
Advocate for data sharing that optimizes patient care and outcomes.
Takeaways:
- Interoperability occurs when two or more systems exchange health information.
- Nursing is the vanguard of patient-centered care, but nurses haven’t been supported in their efforts to help healthcare organizations meet interoperability goals.
- Front-line nurses must advocate for interoperability of all health data to ensure patient-centric, not technology-centric solutions.
Maria Nestor*, an unaccompanied elderly patient with shortness of breath, arrives at the emergency department by ambulance. She’s new to the community and health network. Her entire health history is sequestered miles away in another health system’s electronic health record (EHR). As the transferring nurse admits Ms. Nestor to the unit, the emergency nurse remarks that the patient’s health history is a “black hole.”
What are the opportunities and gaps in this scenario? Despite the Centers for Medicare and Medicaid Services (CMS) incentive program for and commitment to interoperability (the ability of one EHR system to electronically communicate a patient’s health history to another system using common terms), limitations prevent some essential information from being shared from one setting to another and even between providers within the same setting. EHRs weren’t designed to connect with each other and especially not across the care continuum. Even when systems do connect, the terms used to describe patient assessments and information may vary by organization. Subsequently, nurses and other providers lack access to key information, which may compromise care.
System and terminology interoperability across healthcare systems can alleviate information gaps at the point of care. National, regional, and state-based health information exchanges work to share data between EHRs across the care continuum, and although work continues and progress is being made, significant gaps, barriers, and limitations pose challenges. The solutions to this issue are complex, but frontline nurses can engage with their healthcare system to educate and create awareness of the importance of nursing-related data to breaking down the barriers to interoperability.
Unfortunately, nurses haven’t always been supported in their efforts to help healthcare organizations meet interoperability goals. The price of this omission includes diminished patient-centered care. It also doesn’t recognize the distinct value of nursing’s contributions to patient outcomes. Interoperability is complex and nuanced, but understanding its value to nursing practice and patient-centered care can help nurses advocate for it to improve care and outcomes.
Interoperability and its trajectory
A patient’s health history is complete when providers have full access to prior health concerns and care utilization across settings. Evidence demonstrates that the lack of a health history can compromise care delivery, and the absence of interoperable EHRs is a primary contributor. Interoperability supports efficiency, avoids redundancy, and improves safety. It also facilitates clinical decision-making and support, improving patient outcomes.
The Federal Health Information Technology for Economic and Clinical Health Act required the implementation of a nation-wide, standardized framework for exchanging health information and guiding EHR use. The act requires healthcare organizations to adopt an EHR with meaningful use criteria. Adoption implies actual EHR use in patient care; meaningful implies using the EHR’s full potential.
To stimulate EHR adoption and meaningful use, federal legislation links financial incentives (bonus payments and penalties) to clinical decision support, order entry, and other EHR features. Additional legislation requires vendors to demonstrate functionality for patient-centered care within the EHR. The Office of the National Coordinator for Health Information Technology and CMS recently established standards for structured data transfer to promote interoperability, creating an EHR certification. Healthcare providers can demonstrate quality care and be reimbursed by exchanging data via a CMS-certified EHR.
Organizations also must adopt standardized application programming interfaces to help individuals securely and easily access their electronic health information using smartphone applications. Although many healthcare organizations use EHRs and can exchange patient information, several challenges (including an opt-out option, cost, data sharing hesitancy, and privacy and security concerns) have prevented the intent of the federal mandates from being fully achieved, leaving many healthcare professionals unable to access useful data across the care continuum.
Current state of interoperability
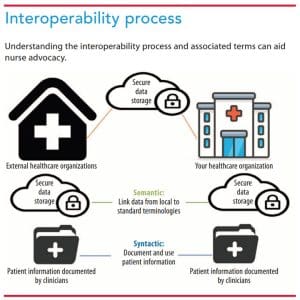
Effective patient data exchange in a complete, consistent format requires multiple people and steps as well as syntactic and semantic interoperability. Healthcare organizations achieve syntactic interoperability when they transfer and communicate data using existing standards and tools. Semantic interoperability, the transfer and exchange of data that both systems understand in the same way, proves more challenging because most nursing documentation resides in nonstandardized formats. Both syntactic and semantic interoperability must be achieved to reach federal goals. (See Interoperability process.)
Healthcare uses structured and unstructured data. Structured data are documented in a discrete location and coded with common metrics and meanings and then mapped to an existing, interpretable standard terminology to support semantic interoperability. Examples of structured data include vital signs (such as blood pressure and heart rate), medications (including dosages and administration frequency), and drop-down box responses (for example, breath sounds and neurologic assessment). Structured data across different EHR systems with the same definitions and structures facilitate interoperability.
Unstructured data are seen in free text notes. These data aid communication and documentation of information that doesn’t fit into a box or checklist, but nurses and other providers use various terms to describe the same symptom or phenomena. For example, the color of a patient’s urine may be described as “dark amber” by one clinician, “yellowish-brown” by another, and “dark yellow” by a third. Without standardized nursing language and nomenclature used across EHRs, semantic interoperability can’t exist.
