A nurse-led care transformation model.
Takeaways:
- The nursing profession must take a lead role in the transformation of care delivery.
- Success can be achieved by clinical nurses observing care delivery across all settings, identifying opportunities for improvement, implementing care transformation developing partnerships across settings, and creating integrated plans of care.
- The evolution of fee-for-service to value-based payment models impacts the support and financial feasibility of patient-centered care transformation.
As we endure the ongoing effects of the COVID-19 pandemic, one thing has become abundantly clear. Healthcare delivery in the United States isn’t equitable and frequently not available to high-risk populations. Healthcare delivery has been transforming from a fee-for-service to a value-based care model, which focuses on the Triple Aim and aims to improve the patient experience and population health while also decreasing cost. These goals can be achieved by creating a continuum of care across a patients’ life, delivered by integrated teams focused on health promotion and disease prevention.
At Southwestern Vermont Medical Center, a community hospital in Bennington that has received Magnet® designation five times, clinical nurse specialists (CNSs) were in danger of losing their hospital-based positions because of decreasing inpatient admissions. To address this issue, nurses were encouraged to seek solutions to improve care coordination for patients with chronic disease who were high-cost healthcare users. What began as an experiment to save a critical skillset for the health system soon became a pathway to transform care delivery focused on a value-based payment model.
Inspired care
Nurses at the organization recognized the need for a bridge between primary care providers and care delivered across all other settings. Each CNS (now transitional care nurses or TCNs) partnered with four primary care practices, identifying high-risk patients. As the TCNs navigated across the care continuum, observing the lived experience of patients and their families, they identified gaps and opportunities for improvement. They witnessed the role of social determinants of health, lack of adequate individualized patient education, and misunderstandings about medication and symptom management.
For the past 7 years the TCNs have assembled teams of healthcare profession partners who care for friends and neighbors in innovative ways to create the Inspire Model. This step-by-step approach to implementing value-based care focuses on improving the patient experience and population health at a decreased cost. This model can be implemented in your organization, too. (See Get inspired.)
Get inspired
The Southwestern Vermont Medical Center approach to population health can be summed up in one word: Inspire.
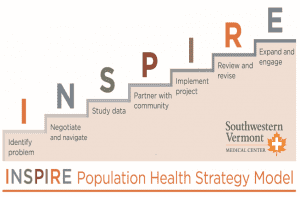
Identify the problem
Start your organization’s process transformation by identifying potential issues in care delivery. Consider deploying nurses to observe care delivery across the care continuum in a service line. What patient population will be your focus and what targeted area will you seek strategies to improve? Convene a meeting with relevant stakeholders to discuss ideas, suggestions, concerns, and perceived barriers. Include providers, front line staff, and community partners in these discussions. Review the literature to find successful strategies and narrow your area of focus.
Negotiate and navigate
Work closely with the executive management team to assess the payment model and contractual agreements. Partner with the finance team to assist with baseline metrics, identify senior leaders and physician champions, and seek opportunities to educate staff. Consider options for funding new positions, including grant writing, redeployment, re-training, and staff development.
Who are the providers, community agencies and partners, and ancillary professionals you may need on your team? Involve them early in the process to build trust and avoid barriers, overlap, and competition.
Study data
Review existing baseline data related to your potential project. Consider future metrics (quantitative or qualitative research, baseline measurements before and after implementation, rates of emergency department [ED] or hospital utilization, serial lab results) to evaluate project success. Review metrics found in your literature review that may be used for benchmarking and identify methods to collect evidence of patients demonstrating improved chronic disease management. Patient or staff surveys can demonstrate results efficacy, patient and staff satisfaction, and quality of life.
Partner with the community
Population health can only be achieved when a continuum of care is created across all settings by building relationships, and developing overlapping systems, and fostering communication, understanding, and respect. Outreach as you help patients navigate across settings is key to success and one of the most rewarding aspects of the project. It also can become one of the biggest challenges, prolonging your timeline for implementation. Community partners will prove pivotal to success, so leave titles at the door.
Implement the project
Confirm funding sources for the program, create and design workflows, identify team members, hire staff, create onboarding education and training, and consider routine interdisciplinary meetings. Consulting with providers to discuss the vision and progress and get their buy-in and support is crucial to avoiding interference and missteps.
Review and revise
Establish systems to evaluate and measure success. Maintain an open mind, ask for regular feedback, and welcome constructive criticism. Consider all feedback by team members, gathering objective data as a basis for decision making. This will enhance the creation of a committed, strong, and successful team.
Expand and engage
Communicate with patients, family members, providers, and front line workers to share results and seek their input. New programs frequently identify other issues that need to be addressed to improve population health. Share results with providers, partners, the community, and the media. Keep in mind that funding programs sometimes leads to eliminating other budget items vs. advocacy for increased funds. Instead, advocate for increased funds and seek donors with an interest in improving population health.
