic health record check system is an added measure that enables us to notify staff members if they are going to perform an action that is detrimental to a patient’s health. When this program was implemented in the VA hospital inpatient setting, reduced incidence rates of hypoglycemia was reported in patients with diabetes. This strategic move helps identify whether insulin doses are correct for the patient who may be dealing with other chronic health conditions. Also, allowing certified nursing assistants to perform patient blood glucose rechecks is critical to efficiently utilizing staff’s time. Giving nursing assistants additional responsibilities helps instil pride and duty in their work. The added responsibility of patient care in trusted staff members can help nurses perform actions that may be more urgent depending on the patient loads
This QI program is of vital importance to the health and well-being of patients dealing with diabetes and other comorbidities. I hope the staff is incredibly proud of this accomplishment; and that other medical institutions will catch the vision and begin working on establishing similar programs to improve the health outcomes of their patients.
Sincerely,
Richard Del Pino
Nursing Student
SUNY Downstate College of Nursing