Each documentation entry is influenced by the clinician’s training, experience, organizational norms, and cultural perspective. Without human interpretation and manual computer coding (or being able to use natural language processing, which requires substantial data analysis), unstructured data aren’t readily usable, which means professional nursing insight isn’t easily accessed. Unstructured data can be shared, but because it doesn’t have inherent, computable meaning, the recipient may be limited in how they use it.
Interoperability and patient-centered care
Nursing practice remains underrepresented in healthcare quality measurement programs. We’re challenged by a lack of interoperability and inconsistent use of standardized terminology in documentation notes. For example, “rattles” may be used in one hospital to describe breath sounds and “rales” used in another. Historically, leadership roles and committees (including informaticists, but rarely frontline nurses) influence documentation terminology. And because nursing documentation predominantly resides in unstructured free text fields that are less quantifiable than providers’ (which include procedure codes or quality measures), nurses’ value and contribution to patient outcomes are difficult to fully measure and evaluate. It is important to note that many quality measures (including CMS Core measures), nurse-sensitive outcomes, and Magnet® designation are based on nursing documentation; however, because it’s difficult to measure nursing care processes, it’s difficult to demonstrate the value of nursing.
Structured data primarily reflect a patient’s status at a moment in time, but unstructured data delineate a nurse’s assessment, including suspicions, insights, and critical thinking. Because documenting verbally communicated information can be difficult and important information frequently is documented as unstructured data, many aspects of nursing assessment may be lost or forgotten. Nurses manage hundreds of thousands of data points per shift. Unfortunately, the challenge of capturing and capitalizing on all of them results in an inability to determine a clear link between nursing care and patient outcomes. When healthcare team members can’t readily use part of the patient’s story (the unstructured data), care quality suffers. Effective interoperability, including the use of unstructured data, would bring all data points together and illustrate the impact of nursing on patient-centered outcomes.
Advocating for interoperability
Nurses can take several steps to advocate for patient-centric rather than technology-centric EHR interoperability. First, advocate for access to important patient data outside of your organization and request that all of it, including patient-generated data (shared via a patient’s own devices, such as a smartwatch), be based on standardized terminology that’s mapped to discrete documentation fields within the EHR and healthcare databases.
Offer your nursing expertise to aid decisions about the technology used in your organization and what data will optimize patient care. Nurses use data-rich technologies—EHRs, telemetry, vital sign devices, and infusion pumps—to provide patient-centered care. Volunteer to be a super-user (someone who takes an active role in the design, implementation, teaching, troubleshooting, and support during launch) when technology decisions are being made.
Propose to your unit and hospital leadership that nursing executives observe workflow and technology use at the point of care to understand opportunities and barriers associated with a lack of usable, standardized data. This approach helps nurse executives and frontline nurses align around common goals and patient outcomes to advocate for interoperable technology. It also facilitates identification of metrics (improved safety, early detection of complications, efficiency) for implementation, which can be foundational in developing an outcomes scorecard for the impact of a technology on nursing practice and patient care. In addition, this process creates top-down support for frontline nurse representation on implementation teams.
If a nursing informatics practice council doesn’t exist in your organization, collaborate with nurse informaticists and nursing leadership to develop one with frontline nursing representation on technology implementation teams. This council should include representatives from all nursing units with a rotating schedule. These roles support technology implementation, system design, testing, and go-live steps.
Share responsibility
When nurses advocate for strategies to aid interoperability, open and collaborative relationships form. Optimized care requires that everyone share responsibility for improved patient outcomes through interoperability.
*Name is fictitious.
Ronda Hughes is interim director of the masters in nursing informatics program and associate professor at the University of South Carolina in Columbia. Vallire Hooper is associate professor, associate dean of research and scholarship, and director of the PhD program at East Tennessee State University College of Nursing in Johnson City. Rosemary Kennedy, PhD, RN, MBA, FAAN, is chief executive officer of eCare Informatics in Frazer, Pennsylvania. Mollie R. Cummins is a professor, Jon M. Huntsman Presidential Chair, and adjunct professor of biomedical informatics at the University of Utah College of Nursing in Salt Lake City. Eileen T. Lake is Jessie M. Scott Term Chair in Nursing and Health Policy and professor of nursing and sociology at the University of Pennsylvania School of Nursing in Philadelphia. Jane M. Carrington is an associate professor, Dorothy M. Smith Endowed Chair, and co-director of the Florida Blue Center for Health Care Quality at the University of Florida College of Nursing in Gainesville.
References
Centers for Medicare and Medicaid Services Promoting interoperability programs. January 11, 2022.
HIMSS. Interoperability in healthcare.
Office of the National Coordinator for Health Information Technology. 2020-2025 Federal health IT strategic plan. August 21, 2021.
Office of the National Coordinator for Health Information Technology. Health IT legislation. June 8, 2021.
Office of the National Coordinator for Health Information Technology. Meaningful use. October 22, 2019.
Office of the National Coordinator for Health Information Technology. ONC’s Cures Act Final Rule. October 2020.
Šendelj R. Information technology and information management in healthcare. Stud Health Technol Inform. 2020;274:139-58. doi:10.3233/SHTI200674

