Creating a community care team
As an ED nursing director, I was concerned about patients with mental health and substance use disorders who used the department frequently (50 to 400 visits per year). We performed complex medical workups (blood work, computed tomography scans, ECGs, and spinal taps) to assess symptoms of chest pain, abdominal pain, and severe headaches with no concrete findings. The staff were frustrated and didn’t feel equipped and competent to solve the problem, and we weren’t addressing underlying issues, including access to food, shelter, compassion, mental healthcare, and addiction treatment. I was particularly concerned about the lack of empathy displayed by many staff. We took steps to increase staff education on mental health and substance use but saw little improvement. That’s when we initiated the community care team (CCT) project.
Action steps
We began the project by conducting a literature review, meeting with stakeholders, and partnering with Middlesex Hospital to develop a strategy. We then hired an ED patient advocate to help build trusting relationships. The community care team included the ED staff, a social worker, mental health support services, addiction counselors, home care liaisons, and case managers. Other CCT members came from a local homeless shelter and soup kitchen, economic services, the housing administration, and workforce development.
Outcomes
The CCT partnered with the hospital compliance officer and attorney to create a patient consent form that allowed us to share information at monthly team meetings. Initial results included a 40% reduction in avoidable ED visits and increased referrals for services. The CCT’s efforts also resulted in several patient success stories and many others avoiding death, disability, and unnecessary healthcare costs. (See CCT outcomes.)
CCT outcomes
In a value-based payment model, the goal is to decrease cost while also improving quality outcomes and patient experience. All partners who participated in the Southwestern Vermont Health Care community care team (CCT) were engaged and excited about the results, improved relationships, and increased integrated and coordinated care delivery.
- In 2020, the CCT created integrated plans of care for 120 patients. Pre-CCT intervention, that patient cohort had 497 emergency department (ED) visits compared to 340 post-intervention.
- Total charges for ED care pre-intervention totaled $661,441. Average total cost based on statewide payment data decreased by $217,602, recognizing that many of these patients didn’t have insurance.
- Many CCT patients found housing, employment, mental health counseling, addiction support, access to healthcare, and healthcare coverage.
We replicated the program to create two pediatric CCTs (birth to age 6 and ages 7 to 19). The team includes pediatric providers, home care and hospital nurses, social workers, case managers, community partners and agencies, as well as school clinicians, counselors, and teachers.
Payment challenges
Across the United States, health systems function with multiple contractual agreements ranging from traditional fee-for-service models based on volume to value-based models focused on quality outcomes, or some combination of the two. This represents a challenge to chief financial officers (CFOs) and executive management teams. Because nurses lead care transformation, we must improve our understanding of payment models, including the penalties for hospital readmissions, potential lack of reimbursement for unnecessary care, inappropriate care, and medical or surgical errors. Consider the opportunities in your health system to decrease avoidable care by increasing teamwork and care coordination. Make this a goal as you initiate this work.
The TCNs’ work at Southwestern Vermont Medical Center decreased admissions and ED visits for patients who partnered with them. Unfortunately, the transition from fee-for-service to more value-based contracts took longer than anticipated, which presented some challenges. The CCT’s success negatively impacted healthcare revenue, despite being the right thing to do for patients. This resulted in several conversations between the TCN leader and the CFO. We pursued grant funding to support pilot programs that demonstrated success and as soon as data were available indicating program success, efforts were made to remove nonessential budget items. In addition, the TCN explained to the CFO the reputational benefit of delivering quality and safe care. Examples of successful cases also helped, as did discussing the experiences of the CFO’s family and friends in other locations who could have benefitted from transitional care. (See Population health programs.)
Population health programs
Southwestern Vermont Medical Center offers these programs to assist with care transitions.
| Program | Target population | Interventions and outcomes |
| Transitional care nursing | · People with chronic diseases · High-risk patients discharged from ED | · Nurses partner with patients/families to review medication management, chronic disease education, and symptom management and to navigate referrals to resources. · 54.5% reduction in hospitalizations 6 months after intervention. · 39% reduction in hospitalization 1 year after TCN involvement. |
| Transitional care social work | · People with chronic diseases · High-risk patients discharged from ED | · Dedicated social worker assists people with solutions to complex needs throughout transitions of care. |
| Community care team | · People with mental health disorders, substance use disorders, and unmet needs related to social determinants of health | · ED patient advocate navigates and connects people to community resources and support. · Monthly meeting of community resources to create integrated care plan after consent obtained. · CCT has resulted in a 30% decrease in ED use for this population with improved quality of life and access to appropriate assistance, housing, and treatment for substance use disorders. |
| Integrated diabetes education | · People with pre-diabetes, type 1, 1.5, 2, and gestational diabetes | · Diabetes educators embedded in primary care facilitate patient-centered goal identification to improve health, increase activity, and improve blood glucose control. · Patients have achieved an average 11% reduction in their A1C as well as a 20% reduction in hospitalizations. |
| Pediatric community care team | · At-risk children (from birth to age 19 years) in need of medical, emotional, and social supports | · Family advocate in pediatric office engages with families to identify needs, access community resources, and facilitate appropriate referrals. · Monthly meeting with community partners to create integrated care plan after consent obtained. |
| Palliative care | · People with pending end-of-life challenges who might benefit from improved symptom management and emotional support | · Transitional palliative care nurses partner with providers, attending daily interdisciplinary rounds, PCP practices, and SNFs to increase appropriate referrals and access to services. · Palliative care program has decreased hospitalization and ED visits for those with chronic illness while improving satisfaction of symptom management. |
| Pulmonary rehabilitation with maintenance | · People with chronic lung disease | · The goal is to improve quality of life, maintain function, and use self-management techniques such as exercise and behavior changes. |
| INTERACT® | · SNF residents | · INTERACT empowers nursing assistants to speak up about changes in patient conditions, prompting evaluation by RN/provider to decrease SNF ED visits and hospital admissions/readmissions |
| Financial counselor | · People with financial needs, concerns, or questions | · Available financial counseling improves satisfaction with access to assistance for patients without insurance or those experiencing financial struggles. |
| YSBIRT | · Youth in pediatrics, OB/GYN, express care and the ED | · Screening of youth 12-24 years. · Access to immediate intervention and referrals. · Over 700 screens have been completed since program implementation in May 2019. |
CCT = Community care team, ED = emergency department, INTERACT = Interaction to Reduce Acute Care Transfers, PCP = primary care provider, SNF = skilled nursing facility, TCN = transitional care nurse, YSBIRT = Youth Screening, Brief Intervention, and Referral to Treatment
Doing better
Florence Nightingale paved the way for our profession when her Notes on Nursing were published in 1859. She was ministering to the people who needed help the most with no consideration of race, age, sex, or neighborhood. We can and must do better to decrease cost, while improving quality outcomes, patient and care provider satisfaction, and the health of everyone we serve.
Nursing, as a profession, has a unique opportunity right now to use its knowledge, expertise, and influence to chart a course for the future of healthcare delivery as outlined in the Future of Nursing 2020-2030. It may be the highlight of your career.
Billie Lynn is a clinical nurse specialist and value-based care/population health consultant at Southwestern Vermont Health Care in Bennington and co-founder of the Association of Chronic and Complex Care Nurse Navigators.
References
Berwick DM, Nolan TW, Whittington J. The triple aim: Care, health, and cost. Health Aff. 2008;27(3):750-69
Centers for Disease Control and Prevention. Medication safety basics. cdc.gov/medicationsafety/basics.html
Hostetter M, Klein S, McCarthy D. Vermont’s bold experiment in community driven health care reform. Commonwealth Fund. May 10, 2018. commonwealthfund.org/publications/case-study/2018/may/vermonts-bold-experiment-community-driven-health-care-reform
Institute for Healthcare Improvement. Triple aim for populations. ihi.org/Topics/TripleAim/Pages/default.aspx
Institute for Healthcare Improvement. How to improve: Science of improvement: Testing changes. ihi.org/resources/Pages/HowToImprove/ScienceofImprovementTestingChanges.aspx
Ndugga N, Artiga S. Disparities in health and health care: 5 key questions and answers. Kaiser Family Foundation. May 11, 2021. kff.org/racial-equity-and-health-policy/issue-brief/disparities-in-health-and-health-care-5-key-question-and-answers/
Naylor MD, Aiken LH, Kurtzman ET, Olds DM, Hirschman KB. The care span: The importance of transitional care in achieving healthcare reform. Health Aff. 2011;30(4):746-54. doi:10.1377/hlthaff.2011.0041
Shah R, Press VG, Huisingh-Scheetz M, White SR. COPD readmissions: Addressing COPD in the era of value-based health care. Chest. 2016;150(4):916-26. doi:10.1016/j.chest.2016.05.002
Sheff A, Park ER, Neagle M, Oreskovic NM. The patient perspective: Utilizing focus groups to inform care coordination for high-risk Medicaid population. BMC Res Notes. 2017;10:315. doi:10.1186/s13104-017-2638-1
York R, Kaufman K, Grube M. Where have all the inpatients gone? A regional study with national implications. Health Affairs. January 6, 2014. healthaffairs.org/blog/2014/01/06/where-have-all-the-inpatients-gone-a-regional-study-with-national-implications